- Nitroglycerin.
- Aspirin.
- Furosemide.
- Benazepril.
- Metoprolol.
- Amitriptyline.
- Atorvastatin.
- BP 120/72. P 65 with slight irregularity.
- CV: RRR S1S2 with 1/6 SM at LLSB without radiation.
- Chest: CTA.
- Extremities: No cyanosis or oedema.
LV mildly enlarged at 60 mm. Akinesis of the inferior wall and basal 2/3 of the septum. LV function is mildly reduced. LA is 45 mm (mildly enlarged). RV size and function are normal. Trileaflet AoV without AI. Mild mitral and tricuspid regurgitation present. Frequent PVCs noted.
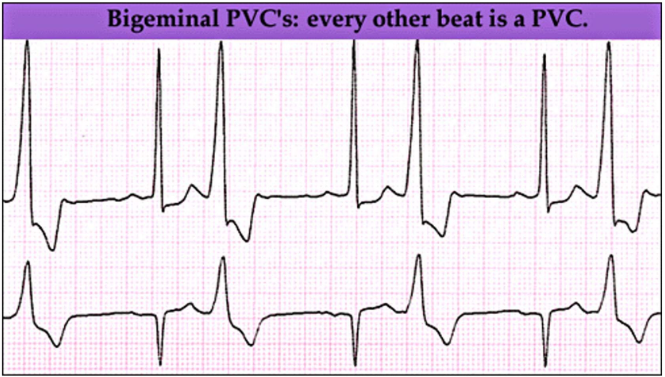
Heart rate avg 79, min 50, max 107. Basic rhythm is sinus with frequent bigeminy (total 7 hours 12 minutes). There were 2443 premature ventricular contractions, more than 200 per hour for 6 hours. There were 25 couplets and no sustained ventricular arrhythmias. The patient experienced dizziness and fatigue while exercising. During this time, the patient had >200 PVCs per hour.