

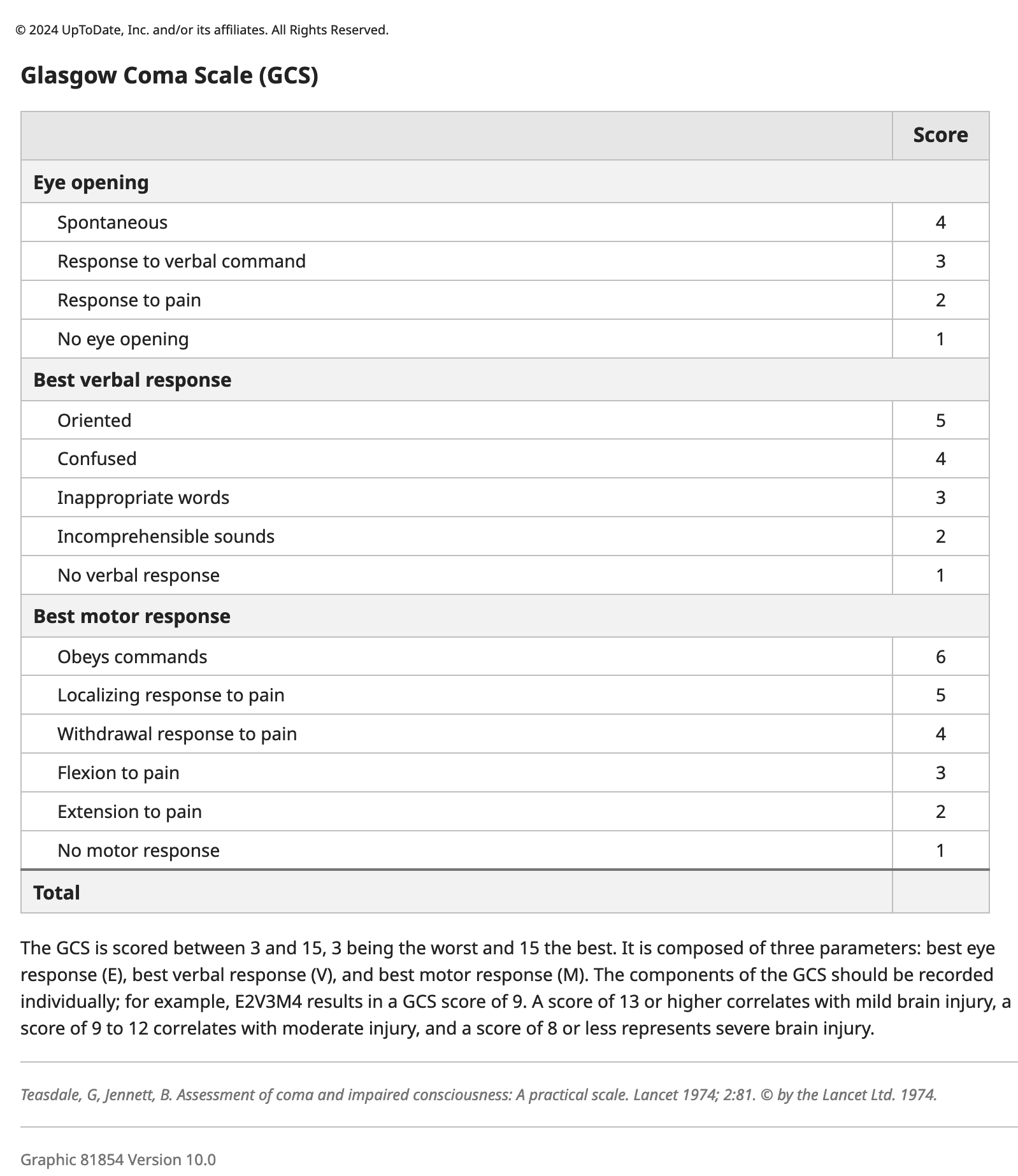
This is most likely mild traumatic brain injury. The definition includes trauma and a Glasgow Coma Scale of 13–15. While patients typically have neurological symptoms—e.g., confusion and headache (symptoms of “concussion”)—focal neurological findings point to a more serious brain injury. While a neuro exam is important, the first step is GCS.
- Patients with a GCS < 15 should be admitted for evaluation and observation for 24 hours.
- Other indications for admission include bleeding risk and significant LOC or neurological findings.
- A non-contrast CT scan to exclude skull fracture or bleeding is the first test if needed.
- MRI is not a first-line test in most instances unless the patient has an obvious skull fracture on clinical examination—then an MRI may be a first-line test to distinguish SDH from EDH.
- Rest for at least 24 hours with “observation” (someone to check on the person) is recommended. Return to school, work, or sports is dependent on function and risk. Return to sports while still symptomatic is not recommended, but prolonged “cognitive rest” is controversial.
- See UpToDate: Sequelae.