MD, MSc, CMedEd, MACP, FRACP, FRCP-London · Senior Associate Dean, Collaboration for InterProfessional Health Education Research & Scholarship (CIPHERS)
Table of Contents
Case study 2: Joe—Couldn't raise left hand and arm
Tap the image to view the case.
A 72-year-old male is brought into the ER by ambulance after he could not pick up his mug of coffee using his left hand. His wife said he tried to pick up the mug, but couldn’t raise his hand and arm off the table. She also noticed that the left side of his face looked “droopy,” and thought he might be having a stroke. His past medical history is notable for mild hypercholesterolemia, hypertension, and stable angina.
Question
Initial imaging is likely to reveal a finding in which location of the patient’s brain?
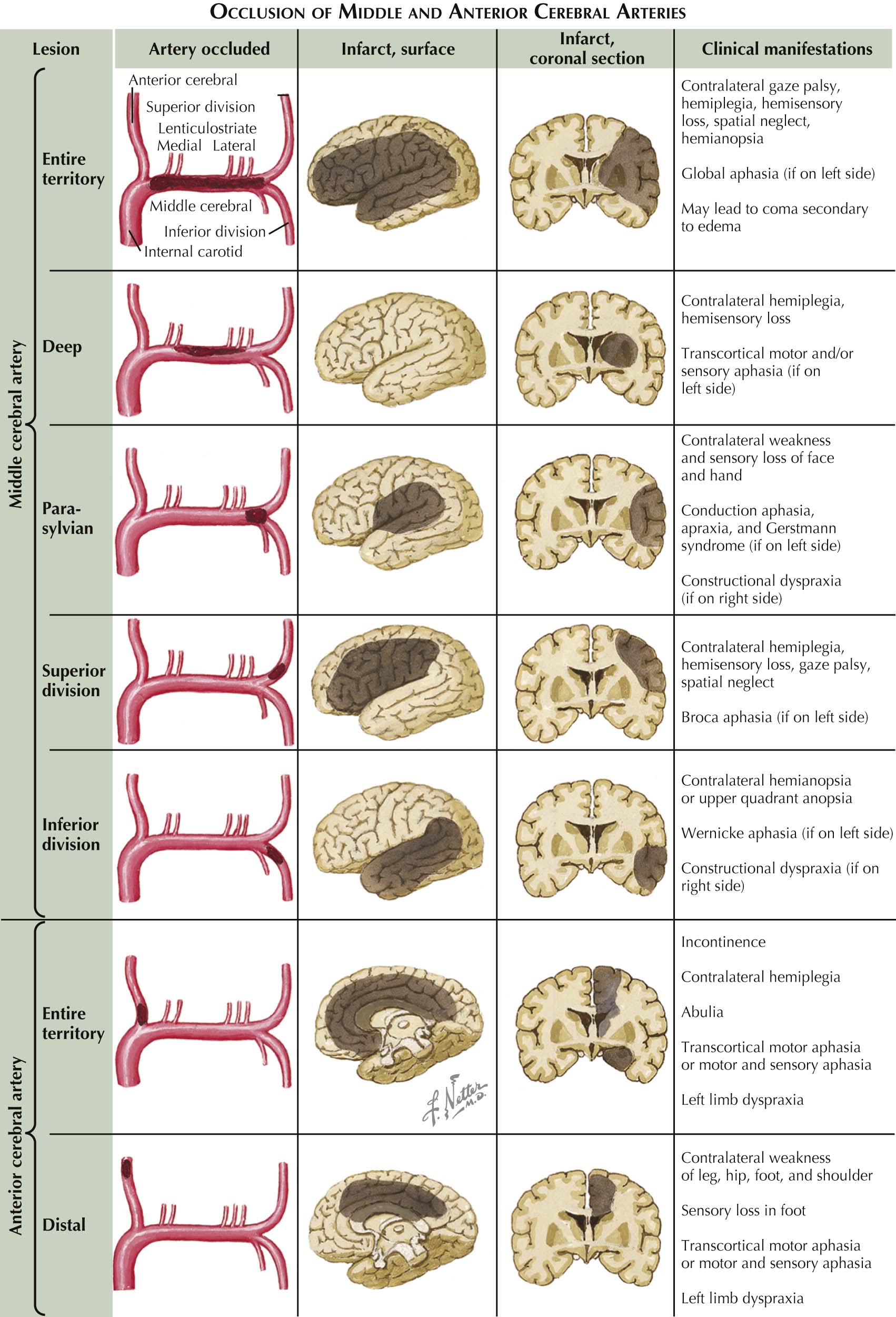
The patient is demonstrating left-sided upper extremity weakness as well as left-sided facial droop. This is consistent with a lesion on the contralateral side of the brain (R) and in the MCA territory.
Localize a stroke
Localizing a stroke involves careful physical examination combined with imaging findings. It is a much bigger topic than we can cover in this single module.
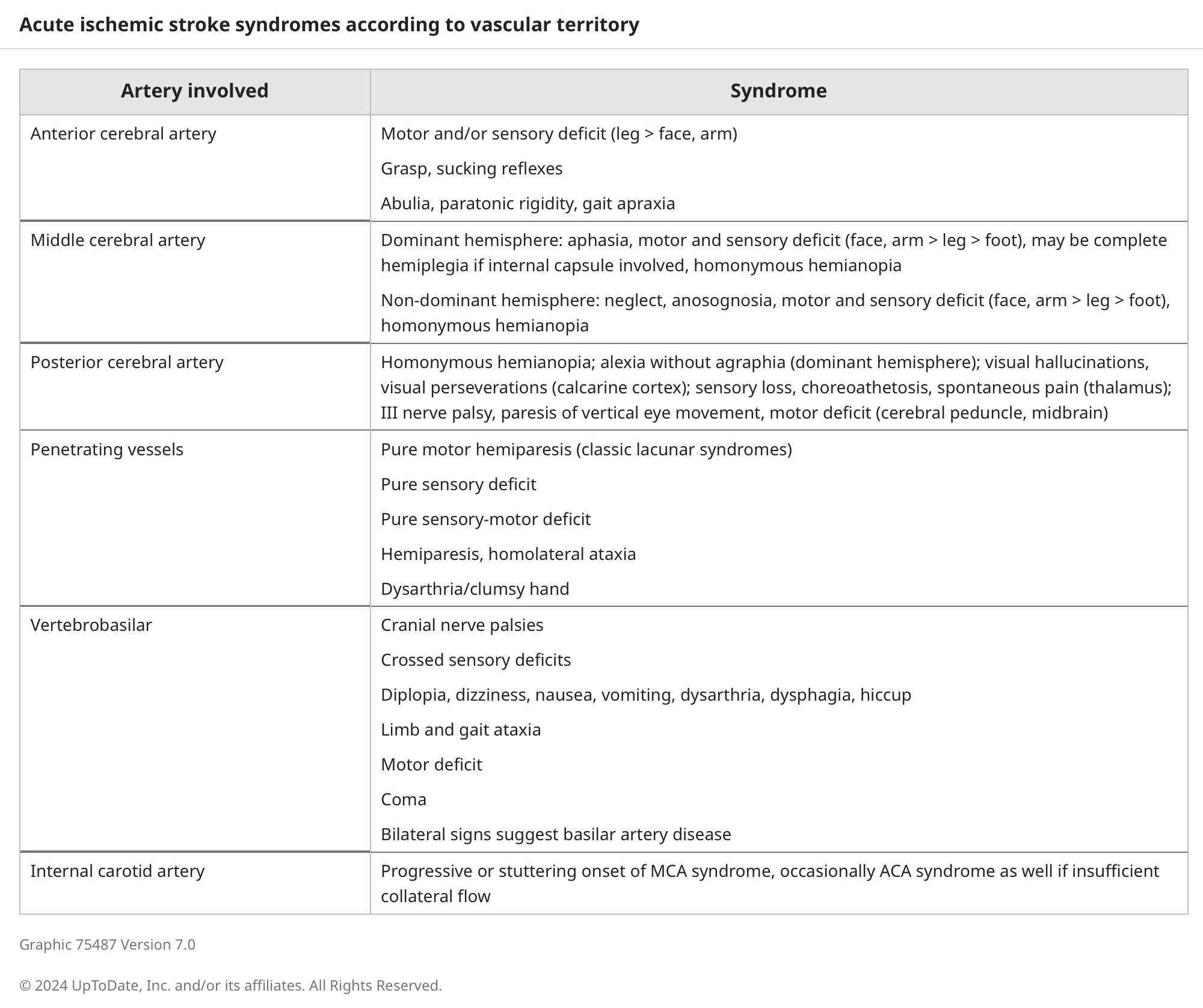
Overview of common stroke findings, by location:
Majority of strokes are supratentorial s/sx of “FAST” (facial droop, arm weakness, speech disturbance, time).