

- Most often presents 3–7 days after aSAH, but may occur up to 21 days after the bleed.
- S/sx: New focal neuro deficits, altered consciousness, new or worsening headache, visual changes, etc.
- Varies by location and etiology.
- Focal neurologic deficits (FNDs) common, especially if stroke, malignancy, or trauma.
- Brainstem lesions may cause autonomic instability or altered consciousness.

- “Triple H therapy” = addresses hypertension, hemodilution, and hypervolemia
- Goal: Increase mean arterial pressure (MAP) while decreasing blood viscosity.
- Increasing MAP = pressors (phenylephrine, norepinephrine, dopamine).
- Prevention of vasospasm: Calcium channel blockers (incl. nimodipine) seem to improve neurologic outcomes; questionable evidence to support an overall reduction in mortality.
- Goal: Increase mean arterial pressure (MAP) while decreasing blood viscosity.
- If not averted/managed, vasospasm can lead to poorer functional outcomes and, potentially, demise in an otherwise-survivable injury.
Within the cerebra, cerebellum, or brainstem.
May result from a number of different insults, ranging from hemorrhagic stroke to infection, malignancy, vascular compromise (e.g. amyloid angiopathy), and trauma (incl. Coup/contrecoup injury). HTN usually involved.


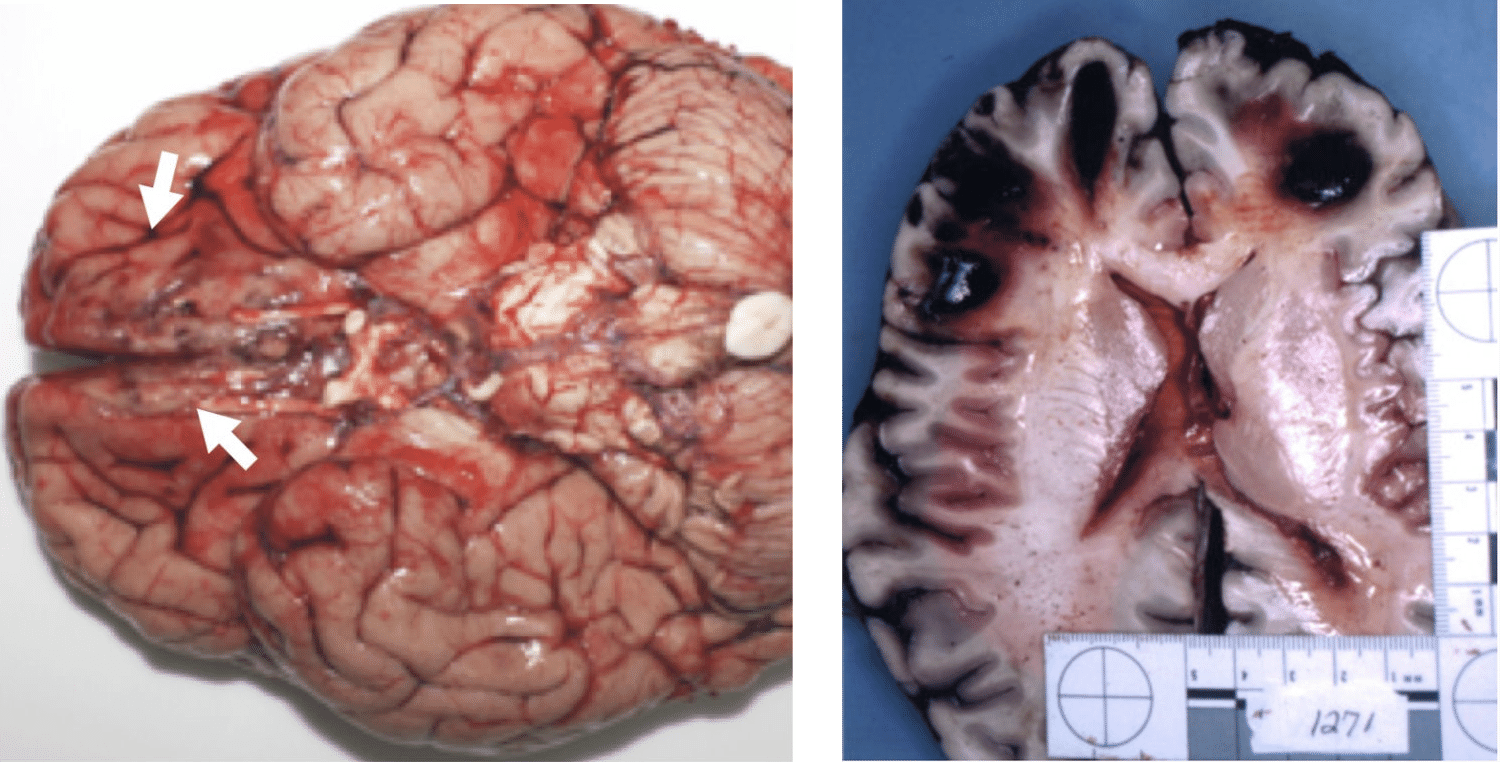
- Blood within brain parenchyma (cerebra, cerebellum, brainstem).
- +/– visible trauma (e.g. skull fx, penetrating injury)

CT
- Generally not sensitive enough to demonstrate extent of injury; clinical presentation may be significantly worse than imaging findings.
MRI
- MRI (diffusion weighted/DWI): Study of choice for DAI.
- May see irregularities (including hyperintensity) at gray-white matter junction.
- Edema often present.

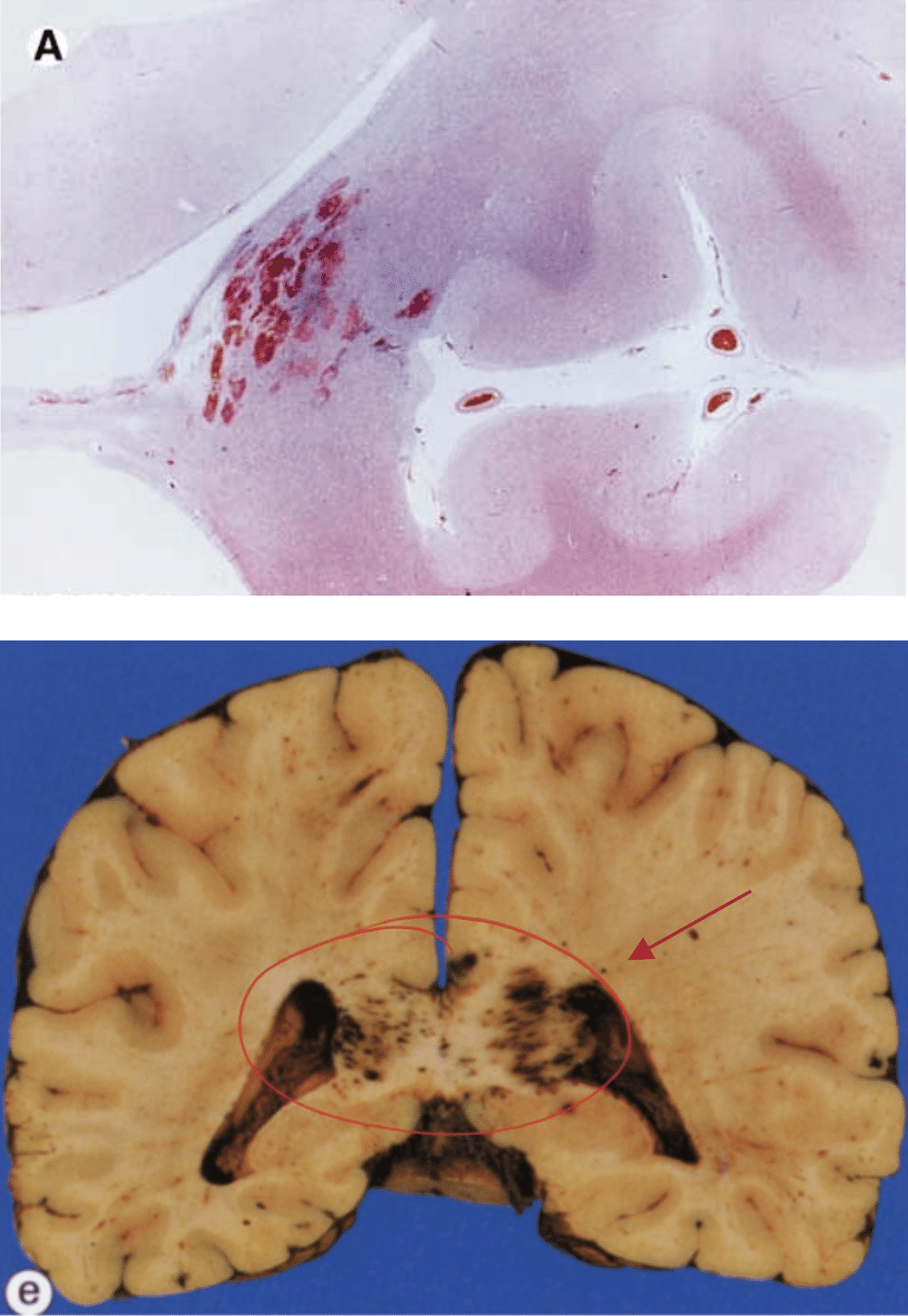
- May see petechial hemorrhages at gray-white matter junction.
- Cerebral edema may be pronounced.
- Some debate surrounding the necessity of observing an associated coup-contrecoup injury.
- Increasing severity of injury is associated with depth of white matter damage.
- Corpus callosum involvement common.
- As generated torque increases, injury to deeper brain structures occurs (thalamus, midbrain, pons, and medulla