

Patient 1: Clay—Pins and needles
Question
Which of the following chemical exposures is the most likely cause of his symptoms?
Organophosphates:
-
Organophosphate toxicity usually presents clinically in three different stages, the final involving a delayed polyneuropathy. Organophosphate-induced delayed neuropathy (OPIDN) is seen as an axonal polyneuropathy involving distal weakness and sensory loss, which may follow a progressive course. While our patient did demonstrate weakness and distal polyneuropathy, he did not experience the usual preceding symptoms, which include an acute cholinergic syndrome followed by an intermediary paralysis of respiratory muscles.
Niacin:
-
The main niacin (vitamin B3) deficiency syndrome is pellagra, which most notably involves dermatitis, dementia and diarrhea (“the three Ds”). While an isolated niacin deficiency is not known to cause peripheral neuropathy in the same way as a B12 deficiency might, it can be a red flag for other deficiencies. When a patient is deficient in niacin, they are most likely deficient in other nutrients.
Nitrogen-based mixtures:
-
Nitrogen-based mixtures have been used as agricultural fertilizers for nearly as long as humans have been cultivating crops. While prolonged exposure to concentrated formulas can cause irritation to the skin and mucous membranes, as well as fainting and low blood pressure, it is not known for inciting peripheral neuropathy.
CBD (Cannabidiol) Oil:
-
CBD oil (cannabidiol oil) has been touted as an alternative therapy for peripheral neuropathy, and is not widely recognized to cause neuropathy-like symptoms.
Alcohol (correct answer):
-
Cerebellar degeneration and polyneuropathy are two well-known complications of heavy, long-term alcohol use. Cerebellar degeneration and subsequent atrophy are, in non-genetic cases, very specific to either alcohol abuse or long-term use of the drug Dilantin. Loss of Purkinje cells in the cerebellar cortex is thought to be the main reason for tissue atrophy, which is visible on brain MRI. Midline cerebellar structures, including the anterior and superior vermis, tend to be affected the most. Distal leg weakness and ataxia can be two initial presenting features of cerebellar involvement, and the axonal polyneuropathy further contributes to gait instability and sensory changes. The pathogenesis of alcohol-related polyneuropathy is believed to be due to a combination of neurotoxicity complicated by nutritional (thiamine) deficiency, as measured by erythrocyte transketolase activity.
Keywords: Neuropathy, alcohol
References
- Kobayashi S, Okubo R, Ugawa Y. Delayed Polyneuropathy Induced by Organophosphate Poisoning. Intern Med. 2017;56(14):1903–1905. doi: 10.2169/internalmedicine.56.7921. Epub 2017 Jul 15. PMID: 28717090; PMCID: PMC5548687.
- Charness, M.E. Overview of the chronic neurologic complications of alcohol. In:UpToDate. Updated Dec. 6, 2018.
- Hammond N, Wang Y, Dimachkie MM, Barohn RJ. Nutritional neuropathies. Neurol Clin. 2013 May;31(2):477–89. doi: 10.1016/j.ncl.2013.02.002. PMID: 23642720; PMCID: PMC4199287.
- Plant fertilizer poisoning. Mount Sinai. Reviewed Sep. 28, 2019.
- Xu DH, Cullen BD, Tang M, Fang Y. The Effectiveness of Topical Cannabidiol Oil in Symptomatic Relief of Peripheral Neuropathy of the Lower Extremities. Curr Pharm Biotechnol. 2020;21(5):390–402. doi: 10.2174/1389201020666191202111534. PMID: 31793418.
- Mary E. Lynch, Paula Cesar-Rittenberg, Andrea G. Hohmann. A Double-Blind, Placebo-Controlled, Crossover Pilot Trial With Extension Using an Oral Mucosal Cannabinoid Extract for Treatment of Chemotherapy-Induced Neuropathic Pain. Journal of Pain and Symptom Management, Volume 47, Issue 1, 2014. Pages 166–173. ISSN 0885-3924,. https://doi.org/10.1016/j.jpainsymman.2013.02.018.
Patient 2: Carrie—Fingers don't work
Question
Which of the following combination of physical findings is most likely?
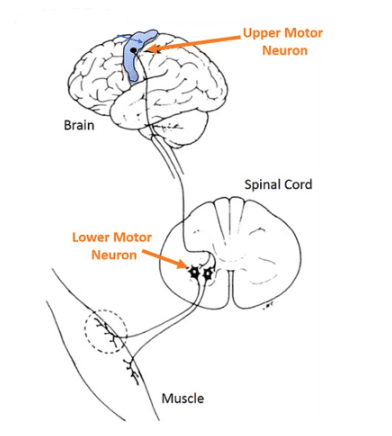 Guillian-Barré is an acute demyelinating disorder that affects the peripheral nerves. This results in symptoms of lower motor neuron lesions. This answer is the only one that contains all LMN findings. There other ones contain UMN or a mix of UMN/LMN findings. Of note, a positive Babinski is found in UMN lesions. Absent DTR reflexes is the hallmark of Guillian-Barré, and you will be asked about this fact a lot on the wards!
Guillian-Barré is an acute demyelinating disorder that affects the peripheral nerves. This results in symptoms of lower motor neuron lesions. This answer is the only one that contains all LMN findings. There other ones contain UMN or a mix of UMN/LMN findings. Of note, a positive Babinski is found in UMN lesions. Absent DTR reflexes is the hallmark of Guillian-Barré, and you will be asked about this fact a lot on the wards!
| Feature | Upper Motor Neuron Lesion (UMN) | Lower Motor Neuron Lesion (LMN) |
|---|---|---|
|
Site of lesion |
|
|
|
Muscle weakness |
|
|
|
Muscle tone |
|
|
|
Fasiculations |
|
|
|
Tendon reflexes |
|
|
|
Abdominal reflexes |
|
|
|
Sensory loss |
|
|
|
Electromyography (EMG) |
|
|
Note
Rationale for incorrect answer choices
UMN: Positive Babinski reflex, hyperreflexia, muscle stiffness.
LMN: Fasciculations, hyporeflexia/areflexia and muscle atrophy.
References
- Brealey, David, and Nicholas Hirsch. Diagnosis, Assessment, and Management of Guillain-Barré Syndrome. Oxford Medicine Online. Apr. 2016. doi:10.1093/med/9780199600830.003.0246.
- Emos MC, Agarwal S. Neuroanatomy, Upper Motor Neuron Lesion. [Updated 2021 Aug 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan—.
- Javed K, Daly DT. Neuroanatomy, Lower Motor Neuron Lesion. [Updated 2021 Aug 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan—.
Image credits
Unless otherwise noted, images are from Adobe Stock.