

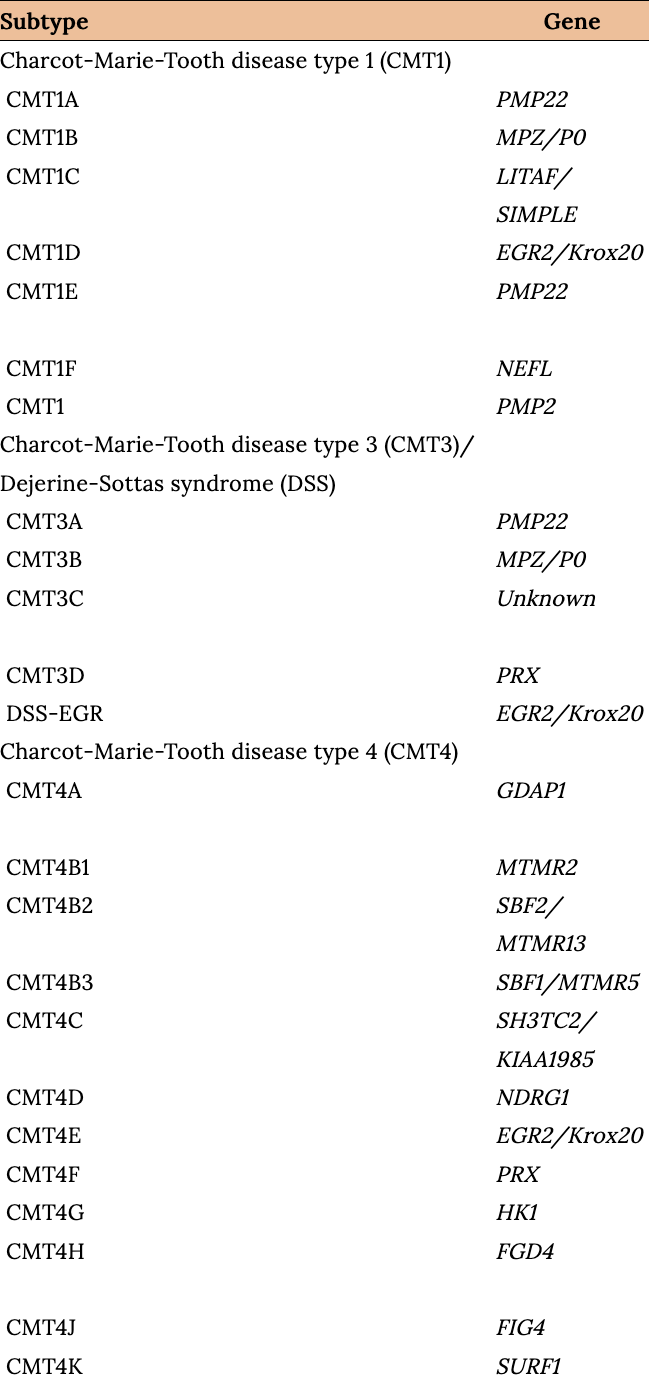
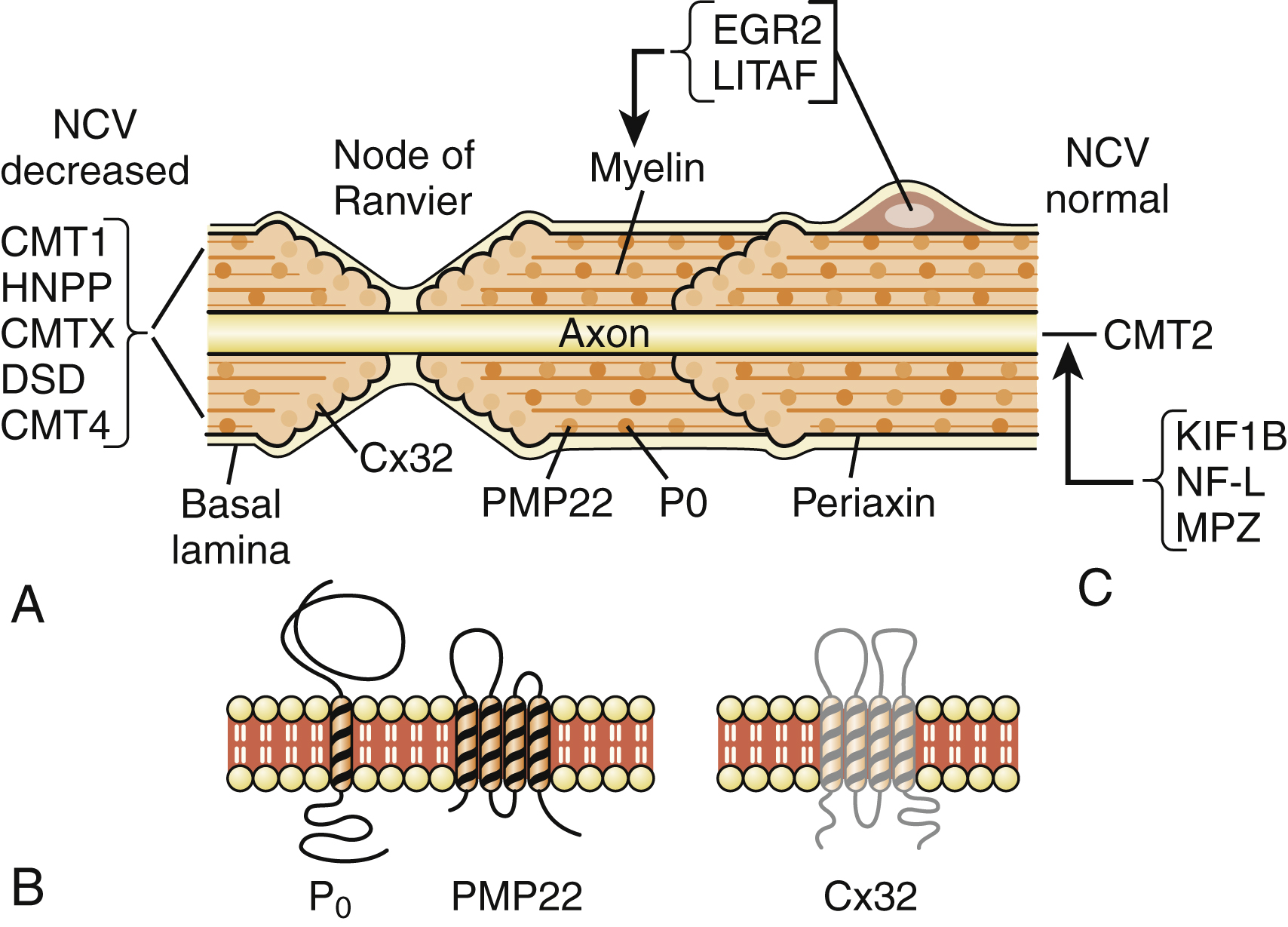
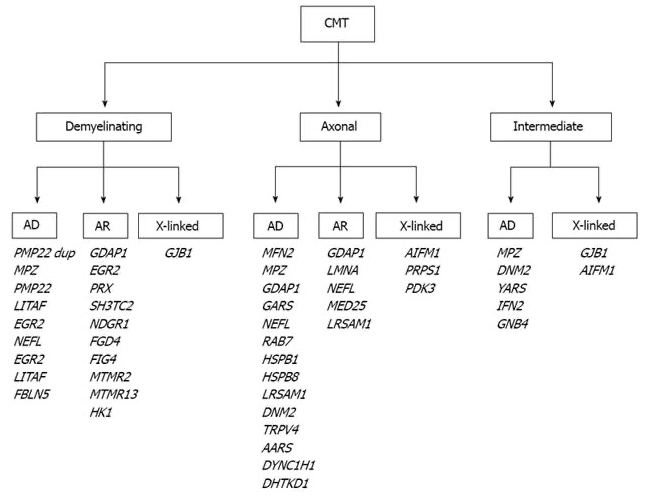
- There are many ways to classify. The majority of CMT neuropathies are demyelinating, although up to one-third are primary axonal disorders.4
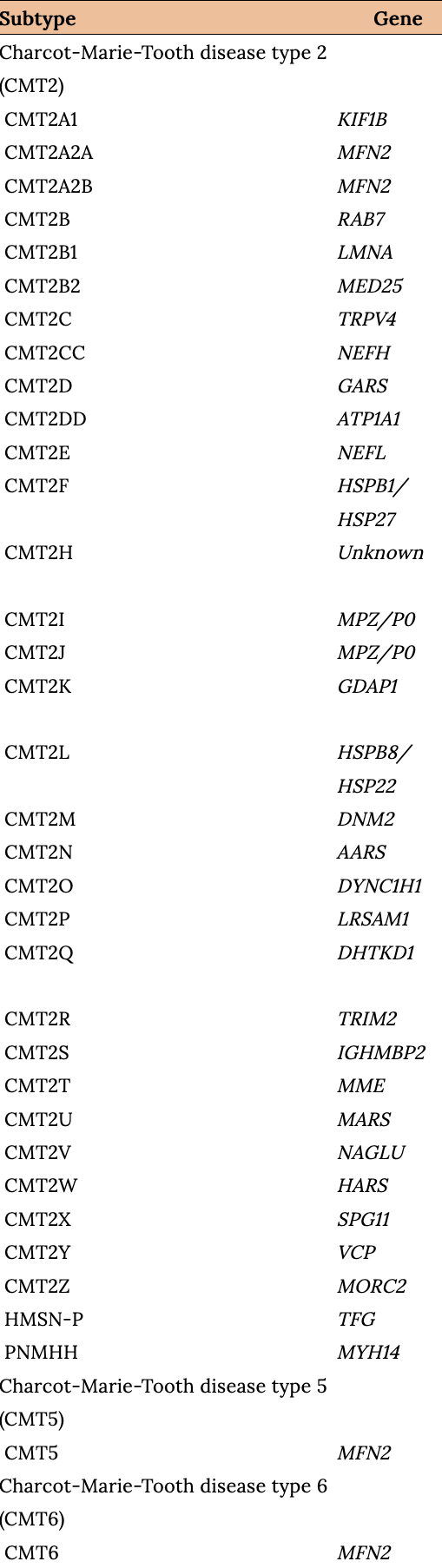
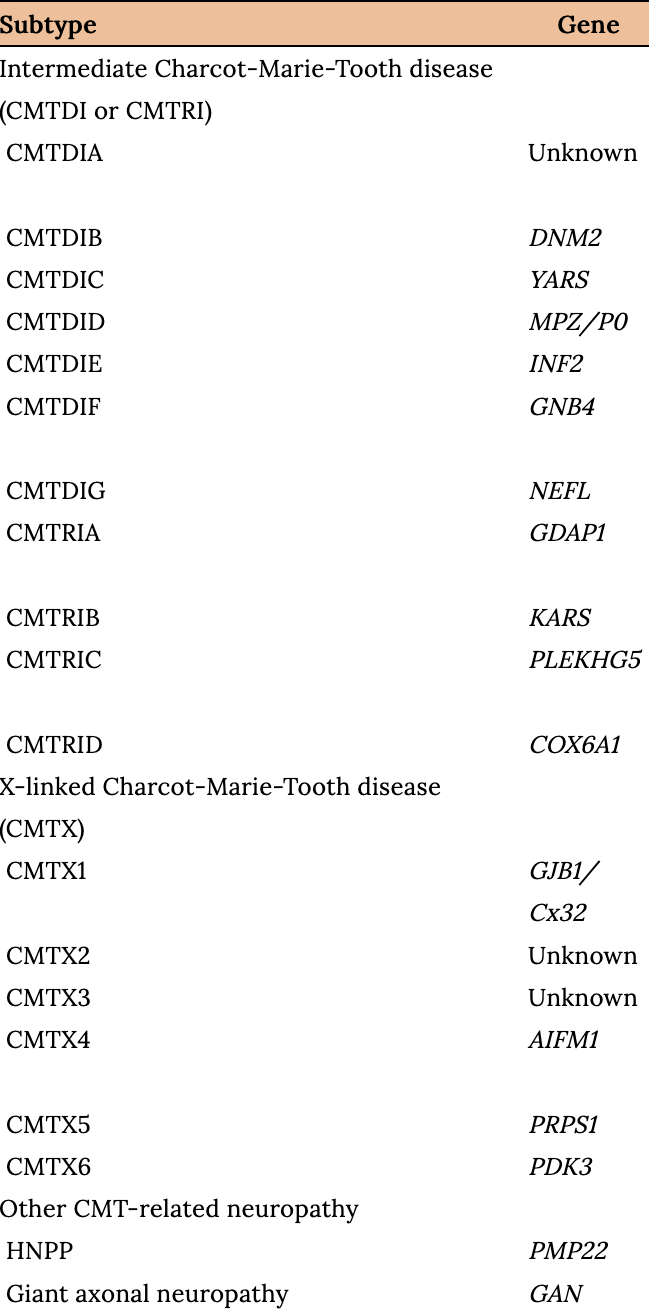
- The three most common types of HMSN are CMT1, CMT2, and CMTX.
- HMSN/CMT Type 1: Demyelinating. Autosomal Dominate
- HSMN/CMT Type 2: Axonal. Autosomal Dominate
- HSMN/CMT Type X: Intermediate motor conduction. X-linked
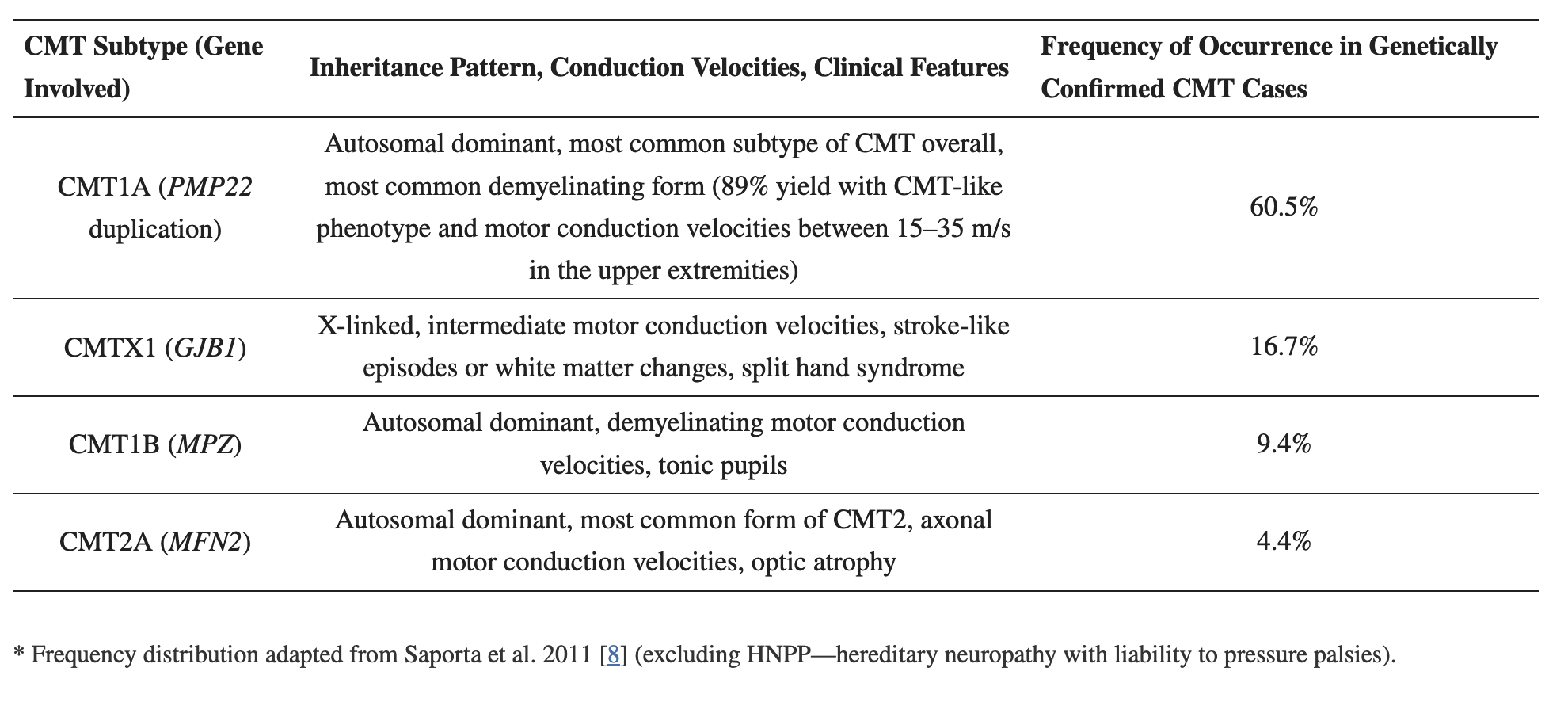
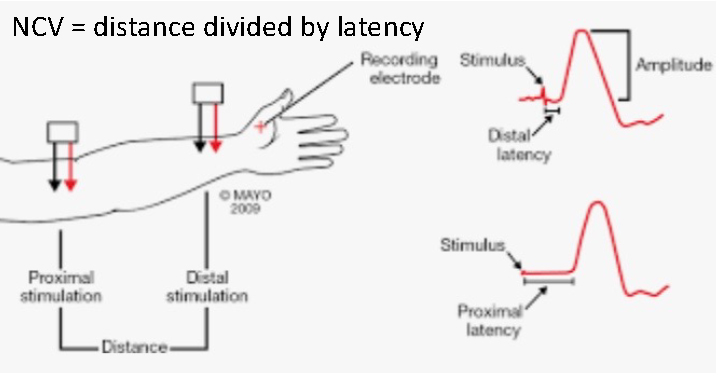
- Loss of myelin (CMT1) slows nerve conduction. Motor conduction velocity below 35 m/sec in the forearm segment of the median or ulnar nerves is a proposed cutoff value to distinguish CMT1 from CMT2 and CMTX.4

Bradley WG. Disorders of Peripheral Nerves, Fig. 106.08.


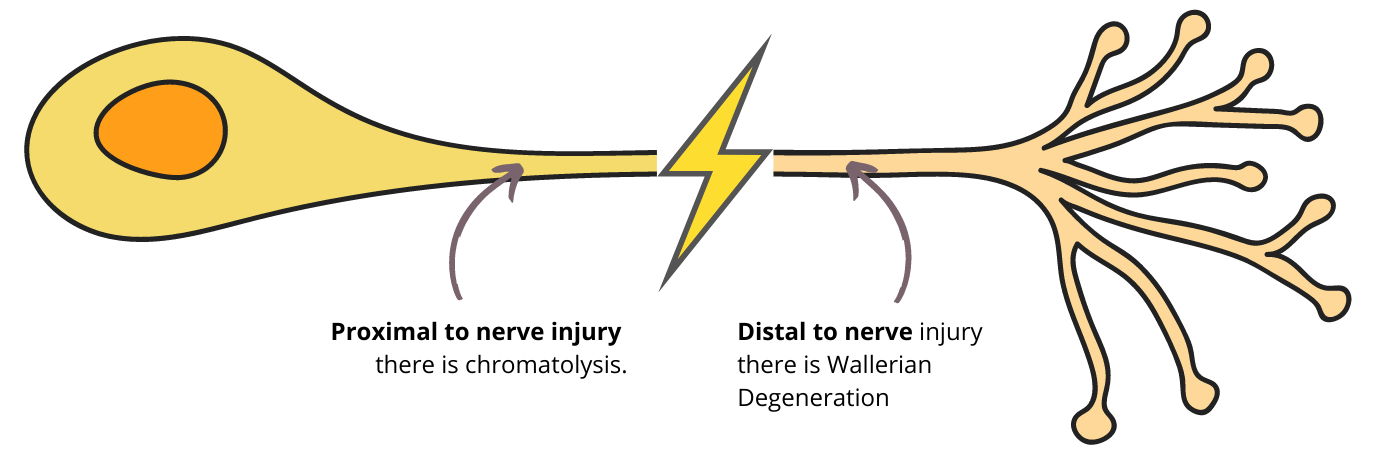
- Wallerian axonal degeneration with intact myelin sheath.
- Motor NCVs are normal or near normal, and nerve biopsy reveals axonal loss without prominent demyelination.4
- Symptoms commonly present in the second decade, or even later.4
- 20% are asymptomatic.
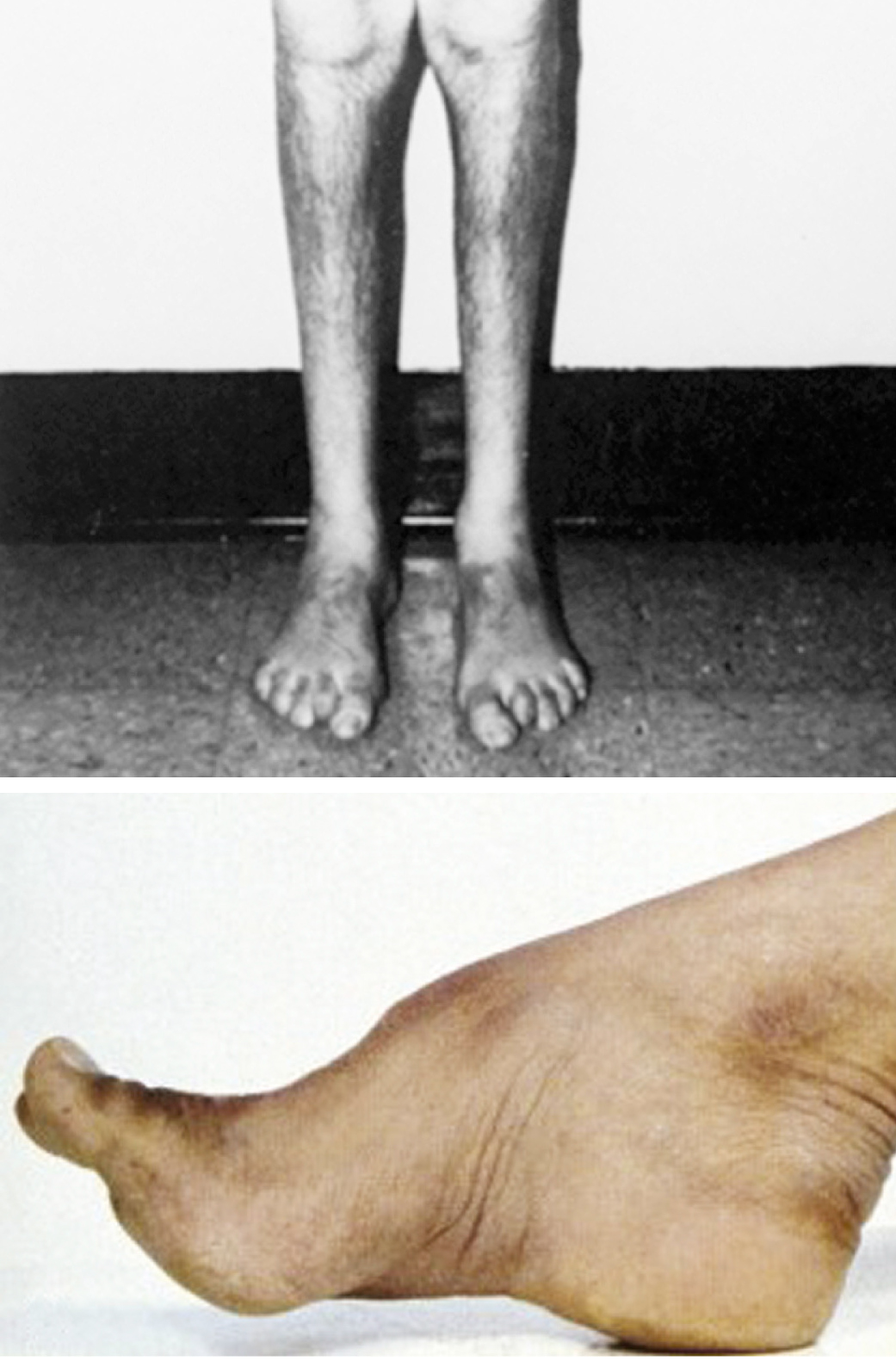
- Foot and spinal deformities are less common.
- The presentation is more variable (optic nerve atrophy, foot ulcers, vocal cord atrophy, intercostal muscle weakness).

- Nerve conduction studies:
- Nerve conduction velocity:4
- CMT1: <38 m/s.
- CMT2: >38 m/s.
- INT CMT: 24–45 m/s.
- EMG:
- Uniform and symmetric abnormalities.
- Nerve conduction velocity:4
- Molecular and genetic testing.
- CSF analysis, CBC, and CMP normal.
Reilly MM. Classification and diagnosis of the inherited neuropathies. See at Diagnosis of Charcot Marie Tooth Disease.
- Symptomatic treatment.4–6
- Physical therapy.
- Proper footwear and insoles and orthotics.
- Avoid insults to PNS, like neurotoxic drugs.4,6
- Risks with pregnancy (birth complications/↑severity of disease).4,6
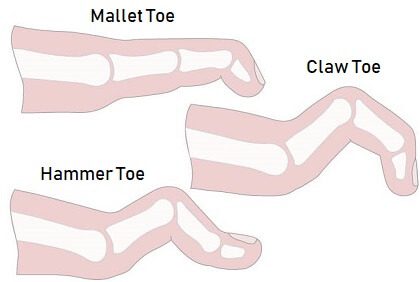
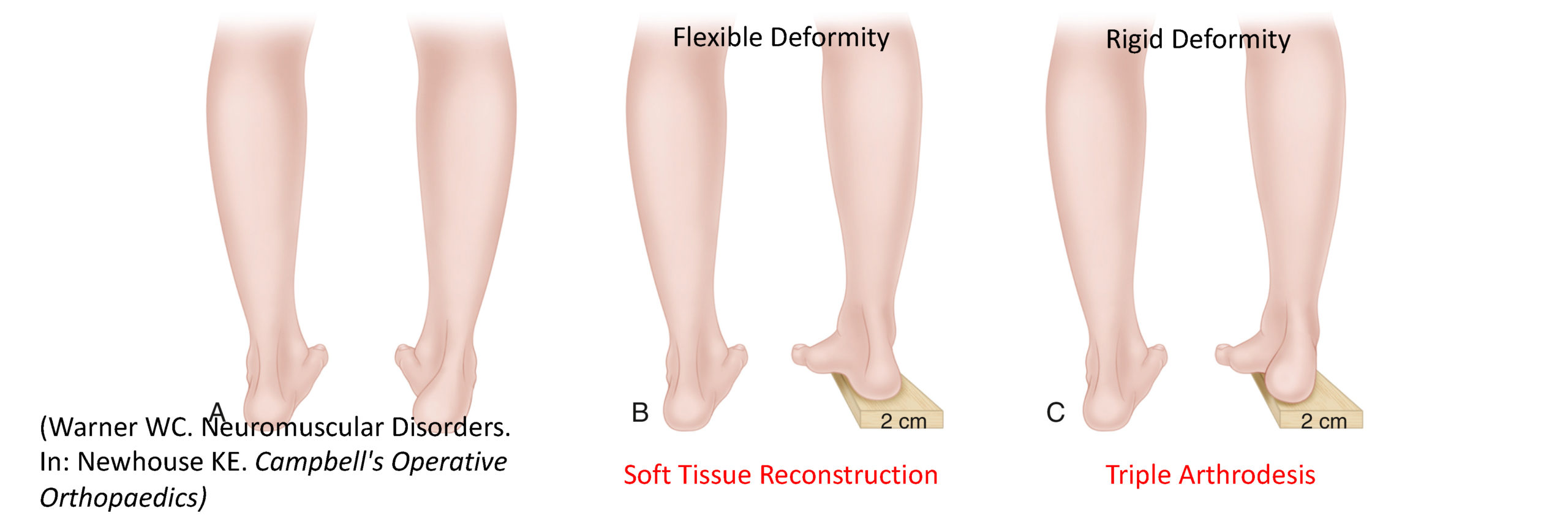
- Orthopaedic consultation for cavovarus, claw foot, hammer toes, and scoliosis.
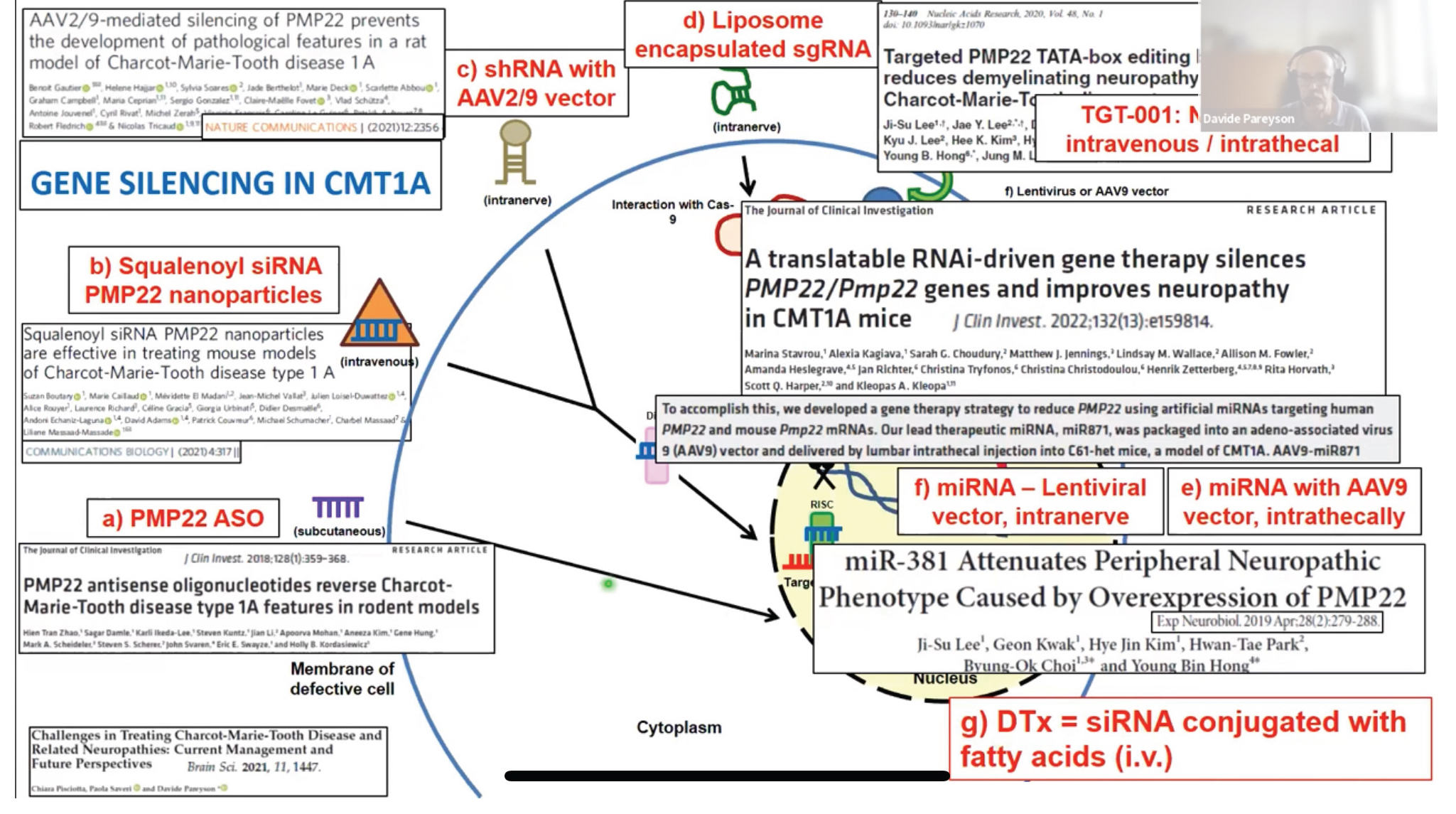
- No effective pharmacological treatment.
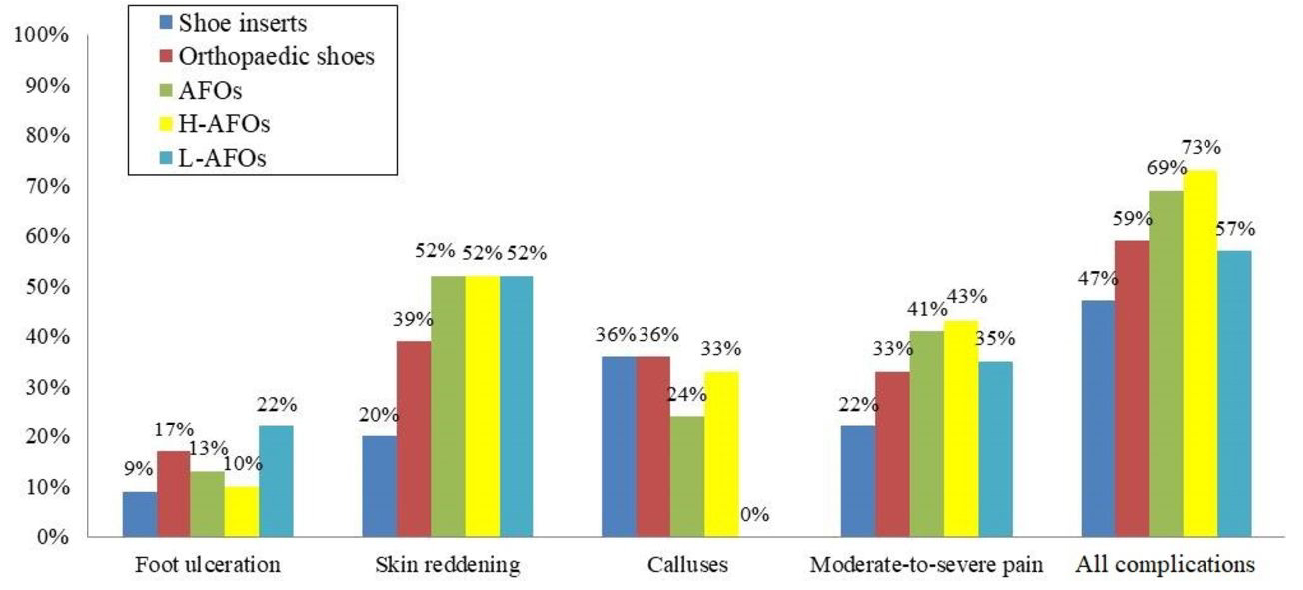
Orthotics and CMT
Perceived improvement in gait, stability/balance, and reduction in falls.7
-
- 21% never used, 31% abandonment, 69% reported complications.7
The utility of physical therapy in CMT
- After intensive rehabilitation treatment, all outcomes significantly improved.8
- This improvement was lost at the 1-year mark.8
Conclusion
Intensive rehabilitation program improves short-term symptoms and functional outcomes in a cohort of inpatients affected by mild to moderate CMT.
Source: Ferraro F, Calafiore D, Curci C, Fortunato F, Carantini I, Genovese F, Lucchini G, Merlo A, Ammendolia A, de Sire A. Effects of intensive rehabilitation on functioning in patients with mild and moderate Charcot-Marie-Tooth disease: a real-practice retrospective study. Neurol Sci. 2024 Jan;45(1):289-297. doi: 10.1007/s10072-023-06998-0. Epub 2023 Aug 8. PMID: 37552411; PMCID: PMC10761523.
Peroneus brevis overpowering peroneus longus.
- Fredrich ataxia.
- Alcoholic polyneuropathy.
- Chronic inflammatory demyelinating polyneuropathy.
- Refsum disease.
- Vitamin B12 deficiency.
- Guillain-Barré.
- Thyroid disease.
- Diabetes Mellitus.
- Amyloid neuropathies.
- Leprosy.
- HIV-associated distal symmetric polyneuropathy.
- Toxic polyneuropathy:
- Chronic: Cisplatin, doxorubicin
- Acute: Diphtheria toxin, suramin, amiodarone.

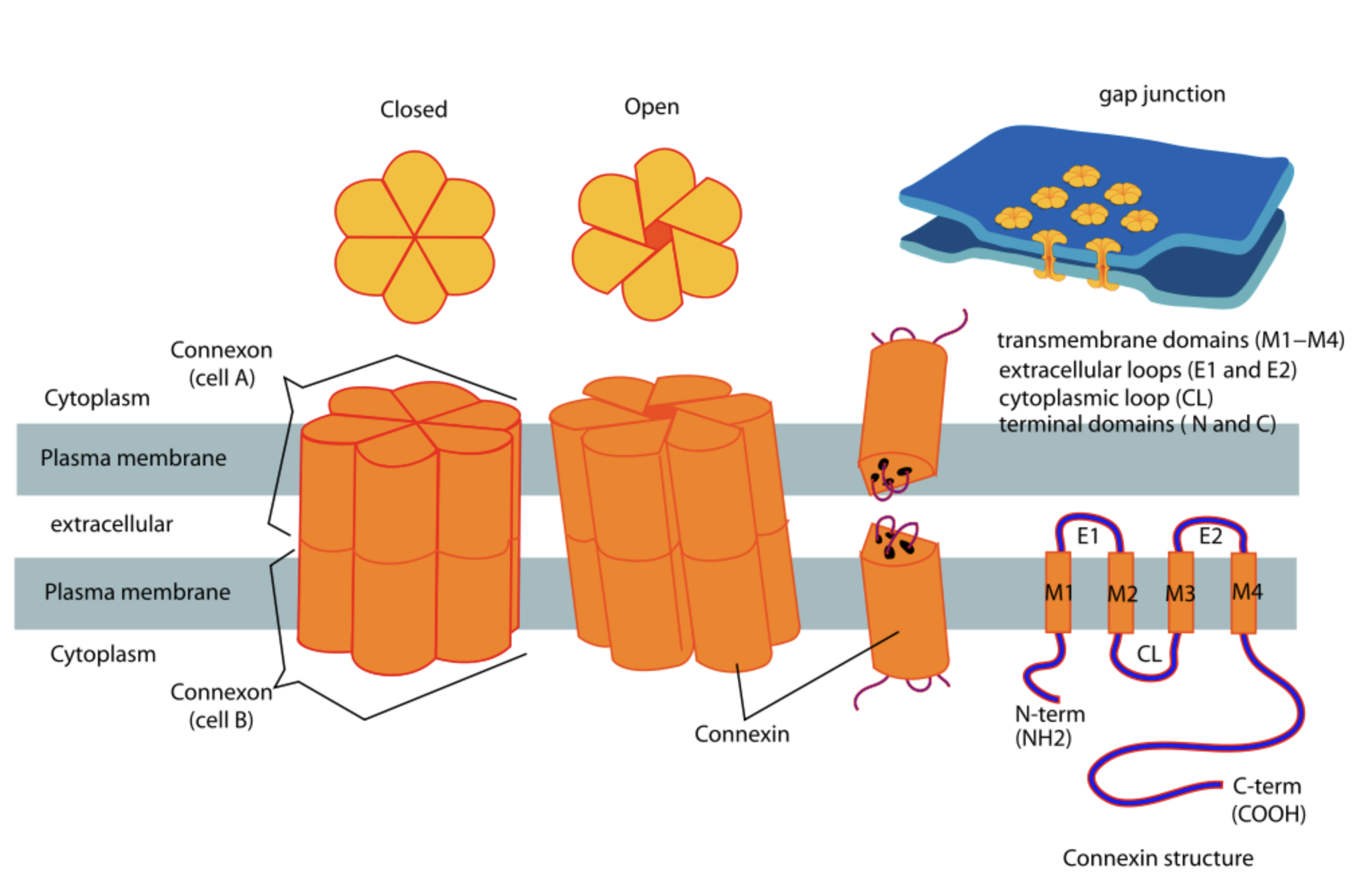
"to support the development of new treatments for CMT, to improve the quality of life for people with CMT, and, ultimately, to find a cure."