Lab 21 navigation
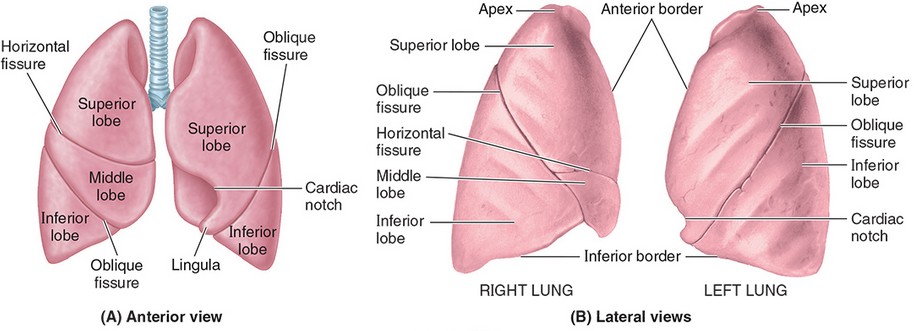
External Anatomy of the Lungs
Apex and base
Lobes
Left lung = superior (upper) and inferior (lower)
Right lung = superior (upper), middle, and inferior (lower)
Surfaces = costal, mediastinal, and diaphragmatic
Anterior and inferior borders
In left lung: Cardiac notch and lingula
Oblique fissure in both lungs; horizontal fissure in right lung only
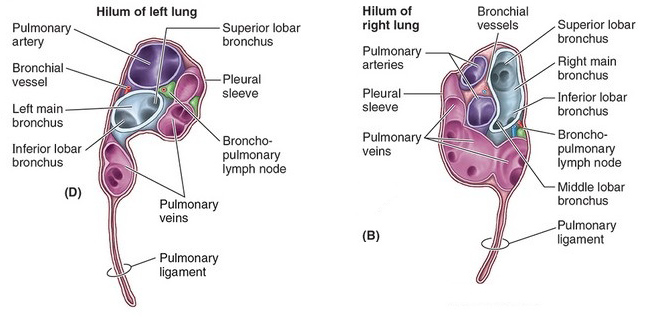
Hilum and root of lung (what is the difference?)
Visceral pleura
Pulmonary ligament
Root of the Lung
Examine the hilum of both lungs to identify structures comprising the root of the lung.
Locate:
Pulmonary artery (branched in the right lung)
Pulmonary veins (superior and inferior)
Main bronchus
Right main bronchus divides into an interlobar and a superior lobar bronchus before entering the right lung
Bronchopulmonary (hilar) lymph nodes
Question
Compare and contrast right and left lungs—are the arrangements of structures in the lung roots different?
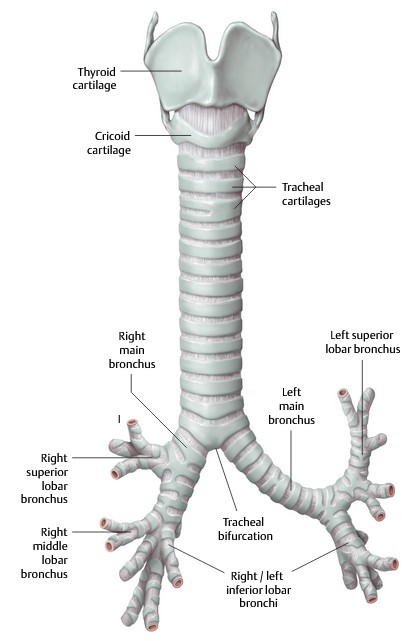
Tracheobronchial Tree
The trachea is the continuation of the airway distal to the larynx. It begins at C-6 and descends in the neck anterior to the esophagus. It is easily palpable just above the suprasternal notch, due to its “C”-shaped rings of cartilage that support the airway and prevent its collapse. The posterior surface that faces the esophagus has no cartilage—thus it is flat. The trachea passes through the superior thoracic aperture to enter the mediastinum.
Just below the level of the sternal angle (~ T-5), the trachea bifurcates into left and right main bronchi (sometimes called the primary bronchi).
- The tracheal bifurcation is marked internally by a ridge called the carina, which is from the Latin word for “keel” (the long piece of wood or metal along the center of the bottom of a boat).
Clinical correlation
A foreign body inhaled into the trachea is more likely to enter and lodge in the right main bronchus, rather than the left, because it is wider and more vertical—thus, more directly in line with the trachea.
The main bronchi branch into lobar bronchi. These are the secondary branches of the bronchial tree.
- The right lung has three = superior (upper), middle, and inferior (lower) lobar bronchi. After the superior lobar bronchus has branched, the remaining main stem bronchus is called the interlobar bronchus. The middle and inferior lobar bronchi branch from the interlobar bronchus.
The left lung has two = superior (upper) and inferior (lower) lobar bronchi.
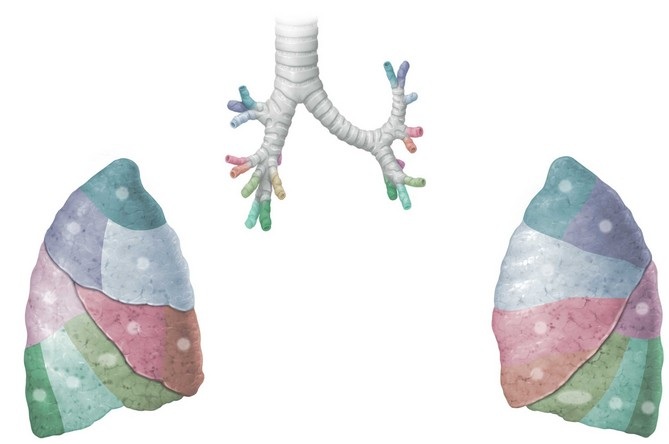
Third-order bronchi are called segmental bronchi. Each lung has roughly 10 of these air tubes. Segmental bronchi aerate specific regions of the lung known as bronchopulmonary segments (Figure 33).
Pleura and Pleural Cavities
We covered the pleura and pleural cavities way back in Lab 8, but it never hurts to review!
Visceral pleura snuggly invests the external surface of the lung—in fact, it is the shiny outer layer of the organ itself.
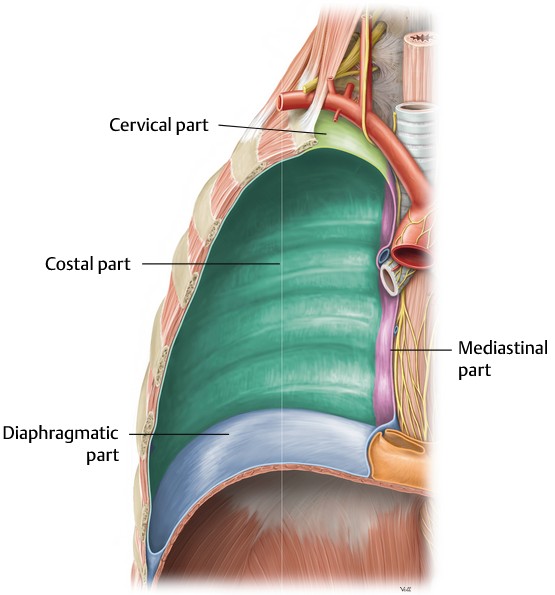
Parietal pleura lines the internal surface of the thoracic wall, the lateral side of the mediastinum, and the superior surface of the diaphragm. Thus, the parietal pleura faces the lungs and visceral pleura. The parietal pleura has four named parts:
-
-
- Costal
- Mediastinal
- Diaphragmatic
- Cervical (also called the cupula)
-
Question
The parietal pleura is associated with the body wall, while visceral pleura is associated with an organ (the lung). Which parts of the nervous system innervate each? How would pain be perceived from each? How does the development of these structures relate to their difference in innervation?
The pleural cavity is the potential space between the layers of visceral and parietal pleurae. It contains a thin layer of pleural fluid that lubricates the pleural surfaces.
-
-
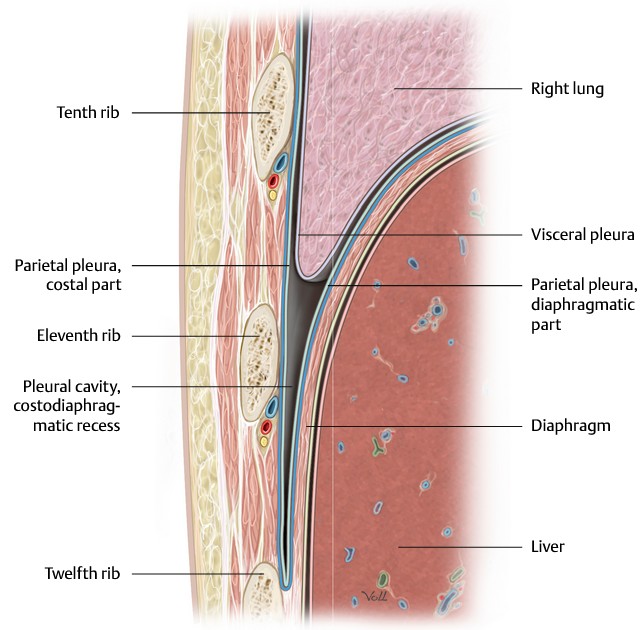
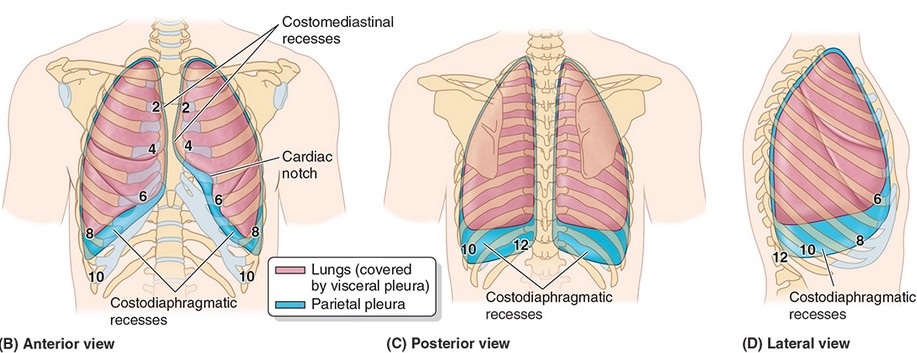
- During expiration, the lungs (covered in visceral pleura) do not fully fill the inferior-most part of the pleural cavities. These potential spaces below the lungs are called the costodiaphragmatic recesses. They form “gutters” around the edges of the domes of the diaphragm. When the lungs expand during inspiration, they slide down into the recesses (see Figure 35).
-
Clinical correlation
The costodiaphragmatic recesses appear on chest X-rays as sharp downward indentations where the diaphragm meets the chest wall. Clinicians call these the “costophrenic angles.” Gravity can cause fluid, pus, or blood to collect in the costodiaphragmatic recesses. On X-rays, this produces “blunting” of the costophrenic angles.
Question
During quiet respiration, there is about a two-rib gap between the inferior border of the lung and the inferior most extent of the costodiaphragmatic recess. Why would this be important information to the clinician?
Clinical correlation
Trace the cervical pleura upwards—note that it extends into the root of the neck.
What is the name of the depression on the surface of the body wall, superior to the clavicle? The cervical pleura and apex of the lung are deep to this landmark.
Do you recall the clinical significance of this relationship?


