


In this case study
Overview
Antimicrobial resistance (AMR) occurs when disease-causing germs are able to withstand the killing or suppressing power of antimicrobial medicines. This phenomenon increases the global infectious disease burden and puts a strain on health systems.
This course builds on the Antimicrobial resistance (AMR), part 1, course, which provides an overview of the basic principles and drivers of antimicrobial resistance (AMR) and describes the impact of AMR on individuals, society, health systems, and global health goals. It presents some of the global health community’s e”orts to contain it, including work supporting the Global Health Security Agenda.
This course, Antimicrobial Resistance Part 2, explains in detail the major factors that contribute to the development and spread of AMR and the interventions available to address these factors. This course also discusses antimicrobials and vaccine development, the impact of globalization and societal shifts on AMR, and international strategies for containing AMR. Because AMR cuts across and a!ects human, animal, and environmental health, a One Health approach is fundamental to tackling this growing global threat; this course emphasizes that multisectoral connection.
Glossary Term:
antimicrobial resistance
Did you know?
A major study published in The Lancet in 2022 showed that an estimated 1.27 million deaths worldwide were directly attributable to antimicrobial-resistant bacterial infections in 2019, which was more than the deaths caused by either HIV/AIDS or malaria.
Source: Antimicrobial Resistance Collaborators 2022
Organization
This course contains six sessions:
- Introduction to the causes and containment of AMR
- Prescribing and dispensing antimicrobials
- Patients and the general community
- Health systems and regulatory issues
- Hospitals
- Containing AMR in the global community
Session 1 lists the major factors contributing to AMR and the broad areas of intervention recommended to contain it.
Sessions 2 to 5 present in detail how various stakeholders, structures, and systems contribute to AMR and what interventions are available to tackle them.
Session 6 briefly offers how globalization and societal shifts have affected AMR, the development of new antimicrobials, and the need for coordination and coalition at international, regional, and local levels to fight the extreme public health threat that AMR poses.
Before we dive into Session 1 and the major contributing factors, let’s consider two scenarios to show when antimicrobials work and when antimicrobial resistance occurs.
Scenario 1: When antimicrobials work
Only 85 years ago, many common infections caused severe illness and death because we had no effective medicines to treat them. The development of antimicrobials, such as penicillin, revolutionized the treatment of these infections.
Consider the following case scenario from 1940, a time before antibiotics were widely available and before AMR was a global health concern.
In 1940, a 43-year-old police officer had pus discharge from his face, scalp, and both eyes, which had originated from a sore at the corner of his mouth a month earlier. The primary cause of infection was Staphylococcus aureus, with secondary involvement of Streptococcus pyogenes. A course of sulfapyridine, a sulfa drug, was administered for a week, but brought no improvement.
After a month, doctors decided to make incisions in multiple abscesses on his face and scalp. Unfortunately, this resulted in the patient developing an arm abscess, which discharged pus. He soon developed a general infection of the left eye, and his eye was later removed. After one more month, all of his incisions were producing pus and his lungs began filling with pus.
As a last resort, doctors tried penicillin and noted a striking improvement after 24 hours. The patient no longer had pus discharge from his scalp, and the pus formation in his right eye was reduced.
Source: Adapted from Abraham et al. 1941
Glossary Term:
Staphylococcus aureus Abscess
Streptococcus pyogenes
Scenario 2: When antimicrobial resistance occurs
Jamel Sawyer was a healthy college football player whose unusual back pain progressed to paralysis and a fever of 106°. After being rushed to the hospital, an MRI revealed an abscess on his spinal cord. In intensive care for several weeks, the doctors tried multiple antibiotics, including several typically reserved as a last resort. Although none seemed to work, eventually Jamel recovered, though he lost the use of his legs. He continued to study for his degree while working to walk again and sharing his story of methicillin-resistant Staphylococcus aureus (MRSA). Though he was lucky to survive, his family suffered a tremendous financial burden. One study suggests that a MRSA infection can extend a hospital stay by 23 days and increase costs by $61,000.
This second scenario describes the harmful effects of contracting an infection that is resistant to multiple antibiotics, a phenomenon that is observed in many parts of the world today. Antimicrobial agents that brought remarkable improvement for the patient in the first scenario had no effect on this patient, whose infection resisted various antibiotics available on the market; this scenario emphasizes the need to intensify efforts to support the development of new antibiotics, while working to slow the emergence and spread of resistance.
Medicines that have been taken for granted for the last 85 years are losing their effectiveness due to antimicrobial resistance, leaving fewer and fewer options.
Sources: Adapted from The Pew Health Group, 2010; Anderson et al., 2009.
Glossary Term:
Bronchoscopy Lung infiltrates
Necrotizing pneumonia Respiratory distress
Did you know?
Staphylococcus aureus is a leading cause of health care-associated infections. Methicillin-resistant Staphylococcus aureus (MRSA) is a dreaded type of Staph infection that is resistant to many antibiotics. In 2019, MRSA caused more than 323,700 infections and 10,600 deaths and cost $1.7 billion in health care costs in the United States.
Source: CDC 2019
Highlight
WHO recently launched a “taskforce of survivors of AMR” to champion an increase in advocacy and help provide a human face to AMR. At the inaugural meeting in October 2023, the taskforce discussed ways to share patients’ stories effectively and set priorities for patient advocacy.
Source: WHO 2023d
Now let’s dive into Session 1: Causes and containment of antimicrobial resistance.
New page
Causes and containment of antimicrobial resistance
Welcome to the first session: Causes and Containment of Antimicrobial Resistance.
Minimizing the impact of AMR requires an understanding of the underlying factors that contribute to its development and spread. Multiple interrelated factors influence and facilitate the development and spread of AMR, which affects not only the human sector but also the animal and environmental sectors. Due to these complex factors, interventions also require a multi-faceted approach.
-
Learning objectives
After completing this first session, you will be able to:
-
- Classify the factors contributing to AMR
- Identify interventions to contain AMR
Factors contributing to AMR
AMR is a natural phenomenon in which microbes acquire genes that enable resistance to antimicrobial drugs. Microbes with these genes will survive in the presence of a medicine, while susceptible ones (without the genes) will die. This will leave the resistant microbe behind with no competition for growth, allowing it to multiply and spread.
People can become infected by microbes that are already drug-resistant or microbes can become resistant after they start antimicrobial treatment. Resistant infections arising in this latter way result from a treatment that killed o” the susceptible microbes but left resistant ones behind to flourish. (Refer to the “What is AMR” session of the AMR Course (Part 1) for more information on the mechanism of resistance.)
Minimizing the impact of AMR requires an understanding of the factors that facilitate its development and spread.
Various researchers and organizations, including the World Health Organization (WHO) cite multiple interrelated factors that facilitate the development and spread of AMR:
-
- Antimicrobial misuse
- Limited access to quality and affordable antimicrobials, vaccines, and diagnostics Poor quality antimicrobial products
- Poor infection prevention and control and lack of clean water, sanitation, and hygiene (WASH) for humans and animals
- Poor regulation and enforcement of laws
- Inadequate surveillance of antimicrobial use and resistance
Several of these factors affect not only the human sector but also the animal and environmental sectors. As such, a problem in one sector can contribute to the spread of AMR in others due to the interface between the three. AMR is thus a One Health issue that cuts across the human, animal, and environmental ecosystem.
The factors listed above are especially common in resource-constrained countries due to:
-
- Weak governance and health systems
- Poor pharmaceutical management and regulation
- Inadequate infection prevention and control practices
The spread of resistant infections is also likely to be elevated in such settings as a result of urban overcrowding, unreliable availability of clean water, poor hygiene, civil conflicts, and high numbers of immunocompromised people living with malnutrition or HIV/AIDS.
Sources: World Economic Forum 2013; Pokharel et al 2019; WHO 2023a; Iskandar K et al 2020; Laxminarayanan R et al 2006
Glossary Term:
Immunocompromised
Highlight
In her foreword to the 2015 Global Action Plan on Antimicrobial Resistance, the then–director-general of the WHO Dr. Margaret Chan highlighted the threat that AMR poses to the global health community:
“Antimicrobial resistance threatens the very core of modern medicine and the sustainability of an effective, global public health response to the enduring threat from infectious diseases. Effective antimicrobial drugs are prerequisites for both preventive and curative measures, protecting patients from potentially fatal diseases and ensuring that complex procedures, such as surgery and chemotherapy, can be provided at low risk. Yet systematic misuse and overuse of these drugs in human medicine and food production have put every nation at risk. Few replacement products are in the pipeline. Without harmonized and immediate action on a global scale, the world is heading towards a post-antibiotic era in which common infections could once again kill.”
Source: WHO 2015.
Interventions to contain AMR
Interventions to contain AMR target several factors, including:
-
- Antimicrobial regulation
- AMR surveillance and research
- Sanitation, hygiene, and infection control
Interventions also encourage the development of new antimicrobials, cultivate stakeholders’ commitment, and promote stewardship for AMR containment, which depend on strong health systems. Containing AMR is crucial to preserve the effectiveness of affordable essential antimicrobials and ensure the success of universal health coverage.
Because AMR is a multi-faceted phenomenon, interventions designed to contain it must also be multi-faceted and interlinked. An ecological approach encompassing human, animal, and environmental sectors with the spirit of One Health, is necessary to tackle AMR successfully. Specific interventions, such as educational, managerial, and regulatory approaches are highlighted in the session on Prescribing and Dispensing Antimicrobials and throughout the course.
The WHO Global Action Plan on AMR (2015) provides a comprehensive framework of interventions to slow the development and contain the spread of drug resistance. The plan recommends that countries, international partners, and the tripartite of Food and Agriculture Organization of the United Nations (FAO), WHO, and World Organisation for Animal Health (WOAH) take actions to achieve the following objectives:
-
- Improve awareness and understanding of AMR through effective communication, education, and training
- Strengthen the knowledge and evidence base through surveillance systems and research
- Reduce the incidence of infection through effective sanitation, hygiene, and infection prevention measures
- Optimize the use of antimicrobial medicines in human and animal health
- Develop the economic case for sustainable investment that accounts for the needs of all countries and increases investment in new medicines, diagnostic tools, vaccines, and other interventions
In a 2011 issue of the Bulletin of the World Health Organization, Leung and colleagues frame the AMR challenge this way:
“The drivers of antimicrobial resistance are interlinked, and so are the solutions. Single, isolated interventions have little impact. Strong leadership and political will are required to bring about bold changes in policies, organize health systems and legislative structures as required, and translate knowledge and recommendations into practice.”
Source: Leung et al. 2011; WHO 2011a; WHO 2015a; Pokharel et al 2019
Highlight
The 2015 WHO Global Action Plan on AMR emphasizes the need for the whole-of-society engagement including a One Health approach:
“Antimicrobial resistance will affect everybody, regardless of where they live, their health, economic circumstances, lifestyle or behaviour. It will affect sectors beyond human health, such as animal health, agriculture, food security and economic development. Therefore, everybody—in all sectors and disciplines—should be engaged in the implementation of the action plan, and in particular in efforts to preserve the effectiveness of antimicrobial medicines through conservation and stewardship programmes.”
Source: WHO 2015
New page
Prescribing and dispensing antimicrobials
In the previous session, we reviewed the causes and ways to contain AMR. In the list of causes, the first was antimicrobial misuse. Health care providers, patients, and consumers are major drivers of AMR.
The inappropriate use of antimicrobials in food-producing animals is another critical contributor. It is estimated that about 70%, and in some countries up to 80%, of medically important antimicrobials are used in animals, largely for growth promotion.
-
Learning objectives
After this session, you will be able to identify the role that health care providers, particularly prescribers and dispensers, play in facilitating the development of AMR, as well as intervention areas.
We examine the factors that contribute to inappropriate prescribing and dispensing of antimicrobials:
-
- Insufficient knowledge and training
- Perceptions and attitudes of prescribers and dispensers
- Perverse economic incentives
- System-related factors
-
We also discuss several intervention areas that address these factors:
-
- Educational interventions to improve knowledge and change attitudes and behavior
- Managerial interventions to improve the system and environment
- Regulatory interventions to protect against negative economic and system-related factors
Now, let’s start this session by looking at inappropriate prescribing and dispensing.
Sources: WHO 2017; Tiseo K et al 2020; Sweileh W 2021, Machowska A & Lundborg C 2019
Glossary Term:
Dispensers
Did you know?
This course focuses on antimicrobial use in humans; however, for more information on AMR in the animal and environmental sectors, review the following FAO and UNEP webpages:
Sources: WHO 2017; Tiseo K et al 2020; Sweileh W 2021, Machowska A & Lundborg C 2019
Inappropriate prescribing and dispensing
While AMR is a naturally occurring phenomenon, we learned in the AMR 1 course that antimicrobial use triggers the development of resistance through selective pressure, a key factor in natural selection, which drives evolution. Irrational prescribing and dispensing are common causes of overuse and misuse of antimicrobials, which can accelerate and amplify AMR.
- Examples of irrational prescribing
- Using antimicrobials when not needed
- Prescribing wrong antimicrobials
- Using broad-spectrum or multiple antimicrobials where narrow-spectrum or single agents would work well
- Prescribing incorrect dose or duration of antimicrobials
- Examples of irrational dispensing
- Dispensing incomplete courses of antimicrobials
- Poor or no counseling while dispensing antimicrobials
- Selling antimicrobials without prescription
Globally, more than half of all medicines are prescribed, dispensed, or sold inappropriately. It is estimated that up to 50% of all antibiotic prescriptions are unnecessary or not optimally e”ective as prescribed. The challenges are higher in low- and middle-income countries (LMICs) due to weaknesses in health systems, including those related to antimicrobial stewardship and prescribing practices. A study by Fink and colleagues on antibiotic exposure in children under five showed that between 2006 and 2016, children in eight LMICs received, on average, 25 antibiotic prescriptions from birth through five years, which is up to five times higher than the already-high levels observed in high-income settings. Several reports from LMICs on antibiotic use in primary care settings have shown high rates of inappropriate use (61% from China, 88% from Pakistan, and 55% from South Africa).
WHO estimates that as much as two-thirds of all antibiotics globally are sold without a prescription, largely through poorly regulated private-sector outlets.
Fink et al., 2020 also showed that 69% of antibiotics in the sub-Saharan Africa region were sold without prescription by retail drug outlets. This is a problem in many LMICs where people access medicines through informal providers, such as street peddlers or drug shops, where risk of poor drug quality and misuse of antimicrobials are more common. Retail drug vendors pose a particular problem: few are trained, and many do not follow regulations. These shops sell antimicrobials without a prescription, often in small quantities rather than in complete regimens, and sell drugs to customers regardless of whether they are actually sick. Even if the vendor knows the correct antimicrobial prescribing practice, they usually yield to customer pressure.
Sources: WHO 2011d; CDC 2013a; Holloway and van Dijk 2011; WHO 2010; Nugent, Back, and Beith 2010; Okeke et al. 1999; Belachew et al. 2021; Embrey et al., 2016; Fink et al., 2020; CDDEP 2021; Sartelli M et al 2020
Glossary Term:
Irrational prescribing selective pressure
Did you know?
Only about half of all malaria cases receive the recommended first-line antimalarial agents. Similarly, only 50% to 70% of pneumonia cases are treated with appropriate antibiotics.
Source: Holloway and van Dijk 2011
Did you know?
About half of all cases of acute viral upper respiratory tract infection and viral diarrhea are inappropriately treated with antibiotics in LMICs. Additionally, in these settings, up to 50% of all events when a medicine is dispensed are inadequate; for example, patients do not receive directions on how to take their medicines.
Source: Holloway and van Dijk 2011
Insufficient knowledge and training
Without accurate and up-to-date knowledge, health care providers are more likely to prescribe or dispense medicines inappropriately.
The infographic illustrates the following barriers, which contribute to a lack of knowledge:
-
- Inadequate training in rational antimicrobial use and related issues
- Limited access to up-to-date product information
- Lack of standard treatment guidelines
- Poor prescribing role models and supervision
- No national medical information center
- Inability to properly evaluate information sources (e.g., from the internet)
The list above isn’t wrong but it’s worth expanding.
-
- Training: It’s not enough to say, “training.” AMR and rational medicine use are often inadequately covered in pre-service and in-service training for health care providers.
- Medical information centers: Training isn’t the end-all solution. Health care providers in resource-limited settings are frequently constrained by their lack of access to independent, unbiased medicines and therapeutics information in the workplace, including up-to-date standard treatment guidelines, essential medicines lists, and formularies. In fact, in some settings, health care providers only have promotional information from pharmaceutical companies as references.
Such deficiencies in training and access to information affect health care providers’ competencies and ability to prescribe and dispense antimicrobials appropriately. The next step, after acquiring training and information, is to implement it correctly. Let’s review that next.
Sources: SIAPS 2013; WHO 2012b; Norris et al. 2005; MSH 2012
Glossary Term:
Formularies
In-service training
Medicines and therapeutics information Standard treatment guidelines Essential medicines lists
Perceptions and attitudes of prescribers and dispensers
Determinants other than knowledge can influence practice behavior. In other words, while health care providers may have the right knowledge, it may not translate to the right behavior or practice.
As shown in the infographic, perceptions and attitudes can dictate prescribing and dispensing behaviors. Let’s take a look at the perceptions and attitudes, expanding on each to ensure comprehension.
-
Fear of poor clinical outcomes
Prescribers in LMICs often fear that patients will not improve without antimicrobial treatment. If unsure of a diagnosis, they will often prescribe antibiotics to be "on the safe side" and to prevent a secondary infection (bacterial) in the case of a viral infection.
-
Fear of litigation
In some countries, a prescriber may fear a patient’s legal action if antimicrobials are not prescribed and there is a bad clinical outcome.
-
Perception of or actual patient demands
Many prescribers feel that patients will be dissatisfied with their care if a medicine is not prescribed, so they choose to prescribe medicines to avoid the risk of losing business. Patients often place more value on the medicine than on the medical consultation. For the same reason, dispensers will sell whatever the customer wants, even if it is unnecessary or a smaller dose than treatment guidelines recommend.
-
Peer pressure and social norms
Standards and norms held by senior health care providers and peers influence prescribing and dispensing practices. Physicians who offer the latest antibiotics may appear more informed, and they may prefer new antibiotics even when older antibiotics may still work quite well.
Perceptions and attitudes are not the only factors influencing behavior. Let’s take a look at the power of the economy next.
Sources: Carlet et al 2012; Haak and Radyowijati 2010; Radyowijati and Haak 2003; Kotwani A et al 2017
Glossary Term:
Secondary infection
Perverse economic factors influencing prescribing and dispensing
Perverse economic incentives can influence health care providers’ behaviors. That is to say, profit motive may overrule other determinants when making decisions related to prescribing and dispensing.
Studies from several countries have illustrated the following economic-based practices, which are often common:
- Dispensing medicine because a profit is received
- Splitting the profit with the drug supplier
- Adjusting the type and quantity of medicine dispensed based on the client’s ability to pay
- Prescribing more expensive antimicrobials to insured patients resulting in higher profits Prescribing more medicines and/or injections per patient encounter
Bottom line, economic interests can trigger the owners and employees of retail drug outlets to dispense antibiotics without prescriptions (see the Highlight box below). The last influence we will cover has to do with the health system itself.
Sources: Li et al. 2012; Haak and Radyowijati 2010; Trap et al. 2002; Dong et al. 1999a, 1999b; Davari M et al 2018; Reynolds L & McKee M 2009; Porter G 2021; Kaiser B & Schmid C 2013: Bahta M et al 2021; Dhingra et al 2020; Goldacre et al 2019
Highlight
In a qualitative study based on focus group discussion and key informant interviews at retail drug outlets in Eritrea, all the key informants highlighted economic interest as a factor in selling antibiotics in retail drug outlets.
Source: Bahta et al 2021
Health system–related factors influencing prescribing practices
So far, we have considered the following influences regarding inappropriate prescribing and dispensing.
-
- Insufficient training and knowledge
- Perceptions and attitudes
- Perverse economic factors
The last behavioral influence is the health system. Health system factors, such as capacity, policies, and practice setting, can greatly a”ect prescribing, dispensing, and counseling practices.
These factors, illustrated in the infographic, include the following:
-
- Availability and quality of antimicrobials
- Laboratory services and surveillance capacity
- Pharmaceutical promotion
- Health insurance, or lack thereof
- Workload
For example, if prescribers lack access to resources and receive little supervision, and if no policy exists on pharmaceutical promotion, face-to- face visits from industry representatives can negatively influence prescribing practices. Supportive, rather than punitive monitoring, and supervision combined with prescription audits can be a particularly effective way to improve prescribing.
Being aware of the issues that can allow incorrect prescribing and dispensing is just part of the process needed to stop AMR. A later session on Health Systems and Regulatory Issues discusses the impact of health system weaknesses on antimicrobial resistance in detail.
Source: MSH 2012
Let’s look at interventions next.
Prescribing and dispensing antimicrobials: Interventions
We have discussed the four factors relating to prescribing and dispensing antimicrobials that contribute to the emergence and spread of antimicrobial resistance. Now we will address the three types of interventions:
-
- Managerial
- Educational
- Regulatory
Let’s start with managerial interventions.
Managerial interventions
Managerial interventions involve putting tools and systems in place to structure or guide prescribing or dispensing decisions. Hospitals, clinics, and pharmacies can promote management practices that standardize antimicrobial use and encourage good pharmaceutical management.
Managerial techniques to ensure appropriate prescribing, dispensing, or administration of medicines include the following:
-
- Supervising and supporting the clinical practices of physicians, pharmacists, and nurses.
- Developing and implementing standard treatment guidelines (STGs) and formularies and monitoring adherence to these guidance tools.
- Conducting medicine use evaluations and prescribing audits and feedback.
- Developing and implementing locally appropriate antibiotic policies, such as requiring a physician to obtain pre-approval to use certain reserve antibiotics.
- Limiting routine procurement to a restricted list of medicines.
When implemented and monitored effectively, these managerial interventions improve medicine use.
Glossary Term:
Audit and feedback
Let’s look at an example tool for managing.
Access, watch, reserve classification: A valuable tool for antimicrobial stewardship
WHO’s Access, Watch and Reserve (AWaRe) classification is a simple and innovative managerial tool for countries to categorize the antibiotics in their essential medicines lists (EMLs), STGs, and formularies to help improve antibiotic use and contain AMR. AWaRe classification is used to guide appropriate treatment prescribing and also to characterize and monitor antibiotic use at facility as well as national level.
WHO defines the three categories as follows:
-
ACCESS
These are antibiotics of choice to treat the 25 most common infections. Antibiotics in this category generally have low toxicity and low propensity to provoke resistance. They should be available at all times, affordable, and quality- assured. The goal is for 60% of global antibiotic consumption to come from this group.
-
WATCH
This group includes the most critically important antimicrobials for human medicine and veterinary use. These antibiotics are recommended only for specific, limited indications.
-
RESERVE
These antibiotics should only be used as a last resort when all other antibiotics have failed or cannot be used due to contraindications. Newer generation antibiotics fall in this category.
AWaRe categorization provides a framework for monitoring to ensure that essential antibiotics are available when needed (access) and that the right antibiotics are prescribed for the right infections (appropriate use). Besides helping to contain AMR by improving antimicrobial stewardship, AWaRe categorization also improves the cost-e”ective use of antibiotics.
Countries are incorporating AWaRe as they revise their national EMLs, STGs, and formularies. In the 2021 survey on implementation of the WHO Global Action Plan for AMR, 36% of countries had adopted AWaRe, which was up from 26% in 2020.
To track national adherence to AWaRe categorization, countries need to have a national antibiotic consumption and use tracking system in place that includes not only human but also veterinary and agricultural consumption. Individual facilities can track their AWaRe progress through prescription audits and drug utilization reviews.
More information is available at https://www.who.int/publications/i/item/WHO-MHP-HPS-EML- 2023.04
Sources: WHO 2021d; WHO 2019a
Glossary Term:
AWaRe classification
Highlight
The WHO benchmarks on International Health Regulations (IHR) capacities (2019) recommends integrating AWaRe categories of antibiotics into EMLs and STGs. USAID Medicines, Technologies and Pharmaceutical Services collaborated with Bangladesh, Burkina Faso, Democratic Republic of the Congo, Ethiopia, Kenya, Mali, and Tanzania to achieve this objective.
Source: Joshi et al, 2023
A Technical Guide to Implementing the World Health Organization’s AWaRe Antibiotic Classification in MTaPS Program Countries is a practical resource for LMICs to use for incorporating AWaRe into EMLs and STGs.
Successful case studies
In Thailand, implementing STGs led to a significant reduction in antibiotic use for respiratory infections. Similarly, medicine use evaluations or audits and feedback have e”ectively changed the prescribing behavior of health care providers.
A review of 13 studies found that a trained person’s face-to-face visit to a health care provider in their setting improved prescribing practices in every case. An important vehicle that can be used to implement these interventions is a drug and therapeutics committee (DTC), which is explained further in the Hospitals session.
In its goal to improve the functionality of DTCs in Tanzania, the Mission for Essential Medical Supplies (MEMS) organization analyzed data at two hospitals to assess prescribing compliance to the Tanzania STGs. The analysis found that only 45.5% of the treatments complied with the STGs, with common deviations including incorrect type of antibiotic and dose as well as over-prescription of antibiotics. Following the baseline assessment, MEMS developed a multi-pronged intervention to improve STG adherence. Sta” presented the data on the poor prescribing practices at clinical and DTC meetings, provided reference books, and trained DTC members and hospital sta”. After six months, prescribing compliance with the STGs increased to 94%.
Sources: WHO 2012b; Thamlikitkul and Apisitwittaya 2004; MSH 2012; SIAPS 2015
Glossary Term:
Medicine use evaluation
Highlight
Tanzania launched the 6th edition 2021 Standard Treatment Guidelines / National Essential Medicines List (STGs/NEMLIT) with guest of honor, the minister of health.
Educational interventions
It shouldn’t be a surprise to see education as an intervention as the lack of training was a factor in the inappropriate prescribing and dispensing.
Education is important to improve the knowledge, perceptions, and attitudes of health care providers. Although educational interventions are not powerful enough to change behavior when used alone, they are necessary to understanding and supporting antimicrobial resistance containment programs.
Educational interventions are most e!ective in shaping behavior when introduced early in the provider’s professional career. Rational medicine use and AMR topics need to be incorporated into not only in-service (continuing education) programs, but also in pre-service training courses. Revising Pre-service Curriculum to Incorporate Rational Medicine Use Topics: A Guide provides guidance on reforming pre- service curriculums to incorporate AMR and rational medicine use topics.
Continuing education/continuing professional development programs are important ways to keep health care professionals updated on the latest research and practices, and to support providers to incorporate best practices and new information into their daily work. Continuing Pharmaceutical Education: Guide to Establishing Quality Assured and Accredited Programs outlines how to establish effective programs.
For best results, educational interventions should involve multiple complementary activities, including behavior change communication, regulatory enforcement, peer interaction, supervision, and incentives.
In a rural Kenya town, for example, skill-based workshop training, accompanied by job aids, ongoing monitoring, and community behavior change efforts improved appropriate treatment dosing six-fold.
Sources: Laxminarayan et al. 2013; Nugent, Back, and Beith 2010; Joshi 2010; Joshi et al. 2014; PAHO 2021
Glossary Term:
Job aid
Behavior change communication In-service training
Case studies of successful curriculum reform efforts
With technical collaboration from the USAID-supported Systems for Improved Access to Pharmaceuticals and Services program, the University of Namibia School of Pharmacy strengthened pre-service pharmacy training on rational medicine use and AMR for undergraduate pharmacy students. The instructional delivery method primarily involved case-based and self-directed learning approaches.
Similarly, the USAID Medicines, Technologies, and Pharmaceutical Services (MTaPS) program collaborated with the University of Nairobi School of Pharmacy to develop a pre-service antimicrobial stewardship (AMS) curriculum. A university committee worked with MTaPS to develop a process roadmap and conduct needs assessments that guided the curriculum revision, including the addition of practical aspects of AMS. The curriculum will be used to develop the capacity of both under- and postgraduate health sciences students (e.g., medical, pharmacy, and nursing students) on AMS as a key strategy to contain and prevent AMR. The MTaPS program in Kenya went on to train almost 90 Bachelor of Pharmacy students in the first quarter after the launch.
In addition to pre-service curriculum revision, Kenya is also supporting in- service AMS training for health professionals. Led by the Pharmaceutical Society of Kenya and regulatory authorities, MTaPS and several other health professional associations representing physicians, nurses, and lab professionals developed a nine-module continuing professional development (CPD) course on AMS. Between September and December 2020, MTaPS collaborated with the associations to conduct virtual AMS CPD sessions to sensitize over 1,000 health care workers on the practical aspects of AMS in health care settings.
Health care workers participating in these sessions earned CPD points from their respective regulatory bodies that also aligned with the renewal of annual practice licenses, which was an incentive for attending the training. The regulatory bodies involved included the Pharmacy and Poisons Board, the Nursing Council of Kenya, and the Kenya Medical Practitioners and Dentists Council.
Sources: Joshi et al., 2014, Jaguga and Kusu 2021
Regulatory interventions
So far, we have presented interventions associated with management and education. Last up are regulatory interventions.
A strong regulatory structure is crucial for supporting rational prescribing and dispensing.
Proper regulations improve prescribing and dispensing in several ways:
-
- Limiting over-the-counter availability of antimicrobials
- Regulating drug seller practices
- Removing unhealthy financial incentives for prescribers and dispensers
- Restricting who is allowed to prescribe or dispense
- Banning use of antimicrobials for growth promotion in animals raised for food Regulating and monitoring promotional activities by pharmaceutical companies
Regulations must also be coupled with strong and effective enforcement, or they will be useless. The session on Health Systems and Regulatory Issues discusses regulations in detail.
Source: MSH 2012
Glossary Term:
Over-the-counter medicines
New page
Patients and the general community
Now that we know about the role that prescribing and dispensing plays in contributing to the development of AMR, let’s now focus on antimicrobial usage by patients and the general community.
Did you know that about 80% of antibiotic use occurs in the community, outside of health facilities. Unlike medicines administered in a hospital, medicines consumed in the community are generally not taken under the supervision of health professionals.
Factors related to patients and the community play a considerable role in driving irrational antimicrobial use and drug resistance. These factors include the following:
-
- Misconceptions and beliefs about antimicrobial use.
- Inappropriate health-seeking and treatment behavior, such as irresponsible self-medication and nonadherence to treatment (e.g., not taking the full dose, quitting treatment when symptoms ease or because of unpleasant side effects).
Information-, education-, and communication-related interventions are used to raise awareness. When such interventions apply social and behavior change approaches, they can help improve behavior related to antimicrobial use among patients and the community.
By the end of this session, you will be able to identify the role that patients and the general community play in contributing to the development of AMR, as well as key interventions to address them.
Sources: Christiansen et al. 2002; WHO 2001; Byrne 2019; PAHO 2021; Kotwani et al 2021; Chan et al 2021
Glossary Term:
Self-medication
Antimicrobial use: Misconceptions and beliefs
Misconceptions and beliefs
Patients’ beliefs and misconceptions about medicines influence how they interpret instructions from prescribers and dispensers and how they use medicines.
Patients’ misconceptions about medicines include the following:
-
- Antimicrobials are strong or extraordinary medicines capable of preventing or curing almost any illness
- New and expensive medicines are more efficacious than older medicines
These beliefs and misconceptions influence patients’ desire for antimicrobial prescriptions and encourage them to use antimicrobials without prescriptions.
Direct-to-consumer pharmaceutical advertising and promotion can also influence and stimulate patient demand for antimicrobials.
Sources: Widayati et al. 2012; WHO 2001
Nonadherence to treatment
Patients’ attitudes influence the way they use medicines. Two primary patient-related behaviors contribute to antimicrobial resistance:
-
- Nonadherence to recommended antimicrobial treatment
- Uninformed or irresponsible self-medication
WHO defines adherence as “the extent to which a person’s behavior—taking medication, following a diet, and/or executing lifestyle changes—corresponds with agreed recommendations from a health care provider.” Proper medication adherence improves patient outcomes and quality of life and is cost-efficient for the health system, because poor adherence can cause treatment failure. It also helps preserve the effectiveness of antimicrobials and contain AMR.
However, nonadherence to medication is a global problem and common in all settings; about half of all patients globally do not adhere to recommended treatments. Nonadherence is especially common among patients with chronic conditions such as diabetes, hypertension, heart disease, and HIV/AIDS. Estimates suggest that nonadherence contributes to up to 57% of the world’s avoidable health care costs due to suboptimal use of medicines. If everyone adhered to treatment, 4.6% of the global health expenditure—269 billion US dollars—could be saved.
Nonadherence occurs when a patient:
-
- Does not purchase or obtain a full course of antimicrobial treatment, often because of cost
- Stops treatment earlier than directed, after relief from symptoms or because of side effects
- Forgets and misses doses
- Does not take the recommended amount or takes doses at the wrong time
Besides patient-related factors, other factors that can affect patient adherence include:
-
- The way a specific condition/infection is treated (e.g., high pill burden)
- The quality of counseling or information that the patient receives
- Structures of the health system itself, for example, limited health care coordination, poor patient tracking and record systems, and disease stigma
Uninformed and irresponsible self-medication, another patient behavior that contributes to antimicrobial resistance, is described on the next page.
Sources: WHO 2003; WHO 2012b; IMS Institute for Healthcare Informatics 2012; Holloway and van Dijk 2011; MSH 2012; Joshi et al 2016
Self-medication
So far, we have presented two factors associated with patient and community behavior that can lead to AMR. This next factor, self-medication, shouldn’t come as a surprise as it was discussed briefly on the previous page. Let’s learn more about this factor.
Self-medication includes the following:
-
- Using leftover antimicrobials from a previous treatment course
- Purchasing medicines over-the-counter that require a prescription
- Sharing unused antimicrobials with others
Factors that may influence a person’s decision to self-medicate include:
-
- Poverty
- Poor access to formal health care Lack of information
- Advertisements
- Internet sales
- High disease burden
Therefore, self-medication is especially common in low- and middle-income countries where the population can access antibiotics over-the- counter in pharmacies or local marketplaces. It may include taking unnecessary or ineffective antimicrobials or taking inadequate doses.
A population-based study in Laos on the use of antibiotics among 300 mothers following delivery found that 59% used antibiotics based on their own decision to do so or on the advice from relatives or friends. Few women knew the reasons to use antibiotics and even fewer knew about antibiotic resistance.
Sources: Carlet et al. 2012; WHO 2012b; Widayati et al. 2012; Keohavong et al. 2011; WHO 2001; Kotwani et al 2021; PAHO 2021
Interventions
We have addressed how certain patient and community misconceptions and beliefs can lead to behaviors that contribute to the development of antimicrobial resistance. These inappropriate behaviors include nonadherence to treatment and irresponsible self-medication.
Now, let us explore the primary types of interventions that can be used to address these misconceptions and discourage risky behaviors. At the heart of this process is education.
Education can be accomplished multiple ways. Let’s consider the following:
-
- Professional health care workers educate the public as part of their practice
- Mass media used to send appropriate messages to the masses
Highlight
After finding a lack of knowledge on AMR among Addis Ababa Women Federation members during a 2020 knowledge and behavior assessment, the USAID Medicines, Technologies, and Pharmaceutical Services (MTaPS) program engaged with the Ethiopian Youth and Women Federations, a civil society organization (CSO) involved in health education, to add AMR to their health messaging.
MTaPS conducted a 2-day training on AMR for 29 volunteers from that CSO, who then cascaded the training to 520 members of the Addis Ababa Women Federation with minimal support from MTaPS. The success of this endeavor highlights the potential that communities, such as CSOs, can play in disseminating important messaging on AMR.
After the training, the Vice President of the Addis Ababa Women Federation, Huluagerish Tazeze, said, “This training opportunity helped me to recognize that AMR is an important topic that we had not addressed so far in our engagement with the public. From now on, we will have sessions on AMR when we discuss public health issues with our communities.”
Source: MTaPS 2021c
Patient education
Educational interventions are designed to raise awareness about rational medicine use among patients and the community.
The WHO Global Strategy for Containment of AMR recommends the following interventions:
-
- Educate patients and the general community on the appropriate use of antimicrobials
- Educate patients on the importance of preventing infection, such as immunization, vector control, and use of bed nets
- Educate patients on simple measures that may reduce infection transmission in the household and community, such as hand washing, food hygiene, etc.
- Encourage appropriate and informed health care- seeking behavior
- Educate patients on suitable alternatives to antimicrobials for relief of symptoms
- Discourage patient self-initiation of treatment, except in specific circumstances
To be effective, public and community education and awareness-raising should use evidence-based and behavior change-oriented approaches that target underlying public perceptions and beliefs.
The COVID-19 pandemic has shown the importance of engaging and properly educating individuals, patients, and communities in preventing and managing infections such as hand hygiene, social distancing, mask use, and cough/sneezing etiquette.
Source: WHO 2001; PAHO 2021; Chan et al 2021
Glossary Term:
Vector control
Example: World AMR Awareness Week—educating about AMR
Launched in 2015 after endorsement at the Sixty-Eighth World Health Assembly, World AMR Awareness Week (WAAW) is a global campaign to raise awareness of AMR and best practices among the public, health workers, and policy makers. Celebrated annually between November 18 and 24, WAAW’s four objectives are to 1) make AMR a globally recognized issue by engaging human, animal, plant, and environment sectors in a One Health approach; 2) raise awareness of the need to protect antimicrobial efficacy through prudent and responsible use; 3) increase recognition of the roles that individuals, governments, civil society organizations, and relevant multisectoral organizations must play in tackling AMR; and 4) encourage behavior change to improve antimicrobial use across all sectors and spread the message that simple actions can make a big difference.
Source: WHO 2023a; Wu et al. 2021
Mass media
Although challenging, changing patients’ perceptions and behavior related to medicine use is critical to containing antimicrobial resistance.
Mass media can be an effective way to raise awareness and influence behavior change.
A comprehensive review of public education campaigns on rational antimicrobial use targeting patients and doctors in 22 high-income countries showed that most of the programs positively affected antibiotics use. Multi-faceted campaigns carried out over several years seemed to have the greatest impact.
France launched a national campaign called Les antibiotiques, c’est pas automatique (Antibiotics are not automatic) from 2002 to 2007 to reduce unnecessary antibiotic use. It comprised an educational campaign for health care workers, the promotion of rapid tests to diagnose streptococcal infections, and a public information campaign about viral respiratory infections and AMR. The campaign succeeded in reducing antibiotic prescribin by 26.5%. The greatest decline (35.8%) was among children aged 6 to 15 years.
Journalists can be a powerful ally in educating the public on rational medicine use and antimicrobial resistance. In Ethiopia, the USAID-funded Systems for Improved Access to Pharmaceuticals and Services program helped the Food, Medicines, and Health Care Administration and Control Authority to educate journalists on rational medicine use and AMR containment. As a result of this capacity- building effort, mass media channels such as radio, TV, and print media published and broadcast 218 stories on AMR containment and rational medicine use between 2012 to 2014 to inform, educate, and empower the public.
Professional societies have also taken the initiative to educate the public on antibiotic use and antimicrobial resistance. National Pharmacy Week campaigns were organized in Namibia in 2013 and in South Africa in 2014, for which rational antibiotic use and AMR were key themes.
Sources: SIAPS 2014; Huttner et al. 2010; SIAPS 2015
Highlight
With 4.5 billion users worldwide in 2021, social media has become a heavily used source of information and means of communication. During the COVID-19 pandemic, social media was widely used to raise awareness and disseminate information.
Source: Parveen et al 2022
Highlight
The USAID Medicines, Technologies and Pharmaceutical Services (MTaPS) program collaborated with national counterparts to assess the baseline knowledge of AMR among 114 journalists from all seven provinces of Nepal, including the impacts of gender on AMR. This helped identify gaps and informed the development of workshops to sensitize nationwide media on AMR.
Source: MTaPS 2024
Success story: AMR advocacy, awareness, and containment activities
Ecumenical Pharmaceutical Network (EPN), a faith-based regional network based in Africa with 141 members in 38 countries, collaborated with the USAID-funded Strengthening Pharmaceutical Systems and Systems for Improved Access to Pharmaceuticals and Services Program to initiate antimicrobial resistance-awareness activities among its member organizations in multiple countries.
Between November 2008 and June 2011, EPN members carried out well over 100 activities related to AMR awareness, sensitization, advocacy, research, training, and publication of AMR information, including the following:
-
- India: Educated 1,371 adolescents (14–18 years) in 11 schools on the dangers of AMR, the need to use medicines correctly, and on health promotion. Pre- and post- intervention assessments indicated that their knowledge level increased from 29% to 66%.
- Tanzania: Carried out an intervention to increase prescribing adherence to treatment guidelines; post-intervention assessments showed improvements. For example, prescribing compliance improved from 55% at baseline to 96% post-intervention at Marangu Hospital.
- Zimbabwe: Trained journalists on AMR and rational medicine use resulting in media publications and broadcasts.
EPN and its members developed an AMR Call-to-Action advocacy document in five languages and distributed it to a wide circle of stakeholders to promote awareness and encourage involvement in the local and global fights against AMR. EPN also created an AMR campaign website with multiple resources and tools for its members, including bookmarks, fact sheets, posters, and comic strips.
The comic strips (shown above), produced in English, French, and various local languages, respond to a real need for easy-to-understand information and have been successful in transmitting relevant messages. EPN has distributed more than 33,000 copies in 35 countries, resulting in positive behavior change and a social commitment by communities to tackle AMR.
After their kick-off regional meeting on AMR in 2008, EPN was able to leverage support from multiple partners for their ongoing AMR work (Action on Antibiotic Resistance, Bread for the World, Difaem, Misereor, Strengthening Pharmaceutical Systems, and Systems for Improved Access to Pharmaceuticals and Services). To further support sustainability, EPN made AMR an organizational priority in their 2016-2020 strategic plan.
For step-by-step guidance, examples, and practical tools on building coalitions for AMR advocacy and containment, read Building Local Coalitions for Containing Drug Resistance: A Guide.
Sources: EPN 2012; SIAPS 2017; Joshi and Kusemererwa 2011; Joshi et. al 2015; Joshi et al., 2018; SIAPS 2015a
New page
Health systems and regulatory issues
In a previous session, we presented how health systems can contribute to AMR and how regulatory interventions can support appropriate use of antimicrobials. In this session, we expand on these topics.
Strong health systems, including appropriate policies and regulations, contribute to an enabling environment to preserve the effectiveness of antimicrobials and contain antimicrobial resistance.
However, the existence of policies and regulations alone is not enough. They must be backed by effective enforcement.
-
Learning objectives
By the end of this session, you will be able to identify weaknesses in health systems and regulatory structures that contribute to AMR. These include the following:
-
- Weak or nonfunctional multisectoral coordination on AMR
- Weak policy and regulation related to medicine supply and access
- Inability to minimize falsified and substandard medicines
- Unrestricted pharmaceutical promotion
- Lack of antimicrobial use and resistance surveillance
You will also learn how health systems—and specifically the regulatory system—can combat AMR through the following:
-
- Policy and regulatory interventions to improve medicine supply and access
- Regulatory interventions to assure medicine quality
- Regulatory interventions targeting pharmaceutical promotion
- Interventions targeting surveillance of antimicrobial use and resistance, including antimicrobial leadership and stewardship initiatives
Let’s start by looking at common weaknesses in health systems and regulatory structures that allow AMR to happen.
Glossary Term:
Pharmaceutical promotion
Weak or nonfunctional multisectoral coordination on AMR
AMR cannot be conquered without addressing all its drivers, which include:
- Humans
- Animals
- Plants
- Environment
Consequently, the One Health approach, and multisectoral coordination (MSC) at its core, is an essential component of the global AMR response. Most countries’ national action plans on AMR emphasize the fundamental importance of MSC. A UN General Assembly High-Level Meeting on AMR, held on September 26, 2024, also reiterated the pivotal importance of MSC for containing AMR.
However, having MSC structures in place is not enough to guarantee their robust functioning. A WHO report (EB148/11, 16 December 2020) acknowledged progress in forming MSC structures on AMR in many countries, but also highlighted that many of these bodies are not functional.
To be effective, MSC-AMR bodies need to be supported through an enabling environment that includes:
-
- Mandates
- Budget
- Human resources and their capacity-strengthening
Additionally, expanding MSC structures and functions at subnational and local levels are crucial for nationwide operationalization of the national actions plans on AMR, stronger localization, and increased e”ectiveness of health security efforts.
Sources: WHO 2024, WHO 2020a
Weak policy and regulation related to medicine supply and access
In addition to multisectoral coordination on AMR, it is important to look at policy and regulatory issues related to medicine supply and access. Government policy and regulation, or lack thereof, can have an impact on the control of medicine supply, distribution, and sales.
Without controls within the health system, antimicrobial medicines may be sold irresponsibly through retail outlets or street vendors.
Antibiotics are one of the most commonly purchased products in the world, and as mentioned in the session on Prescribing and Dispensing Antimicrobials, up to two-thirds of all antibiotics are sold without prescriptions, mostly through unregulated private sector outlets. Over-the-counter availability of prescription-only medicines can lead to overuse and misuse, thus propagating the emergence and spread of AMR.
Another equally formidable challenge in low- and middle- income countries is lack of access to antimicrobials when they are really needed. Irregular supply such as stock outs and expense (e.g., lack of insurance and high product prices) contribute to AMR—these constraints may result in the sale of an incomplete course of antimicrobials (to avoid paying out of pocket for a full course) or motivate patients to seek alternatives that could include unaccredited drug shops that sell substandard or falsified medicines.
Strong systems-based efforts, such as robust supply chain systems, are needed to expand appropriate and sustainable access to antimicrobials, while also restricting inappropriate access through regulatory oversight and enforcement.
Sources: Laxminarayan et al 2013; WHO 2011c; Holloway and van Dijk 2011; Laxminarayan et al 2015
Inability to minimize falsified and substandard medicines
As mentioned on the previous page, substandard or falsified medicines contribute to AMR. Such poor-quality medicines are a problem everywhere, but particularly in resource- limited countries.
A recent systematic review of 96 studies from low- and middle-income countries worldwide showed that the prevalence of substandard and falsified medicines was 13.6% overall, with 19.1% for antimalarials and 12.4% for antibiotics. However it is assumed that these figures are underestimations of the true nature of the problem.
Regional figures ranged from 18.7% in Africa to 13.7% in Asia and 14.4% for other single-region studies. Data on the estimated economic impact were limited primarily to market size and ranged widely from $10 billion to $200 billion. The prevalence was higher in countries with weak governance, regulatory capacity, and pharmacovigilance. A 2013 study of 39 African countries estimated that in children under five years of age, 122,350 deaths were associated with the use of poor-quality antimalarial medicines.
Substandard antimicrobials can come from multiple sources such as poor quality:
- Manufacturing
- Packaging
- Transportation
- Storage conditions
These products can be dispensed in:




Such products may result in:
- Treatment failure
- Extended hospital stays
- Need for more expensive and toxic treatment
- Growth of resistant strains of microbes
The increased morbidity and mortality associated with the use of substandard and falsified medical products combined with the economic consequences to the patient, family, and community result in a loss of confidence in health care providers and the overall health system.
Many low- and middle-income countries lack the resources and enforcement capacity to safeguard their populations from falsified and substandard medicines. What results is a largely unregulated pharmaceutical market where poor-quality medicines circulate freely.
Sources: Almuzaini, Choonara, and Sammons 2013; Nugent, Back, and Beith 2010; Renschler et al 2015; WHO 2018; Ozawa et al., 2018; Schäfermann et al 2020
Glossary Term:
Sub-therapeutic levels
Unrestricted pharmaceutical promotion
We just discussed several reasons that contribute to poor quality antimicrobials. However, poor-quality isn’t the only issue.
Pharmaceutical companies spend considerable sums of money to promote their products. The WHO defines pharmaceutical promotion as “all informational and persuasive activities by manufacturers and distributors, the e!ect of which is to induce the prescription, supply, purchase, and/or use of medicinal drugs.”
Examples of pharmaceutical promotion activities include the following:







Over 80% of pharmaceutical promotion efforts are directed towards physicians. Promotion influences physicians’ attitudes more than they realize. Similarly, patients exposed to direct-to-consumer advertising make more requests for advertised medicines.
Unrestricted promotional activities can contribute to both irrational prescribing and patient demand.
Now that we have reviewed the weaknesses in health systems and regulatory structures that contribute to AMR, let’s look at some responsive interventions.
Sources: Kornfield et al. 2013; Olivier et al. 2010; Norris et al. 2005; WH0 1988; BBC News 2015; Leonardo Alves 2019; PEW 2011; Jacob 2018; CDC 2015.
Lack of antimicrobial use and drug resistance surveillance
Recall that surveillance, a means of collecting and monitoring AMR and antimicrobial use-related data that was referenced in Antimicrobial Resistance, part 1, is an important tool for containing AMR. It provides critical information on:
-
- Resistance levels in various organisms
- Usage patterns of various antimicrobials
This information helps such efforts as:
- Providing an effective treatment
- Designing an intervention
- Reducing the use of certain inappropriately prescribed antimicrobials
Surveillance systems that consistently and reliably collect and report quality data are a critical component in our ability to track resistance and mitigate factors contributing to AMR. Data can be used for several purposes:
-
- Characterize AMR and antimicrobial use trends
- Support national, regional, and international advocacy
- Inform public health policy
- Identify priority areas of intervention
- Guide treatment choices
- Monitor the effectiveness of AMR containment interventions
Most low- and middle-income countries have weak laboratory infrastructures and health information systems, which prevent robust monitoring of resistance and antimicrobial use. Other challenges to establishing surveillance systems include inadequate staff capacity to conduct laboratory tests, suboptimal communications between lab staff and clinicians regarding testing the susceptibility of a bacterial infection to a particular treatment, and limited availability of diagnostics and related commodities to correctly identify the source of illness.
A worldwide survey conducted by WHO in 2007 found that only 55% of low- and middle-income countries that responded had national-level reference laboratories for AMR surveillance. While Africa has the highest global incidence of tuberculosis (TB), only six African countries contributed data to the 2008 global report on TB drug resistance.
Challenges to creating and sustaining surveillance systems vary widely across countries. Such challenges include:
-
- Weak infrastructure and surveillance capacity
- Lack of standards
- Inadequate expertise
- Poor data management
- Insufficient networking and coordination
- Incomplete data from hospitals: little information available on antimicrobial use and resistance in the community
- Low digitalization
Without functional surveillance systems in place, health care providers cannot implement, measure, or evaluate the e!ectiveness of treatment strategies.
Sources: WHO 2015c; WHO 2012b; Nugent, Back, and Beith 2010; WHO 2009; Iskandar et al 2021; Kiggundu et al 2023
Health Systems and Regulatory Issues: Interventions
So far, we have discussed the role that a country’s health system and regulatory structure play in contributing to the development and spread of antimicrobial resistance. As you will recall, these factors include the following:
-
- Weak or nonfunctional multisectoral coordination on AMR
- Weak policy, guidelines, and regulation related to medicine supply and access
- Inability to prevent the presence of substandard and falsified medicines in the market
- Unrestricted pharmaceutical promotion
- Lack of medicine use and resistance surveillance
Now, we will discuss interventions designed to address these factors:
-
- Promoting multisectoral coordination and commitment to mitigating AMR at the national and local health system levels
- Adding or revising policies and guidelines and monitoring their adherence in health systems
- Implementing regulatory interventions in health systems
To get started, let’s take a look at one example and two case studies that demonstrate how AMR can be fought.
Multisectoral coordination and commitment at the national and subnational health system levels
Multisectoral coordination and commitment (including through resources) are required from governments and other sectors to combat the escalating public health threat of antimicrobial resistance.
WHO recommends that countries commit to a comprehensive, costed national plan with measures for accountability and civil society engagement.
As of November 2023, 178 countries had finalized a national action plan (NAP) on AMR that is aligned with the WHO Global Action Plan on AMR.
To go from plan to results, the national action plans must have complementary costed operational plans and monitoring and evaluation frameworks. The WHO said, “A costed NAP provides the foundation to identify funding gaps and mobilize additional resources to fill those gaps to allow for successful implementation of the activities.”
To help member countries implement their NAPs, WHO has published several practical tools, including a costing and budgeting tool, an implementation handbook, and a people-centered package of core AMR interventions. In 2023, the UN quadripartite (WHO, FAO, WOAH, and UNEP) also published a “Guidance to facilitate monitoring and evaluation for antimicrobial resistance national action plans.”
At country level, the USAID Medicines, Technologies, and Pharmaceutical Systems program worked with multisectoral groups in Kenya and Bangladesh to develop and finalize national monitoring and evaluation frameworks for their NAPs on AMR, which help identify issues around stakeholder accountability and move the NAP-AMR from policy to implementation.
Multidisciplinary cooperation and advocacy are also critical to ensuring the sustainability of results and continued progress when implementing interventions that address AMR. For example, USAID supported country-level AMR advocacy and containment initiatives in Ethiopia, Namibia, and Zambia.
In these three countries, multidisciplinary working groups brought national attention to the issue of AMR in several ways:
-
- Call-to-action meetings that bring stakeholders together around a common goal
- Sensitization activities such as newspaper articles
- Containment actions such as joint supervision visits to facilities involving stakeholders from across several sectors including academia, private sector, and government
Sources: Mabirizi et al. 2013; Joshi et al 2011; WHO 2011b; Joshi and Ludman 2015; Joshi et al 2018; Joshi et al 2021; Joshi et al 2023; WHO 2015c; Joshi et al 2015; WHO 2021a; WHO 2021b, WHO 2022, WHO 2023b, WHO 2023a, WHO 2023c.
Case Study
The WHO developed the Joint External Evaluation (JEE) tool in 2016 (revised in 2018 and 2022) for countries to monitor their progress on International Health Regulations (IHR). The GHSA initiative also uses this JEE tool to advance the various IHR technical areas, including AMR. One of the indicators within the AMR technical area included in the JEE tool (2018 and 2022) is on multisectoral coordination on AMR (See Part 1 for more details).
In 2019, to complement the JEE, WHO published Benchmarks for IHR Capacities that lays out the activities needed to increase country capacity in the areas measured in the JEE including multisectoral coordination on AMR. (See Part 1 for more details). The USAID Medicines, Technologies, and Pharmaceutical Services program has worked with 13 countries to use the benchmarks tool as a way to prioritize their activities and measure progress. In 2023, WHO published an updated version of the benchmarks tool as “WHO Benchmarks for Strengthening Health Emergency Capacities.”
The next page features a multi-country case study on fostering MSC on AMR.
Source: WHO 2021c; WHO 2022b; Joshi et al. 2023; WHO 2023d
Did you know?
WHO Ethical Criteria for Medicinal Drug Promotion
In 1988 the WHO published guidelines on ethical criteria on pharmaceutical promotion. These guidelines cover various aspects of drug promotion, including advertisements to health providers and the general public, activities of medical representatives, distribution of free medicine samples, packaging and labeling, and the information included in package inserts.
Source: WHO 1988
Case Study
USAID Medicines, Technologies, and Pharmaceutical Services (MTaPS) has worked with more than a dozen countries to build multisectoral coordination on AMR (MSC-AMR).
Previous AMR containment efforts focused mainly on the human health sector. But the One Health nature of AMR containment calls for a coordinated multisectoral effort. To help countries establish strong MSC-AMR, MTaPS tailored activities to each country’s situation and their JEE scores. This approach included the following:
-
- Identify strengths, gaps, and priorities for MSC-AMR
- Help finalize and operationalize NAPs-AMR
- Strengthen leadership and build capacity of MSC-AMR governance structures
- Facilitate coordination of AMR activities within and across sectors
Examples of countries’ achievements from 2019 to 2020 using this approach include the following:
-
- Representatives from multiple sectors including human and animal health finalized their NAPs- AMR (Burkina Faso, Côte d’Ivoire, and Mali); developed a costed operational plan (Cameroon); and created a monitoring and evaluation framework (Kenya and Bangladesh)
- Tanzania developed a multisectoral communication strategy to increase awareness and understanding of AMR across all sectors
-
- Ethiopia established a three-tiered national AMR governance and coordination structure that includes six multisectoral technical working groups
-
- Nine countries created or revitalized multisectoral infection prevention and control (IPC) or antimicrobial stewardship (AMS) technical working groups (TWGs) who developed policies and guidelines; assessments and action plans; and training materials, including eLearning modules and courses. When the COVID-19 pandemic hit, the national IPC TWGs were able to respond quickly by creating COVID-19 treatment guidelines and drafting or adapting IPC guidelines to incorporate COVID-19 considerations.
MTaPS published two articles with more detail on our approaches to strengthening MSC-AMR and lessons learned in multiple countries:
-
- Strengthening Multisectoral Coordination on Antimicrobial Resistance: A Landscape Analysis of Efforts in 11 Countries in Journal of Pharmaceutical Policy and Practice (Joshi et al., 2021)
- Moving from assessments to implementation: promising practices for strengthening multisectoral antimicrobial resistance containment capacity in One Health Outlook (Joshi et al. 2023).
Sources: Joshi, Hafner, Twesigye, et al 2021; Joshi, Alombah, Konduri, et al. 2023.
Policies, guidelines, and surveillance in the health system
While self-governance is important for preventing misuse of antimicrobials within the organizations responsible for using antimicrobials, enforceable regulations created at the government level also play a role, so that true enforcement can be accomplished.
The government and other stakeholders are responsible for providing sound policies and guidelines to help prescribers use antimicrobials appropriately:
-
- Developing and implementing policies and programs to ensure adequate access to essential medicines, including antimicrobials, and establishing systems to monitor their availability, affordability, and utilization
- Establishing systems for both AMR surveillance and antimicrobial consumption and use and improving the use of surveillance data in decision-making
- Implementing appropriate policies and standards regarding continuing professional education for re-licensing of health care providers and accreditation of health facilities
- Developing and implementing up-to-date national standard treatment guidelines and essential medicines lists including AWaRe categorization of antibiotics, coupled with training and supervision of health care providers
- Promoting disease prevention measures so that medicines and treatment are not needed (e.g., sanitation to prevent diarrhea, bed nets to prevent malaria, and pneumococcal vaccine to prevent pneumonia)
-
Global Antimicrobial Resistance and Use Surveillance System (GLASS)
In 2015, WHO launched the GLASS initiative, which provides a standardized approach to collect, analyze, and share AMR surveillance data. GLASS promotes a surveillance system that includes epidemiological, clinical, and population-level data in addition to laboratory data. As of December 2021, 114 countries were enrolled in GLASS.
Source: WHO 2021c -
WHONET
WHO has developed a simple software called WHONET for AMR surveillance laboratories. This free software, available in 44 languages, has been used by 2,300 hospitals and public health, animal health, and food laboratories in over 130 countries to support local, national, regional, and global surveillance programs with data collection, analysis, reporting, and encryption.
-
WHO Model Lists of Essential Medicines
WHO has developed model lists of essential medicines for adults and children and revises them every two years. These model lists serve as guides for the development of national and institutional-specific lists.
Since 2017, the WHO list has incorporated AWaRe (Access, Watch, Reserve) categories for antibiotics, which is a valuable tool to monitor and improve antibiotic use and stewardship. The next page includes more information. -
Hospital antimicrobial use studies in Tanzania and Uganda
The USAID Medicines, Technologies, and Pharmaceutical Systems program supported 6 hospitals in Tanzania and 13 hospitals in Uganda to determine the prevalence and factors of antimicrobial use using WHO’s point-prevalence survey methodology. The Tanzania results, based on records of 948 patients, showed that use of antibiotics was high (63%) with only two patients treated based on antibiotic susceptibility testing. However, almost 98% of 991 antibiotics prescribed were from the WHO Access list. In Uganda, data from 1,077 patients showed that 74% of patients were on at least one antibiotic, a high proportion (37%) of which were from the WHO Watch list, primarily due to the high use of ceftriaxone, which was prescribed most frequently. Additionally, adherence to the Uganda clinical guidelines was low (30%), and a high proportion (88%) of antibiotics were administered parenterally (not via mouth). Such findings help inform the prioritization and design of evidence-based AMS activities.
Source: Seni et al 2020; Kiggundu et al 2022
Regulatory interventions in health systems
In addition to policies and guidelines, governments must also provide legal and regulatory frameworks and strategies for containing antimicrobial resistance. However, qualities such as political commitment and good governance are necessary to ensure that such regulatory and policy frameworks are properly implemented and enforced.
Key regulatory interventions include the following:
-
- Controlling the circulation of substandard and falsified antimicrobials by, for example, mandating retail outlets to purchase from an approved source
- Granting marketing authorization only to those antimicrobials that meet international standards of quality, safety, and e#cacy
- Strengthening registration of medicines and pharmaceutical dispensing outlets in the country
- Limiting over-the-counter availability of antimicrobials
- Separating medicine prescribing and dispensing functions
- Controlling pharmaceutical companies’ unethical promotional activities
Although this course primarily focuses on interventions related to the human health sector, AMR containment cannot occur without regulatory strengthening in the animal sector (e.g., prohibiting the use of antimicrobials for growth promotion in animals raised for food) and the environmental sector (e.g., developing and enforcing clear regulations on the disposal of hospital discharge and waste from the production and remains of antimicrobial medicines).
Sources: WHO 2012d; Ming et al 2019
A review of 36 studies from the US found that pharmaceutical industry payments to physicians affected how they prescribed. Despite concerns regarding industry influence on medical practice, such payments are common. Federal regulation requires the disclosure of payments, but does not attempt to reduce them. The primary barrier to reform has been physician opposition, potentially rooted in the belief that such payments do not affect their practice.
Source: Mitchell et al. 2021
In 1988, the forty-first WHO World Health Assembly passed a resolution (WHA41.17) on ethical criteria f or medicinal drug promotion. The criteria cover different aspects of drug promotion, including advertisements aimed at health providers and the public, activities of medical representatives, and information included in package inserts.
Source: WHO 1988
New page
Hospitals
Overview
-
Learning objectives
By the end of this session, you will be able to identify challenges that hospitals face, particularly those in low- and middle-income countries (LMICs), that can facilitate the development and spread of antimicrobial resistance, including the following:
-
- Poor infection prevention and control leading to health care-associated infections
- Poor diagnostic laboratory facilities
- Gaps in antimicrobial stewardship programs
You will also be able to recognize interventions to address these factors at the facility level focusing on multiple areas:
-
- Preventing and controlling hospital-acquired infections
- Strengthening diagnostic laboratories
- Establishing an antimicrobial stewardship program
Poor infection prevention and control
As you learned in the previous session, infection prevention and control (IPC) is a key element for AMR containment, pandemic preparedness, and universal health coverage.
The COVID-19 pandemic exposed how seriously unprepared and inadequate countries’ IPC systems are. COVID-19 experiences showed that traditional IPC plans and training have little focus on pandemic preparedness, including transmission-based precautions.
These weaknesses also contribute to the worryingly high prevalence of health care-associated infections (HAIs) in LMICs of 15.5%. HAIs are primarily acquired in hospitals, in which case they are referred to as hospital-acquired or nosocomial infections.
Most HAIs are caused by drug-resistant microorganisms. Many of the most well-known and threatening resistant bacteria such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and carbapenem-resistant enterobacteriaceae (CRE) are primarily acquired in hospitals.
HAI significantly increases morbidity, mortality, and costs. In the United States alone, such infections are estimated to cause more than 89,000 deaths annually. However, the majority of HAIs are preventable. For example, up to 70% of catheter-associated bloodstream and urinary tract infections may be prevented with current evidence-based strategies.
Some preventable factors that contribute to hospital-acquired infections include the following:
-
- Lack of infection prevention and control (IPC) policies and guidelines and poor practices including prolonged and inappropriate use of invasive devices, lack of proper isolation precautions, waste disposal, and hygienic measures—good hand hygiene practices, for example, substantially decrease HAIs, and yet compliance is commonly poor
- Lack of IPC-related supplies and consumables such as soap, alcohol-based hand rubs, and personal protective equipment
- Intensive and irrational use of antibiotics leading to development of multidrug-resistant organisms
Sources: Allegranzi et al 2011; Umscheid et al. 2011; Haque et al. 2018
Glossary Term:
Healthcare-associated infections Vancomycin-resistant enterococci
carbapenem-resistant enterobacteriaceae
Did you know?
Fewer infections in a hospital setting means less need for antimicrobials and therefore lower selective pressure for infectious agents to develop resistance.
Highlight
Infection prevention and control (IPC) is a ‘best buy’ with high returns on investment:
-
- IPC reduces health care-associated infections such as catheter-associated bloodstream infections, catheter-associated urinary tract infections, surgical site infections, and ventilator- associated pneumonia by 35 to 70%
- Hand hygiene, antimicrobial stewardship, and environmental hygiene can reduce AMR by 85%
- Hand and environmental hygiene in health facilities reduce AMR-related deaths by more than 50%
- Each dollar invested in hand hygiene can save 16.5 US dollars
Source: WHO 2022c; OECD 2018
Poor diagnostic laboratory facilities
Diagnostic uncertainties drive irrational antimicrobial use and antimicrobial resistance. When a patient presents symptoms to a health care provider, it is not always clear if the cause is an infection. Without diagnostic testing, it may not be possible to identify the exact infectious agent to treat.
Lack of diagnostic support or slow and poor-quality laboratory test results force prescribers to base their decisions on empirical judgments alone. Often, this results in writing prescriptions for antimicrobials without diagnostic testing “just in case.”
Laboratories need to accurately identify infections and antimicrobial susceptibility to guide treatment. They also need to participate in resistance surveillance to support AMR containment efforts.
Unfortunately, hospital laboratories in many resource-constrained settings often lack trained personnel, infrastructure, supplies, and quality-assurance mechanisms.
Source: Laxminarayan et al. 2013
Gaps in antimicrobial stewardship programs
Fifty percent or more of antimicrobial use in hospitals is inappropriate. Antimicrobial stewardship (AMS) programs help correct this problem using a systematic approach supported by policies, structures, and interventions.
Hospital antimicrobial stewardship programs are well-recognized and implemented in high-income countries. However, most hospitals in resource-constrained settings do not generally have organized stewardship initiatives. LMIC hospitals often face other interrelated constraints such as lack of diagnostic services and antimicrobial availability. The USAID Medicines, Technologies and Pharmaceutical Services (MTaPS) program has supported 13 LMICs to enhance AMS as part of their Global Health Security Agenda efforts to help contain AMR. When MTaPS started in these countries, more than two-thirds of them were at level 1 or 2 on their baseline Joint External Evaluation score in this area. This meant they had no or only limited capacity in AMS.
Now let’s look at some interventions that hospitals can use to help prevent the development and spread of AMR.
Sources: McKenzie, Rawlins, and Del Mar 2013; Health Protection Surveillance Centre 2009; Dellit et al. 2007; CDC 2014b; WHO 2019c; MTaPS 2020
Glossary Term:
Antimicrobial stewardship
Did you know?
Overuse of antibiotics and inappropriate use of personal protective equipment (PPE) are challenges during infectious disease outbreaks, highlighting the importance of AMS and rational use.
Source: Vaughn et al. 2021
Interventions at the facility level
IPC program core components and assessment tools
WHO published the eight core components of national- and facility-level infection prevention and control (IPC) programs.
-
- Core component 1: Infection prevention and control programs
- Core component 2: Infection prevention and control guidelines
- Core component 3: Infection prevention and control education and training
- Core component 4: Health care-associated infection surveillance
- Core component 5: Multimodal strategies
- Core component 6: Monitoring, audit, and feedback of infection prevention and control practices
- Core component 7: Workload, staffing and bed occupancy at the facility level
- Core component 8: Built environment, materials and equipment for infection prevention and control at the facility level
WHO recommends the above eight core components for facility-level IPC actions and the first six for national-level actions. Minimum Requirements for Infection Prevention and Control describes IPC standards that should be in place at the national and facility level to provide minimum protection for patients, health care workers, and visitors.
A clear lesson learned from previous outbreaks and the latest COVID-19 pandemic is that improving IPC must be part of a health systems strengthening approach for longer-term capacity building, sustainability, and resilience. Another lesson is that IPC efforts should emphasize not only standard precautions, but also transmission-based precautions to enhance preparedness or readiness for future infectious disease outbreaks, which often occur quickly.
To monitor how well countries are adhering to the IPC core components, WHO recommends that countries use its Infection Prevention and Control Assessment Tool 2 (IPCAT2) to evaluate their national IPC programs and its Infection Prevention and Control Framework (IPCAF) and Hand Hygiene Self-Assessment Framework (HHSAF) tools to assess health facilities.
The WHO benchmarks for health emergency capacities emphasizes the use of these tools for improving IPC programs and practices. Through Global Health Security Agenda support, the USAID Medicines, Technologies and Pharmaceutical Services (MTaPS) program has collaborated with multiple LMICs to carry out national and facility assessments using these WHO tools, and based on findings, supported interventions to improve IPC practices. Results from these MTaPS collaborations show notable results. For example, as of September 2021, 71 facilities across multiple countries had completed baseline and repeat assessments, and the repeat assessment scores in 37 (52%) of those facilities had increased by at least one capacity level compared to their baseline scores. The next page shows a country example of such improvements.
Sources: WHO 2019d; MTaPS 2021a; MTaPS 2021b; Joshi et al 2023
Country examples of IPC and WASH improvements
Hospital staff can influence infection prevention and control through a number of activities. For example, of five hospitals in Senegal that MTaPS supported, three improved their IPC capacity by one level, and two increased two levels by implementing multimodal strategies.
IPCAF scores of hospitals
|
Hospitals |
IPCAF baseline score/800 and capacity level February-March 2021 |
IPCAF follow-up score/800 and capacity level October 2021 |
|---|---|---|
|
Level 1 Mbour Hospital |
167.5 Inadequate |
455 Intermediate |
|
Level 2 Fatick Hospital |
315 Basic |
513 Intermediate |
|
Level 2 Kaffrine Hospital |
380 Basic |
535 Intermediate |
|
Level 3 Touba Hospital |
310 Basic |
450 Intermediate |
|
Level 3 Aristide le Dantec Hospital |
322 Basic |
692.5 Advanced |
Efforts to improve IPC practices go hand-in-hand with improving water, sanitation, and hygiene (WASH), which generally falls under the WHO IPC core component #8. In Tanzania, MTaPS collaborated with local stakeholders to conduct a WASH assessment at four supported hospitals to establish WASH improvement needs. MTaPS oriented staff responsible for WASH and IPC at three hospitals on the IPC guidelines and reviewed the assessment results with them, which had a significant effect; for example, facilities began to take action immediately, especially on things that did not require resources—hospitals installed elbow-driven handwashing sinks and repurposed unused equipment, and one hospital collaborated with the implementing partner, WaterAid, to install a water storage tank.
Sources: Goredema et al 2015; MTaPS 2020; WHO 2016; Joshi et al 2023
Did you know?
The WHO Guidelines on Hand Hygiene in Health Care provide a thorough review of evidence on hand hygiene in health care and specific recommendations to improve practices and reduce transmission of pathogenic microorganisms to patients and health care workers. Similarly, the WHO Water and sanitation for health facility improvement tool (WASH FIT) is a continuous improvement framework for primary health facilities in low- and middle-income countries to improve water, sanitation, and hygiene.
Highlight
As part of its podcast series called “Between Two Baobab Trees” looking at integrating climate into health programming, episodes 6 and 7 delve into the intersection of WASH and water security, which is a major concern related to climate change.
Strengthening diagnostic laboratories
Given the information already presented throughout this course, it’s no surprise that diagnostic laboratories in hospitals provide important information. They contribute to antimicrobial resistance containment in two ways:
The WHO Global Strategy for Containment of AMR (2001) recommends that diagnostic laboratories in hospitals meet the following requirements:
Ensure access to microbiology laboratory services that match the level of the hospital (e.g., secondary, tertiary)
Ensure performance and quality assurance of appropriate diagnostic tests and timely and relevant reporting of results
Ensure that laboratory data are recorded and used to produce AMR surveillance reports with feedback to prescribers and to the hospital's infection control program
Quality-assured hospital surveillance data should contribute to national and global AMR surveillance programs such as the Global Antimicrobial Surveillance System (GLASS).
Additionally, WHO recommends extending access to rapid diagnostic testing.
Sources: WHO 2001; WHO 2011f
Antimicrobial stewardship programs
An elective approach to optimizing antimicrobial use in hospitals involves a systematic, organized antimicrobial management program, also known as antimicrobial stewardship. Antimicrobial stewardship and complementary infection control and surveillance programs are considered key strategies to contain AMR in hospitals.
Recall from earlier that WHO names six core elements of antimicrobial stewardship programs in health facilities: leadership commitment, accountability, and responsibilities; antimicrobial stewardship actions; education and training; monitoring and surveillance; and reporting and feedback. Properly designed and implemented antimicrobial stewardship programs have consistently demonstrated success, with reductions in inappropriate antimicrobial use by as much as 22% to 36%. They improve patient outcomes and decrease AMR, adverse events, and costs.
In Jordan, the USAID-funded Systems for Improved Access to Pharmaceuticals and
Services program helped three hospitals implement antimicrobial stewardship initiatives to strengthen antibiotic prophylaxis during cesarean sections. Each hospital conducted a medicine use evaluation and established a continuous quality improvement system to improve clinical practice.
The efforts led to the use of standardized prophylaxis protocols and procedures, substantial improvements in the correct administration of antibiotics, and cost savings.
Because hospital antimicrobial stewardship programs require multidisciplinary teamwork, drug and therapeutics committees (DTCs) are appropriate bodies to oversee and support AMS programs. WHO recommends DTCs as a mechanism to support AMR containment efforts and USAID has supported DTC training and follow-up technical assistance efforts to enhance rational medicine use and AMR containment activities in resource-limited settings.
To support health facilities’ efforts to improve AMS programs and practices, WHO published a practical toolkit for use in low- and middle income countries.
The next page features a case study on an initiative in six hospitals to improve antibiotic prescribing.
Sources: WHO 2019c; McKenzie, Rawlins, and Del 2013; Gammouh and Joshi 2013; Australian Commission on Safety and Quality in Healthcare 2011; Dellit et al. 2007; Getahun et al 2015
Glossary Term:
Drug and therapeutics committee
Did you know?
The following national AMS core elements lead to an enabling environment that facilitate AMS actions at all levels, including facilities:
-
- National plan and strategies
- Regulations and guidelines
- Awareness, education, and training
- Supporting technologies and data
Source: WHO 2019c
Case study: Using a quality-improvement approach to improve prescribing in six hospitals
USAID Medicines, Technologies, and Pharmaceutical Services (MTaPS) worked with staff from six hospitals in Uganda to use continuous quality improvement (CQI) approaches to improve the use of antimicrobials in three common scenarios:
-
- Urinary tract infections (UTIs)
- Upper respiratory tract infections (URTIs)
- Surgical antibiotic prophylaxis (SAP).
The first phase of the initiative was to determine the existing practices for each facility using the WHO toolkit of health facility core elements for AMS programs. The development of the hospitals’ AMS work plans focused on defining AMS programs’ structures, systems, and roles including appointing AMS subcommittees.
The second phase comprised the intervention to improve antibiotic use in the three treatment scenarios. Each hospital was trained on how to develop a CQI plan for AMS that was based on baseline survey results and antimicrobial use surveillance. The hospital teams also developed mentorship guides to build capacity in the hospitals and received extensive communication materials. Training focused on adhering to the Uganda Clinical Guidelines for URTIs and UTIs, and 2,244 health workers were mentored during 90 site visits and 38 health facility training activities.
After the interventions, all six hospitals had improved their AMS core element scores. The chart below illustrates the scores for each element.
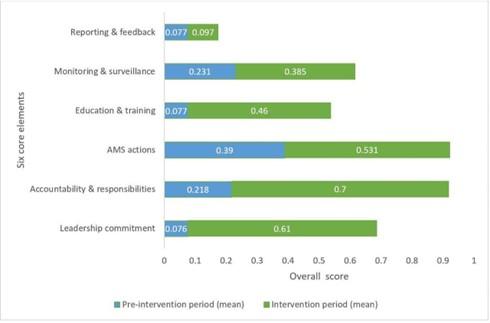
Using methods on investigating antimicrobial use in hospitals, 100 prescriptions for patients diagnosed with either a URTI or UTI and those who had cesarean sections were analyzed each quarter both before and after the interventions. Based on 7,037 patients diagnosed with UTIs, the proportion of patients receiving one antibiotic for UTI treatment rose from 48% during the pre- intervention to 73.2% with a 19.2% reduction in the number of antimicrobials per patient treated during intervention. Based on 5,424 patients diagnosed with URTI, the proportion receiving no antimicrobials increased from 26.3% at pre-intervention to 53.4% during intervention. There was a 20.7% reduction in the mean number of antimicrobials per patient. Among the 4,291 surgical patients, 49.5% received SAP during the pre-intervention versus 50.5% during the intervention.
This study adds lessons suitable for other resource-constrained countries on how to use CQI approaches to improve antibiotic use. In addition, ministries of health can recommend adopting these study approaches for use at the national level and also mandate AMS interventions.
Source: Kiggundu R et al. 2023.
New page
Containing AMR in the global community
So far we have looked into causes and containment of AMR; issues with prescribing and dispensing antimicrobials; and the role of patients and communities, health systems, regulations, and hospitals in both facilitating and containing AMR.
-
Learning objectives
At the end of this session, you will be able to identify the global community’s additional approaches to contain AMR including:
-
- Developing new antimicrobials
- Developing new vaccines and rapid diagnostic tests
- Mitigating issues caused by globalization and societal shifts
- Putting into place international strategies to contain AMR
Development of antimicrobials
Interventions can preserve the effectiveness and life span of antimicrobials, but resistance cannot be prevented entirely. Therefore, intense efforts are needed to stimulate the development of new antimicrobials.
As discussed in the GHeL AMR Part 1 course, the rate of discovery for new antibiotics and other antimicrobials is very slow, thus, it is paramount that existing antimicrobials are used appropriately and rationally (preserving their effectiveness) alongside efforts to discover completely new—or “novel”—antimicrobials.
Decades ago, the development and market release of antimicrobials were considered highly rewarding for the pharmaceutical industry. However, this is no longer the case. The pipeline for new antimicrobials is almost dry.
In the last several decades, only a few antibiotics with truly novel mechanisms of action have become available. WHO’s 2020 review stated that of the 43 products in the clinical pipeline, only 7 were not derivatives of existing products. Pharmaceutical companies have shied away from research and development of antimicrobial medicines for infectious diseases in favor of medicines for chronic diseases because they yield greater profits.
Enabling environments and incentives are needed to encourage investment in antimicrobial development. The WHO Global Action Plan (GAP) on AMR calls for new processes to facilitate renewed investment in research and development of new antibiotics. Examples could include:
-
- Government financing for basic research and clinical trials
- Prioritizing investment in anti-infection research
- Research and development tax credits
- Fast-track product approvals
- Advance market commitments
- Prizes for research breakthroughs or finished products
- Patent buy-outs to provide affordable access in low-resource settings
- Uncoupling research and development costs from product price and sales volume to facilitate equitable and affordable access to new medicines, diagnostic tools, and vaccines
Cooperation among industry, government bodies, and academic institutions is essential in the search for new medicines. Such private-public partnership e!orts are increasingly being used to speed up antimicrobial development. Initiatives include the Global Antibiotic R&D Partnership (GARDP) to develop innovative treatments and the AMR Action Fund that aims to use global pooled funding to fast-track antibiotic development.
Sources: WHO 2023a; World Economic Forum 2013; Goldman, Compton, and Mittleman 2013; WHO 2012b; WHO 2011f; Nugent, Back, and Beith 2010; WHO 2001; WHO 2015; WHO 2021e; WHO 2021f
Glossary Term:
Drug pipeline
Development of vaccines and rapid diagnostic tests
Vaccines complement antimicrobial resistance containment by preventing infections and therefore reducing the need to use antimicrobials. Rapid diagnostic tests (RDTs) play a similarly complementary role; they can help health care providers make quick point-of-care diagnoses and decisions on whether to administer antimicrobial therapy and, if needed, what spectrum of antimicrobial therapy is appropriate.
For that reason, adequate support for the development of vaccines and RDTs should be part of a comprehensive global strategy to contain AMR, along with investments in the discovery of new antimicrobials.
WHO recommends confirmation of malaria before antimalarial drug use and supports universal access to malaria testing. People in many countries rely on the private sector—particularly retail drug shops—for malaria treatment. As a result, malaria control strategies such as diagnostic testing increasingly engage the private sector. Several countries are working to increase people’s access to RDTs through drug shops. Increased access to RDTs will make the job of prescribers easier–decreasing the need for clinical diagnosis of patients and providing tangible evidence to link to treatment.
A new malaria vaccine (RTS,S) may be a game changer for children under five who are most at risk. WHO has included the vaccine in the updated guidelines for malaria (February 2022) and recommends its use in areas of moderate-to-high P. falciparum malaria transmission. Reducing the incidence of malaria in children also reduces the need to prescribe and use antimalarials.
The RDT Xpert MTB/RIF can detect tuberculosis (TB) and resistance to rifampicin within two hours, which significantly reduced delays in TB diagnosis and treatment when it was introduced. In its latest guidelines, WHO added new RDT technologies able to detect TB drug resistance in patients with certain characteristics. For example, the RDT Xpert MTB/RIF Ultra is more sensitive in patients with HIV, while two other RDTs detect isoniazid-resistant, rifampicin-susceptible TB that is often undiagnosed and cases with resistance to isoniazid and second-line anti-TB agents. The availability of more sensitive RDTs will make it possible to detect more multidrug-resistant TB cases in a wider population, enabling them to get on treatment more quickly, thereby reducing community spread.
Diagnostic stewardship oversights facilitating availability and use of RDTs at the point of care can greatly assist in convenient and quick differentiation between infections of viral and bacterial origins and also in some cases presence of resistance. This helps in judicious selection and use of antimicrobials and thus contributes to AMR containment.
Diagnostic stewardship contributes to a larger antimicrobial stewardship program by reducing false-positive testing results (which lead to overuse of antimicrobials) and increasing the detection of true-positive cases who should receive appropriate treatment.
Once developed, new antimicrobials, vaccines, and diagnostic tests will need strategies to maximize their diffusion, uptake, and appropriate use.
Sources: WHO 2012c; Schellenberg 2013; WHO 2015b; Cohen et al. 2015; WHO 2021g; WHO 2021h; WHO 2022c
Glossary Term:
Multivalent pneumococcal conjugate vaccine Point-of-care diagnosis
Rifampicin [or Rifampin] (R)
Xpert MTB/RIF isoniazid
Did you know?
Use of multivalent pneumococcal conjugate vaccine in infants and children not only prevents infections, but also significantly reduces drug resistance in Streptococcus pneumoniae.
Source: WHO 2012b
Did you know?
Introduction of a universal influenza immunization program in the Ontario province of Canada resulted in a 64% greater decrease in influenza-associated respiratory antibiotic prescriptions than in provinces that maintained programs targeted to high-risk groups and their contacts.
Source: Kwong et al. 2009
Globalization and societal shifts
As our world grows smaller through globalization, and as societal structures change, conditions that contribute to the development and spread of antimicrobial resistance will continue to arise.
-
Globalization
prompts large volumes of international travel, trade, and migration, all of which can spread resistant pathogens to distant places
-
Long-term care facilities
are major health care providers. Infections, including those with drug- resistant pathogens, are common in these settings
-
Prisons and other group-living situations
create environments that promote infections and drug resistance
-
Urbanization
causes overcrowding and poor sanitation, both of which promote the development and spread of AMR. For example, multidrug-resistant TB is a major challenge in several densely populated cities including Baku, Cape Town, Dhaka, Mumbai, and Tashkent
Mitigating issues caused by globalization and societal shifts requires multi-pronged strategies and actions. Interventions include immunization, infection prevention and control, food hygiene, antibiotic stewardship, surveillance systems, and reducing person-to-person spread through screening, treatment, and behavior change.
Additionally, strong global cooperation and collaboration are necessary to improve and standardize international disease surveillance and to prevent, detect, and respond to infectious diseases threats. International Health Regulations (IHR) and Global Health Security Agenda (GHSA) are examples of collaborations that aim to improve local, national, regional, and global health security through the spirit of One Health.
The COVID-19 pandemic has shown the importance of investments in health security and pandemic preparedness. There is growing recognition that AMR has the potential to become a similar pandemic without concerted global actions. It is critical to address AMR not only as a threat to individuals and communities but also to global health security. Because of this, WHO’s Joint External Evaluation (JEE) and benchmarks for strengthening health emergency capacities tools, which are used to advance IHR, include AMR as one of the 19 technical areas. GHSA also uses these tools to advance its AMR action package.
Sources: WHO 2014a; CDC 2013b; Alirol et al. 2010; Macpherson et al. 2009; Esposito et al. 2007
Glossary Term:
Globalization
Did you know?
On any given day, the world's prisons hold an estimated 8 to 10 million prisoners. The level of TB in prisons may be up to 100 times higher than in the general population. High levels of multidrug-resistant TB (up to 24%) have been reported by some prisons.
Source: WHO 2014b
International strategies for containing AMR
WHO has labeled antimicrobial resistance a global public health crisis; therefore, efforts to contain this crisis must come from all corners of the world.
Some of the international strategies for containing AMR include the following:
-
- Commitments to and international coordination for advocacy and actions against AMR using a One Health approach
- Innovative national and international partnerships to accelerate the development of new antimicrobials, vaccines, and rapid diagnostic tests
- Worldwide initiatives promoting antimicrobial stewardship and infection control programs in both human and animal sectors
- Global, regional, and national networks for surveillance of antimicrobial resistance and use
- Inspections of pharmaceutical manufacturing plants jointly conducted by international teams to ensure trust in the findings and results
- Collaborations to control the circulation of falsified antimicrobials
- Prioritization and implementation of AMR research in a coordinated manner
- Donor support for AMR containment strategies and actions in low- and middle-income countries
Sources: Laxminarayan et al. 2013; Carlet et al. 2012; WHO 2012b; WHO 2001; Bertagnolio et al 2024
Conclusion
Eighty-five years ago, we lived in a pre-antimicrobial era. Then came the miracle medicines that have saved countless lives. But now, we are in imminent danger of losing these gains and entering an era of totally untreatable infections. If we do not act now and act seriously about AMR, we will soon be living in a post-antibiotic era or facing a multidrug-resistant infectious disease pandemic.
Political commitments, leadership, stewardship, advocacy, and multisectoral coordination are vital components of a sustainable strategy to effectively contain AMR. All stakeholders—governments, nongovernmental organizations, academia, consumer groups, professional societies, the pharmaceutical industry, and international bodies—must come together to address this common global threat. Since AMR cuts across and impacts human, animal, and environmental health, a One Health approach is fundamental to tackling this public health crisis. More needs to be done, especially in low-resource settings, if we are to truly contain AMR on a global scale.
Our efforts should be multi-pronged—including increasing awareness and education and improving AMR/antimicrobial use surveillance, antimicrobial stewardship, and infection prevention and control. Additionally, efforts need to foster innovative ways of developing new antimicrobials, vaccines, and rapid diagnostics.
Because AMR issues are cross-cutting by nature, interventions to contain resistance will not only add value to specific disease-related activities, but also benefit the overall management of infectious diseases and improve global health security. Containing AMR is also critical to the success of global agendas of universal health coverage and Sustainable Development Goals, and AMR containment activities should be mainstreamed into such initiatives at global, regional, and country levels.
Antimicrobial Resistance, part 1 and part 2, have explained AMR and the extent of its threat to global public health, described AMR’s current relevance to diseases of major public health importance worldwide, and explained the factors that contribute to AMR and the interventions available to address them.
Source: Joshi et al. 2023
Ideas in action
Take the information gained from Antimicrobial Resistance Part 1 and 2 back to the workplace to determine how AMR affects your organization and its work, and what can be done to contain it. What are specific actions you can take to contribute to the fight?
These materials were adapted from the Global Health eLearning Center, U.S. Agency for International Development.
Image credits
Unless otherwise noted, images are from Adobe Stock.