

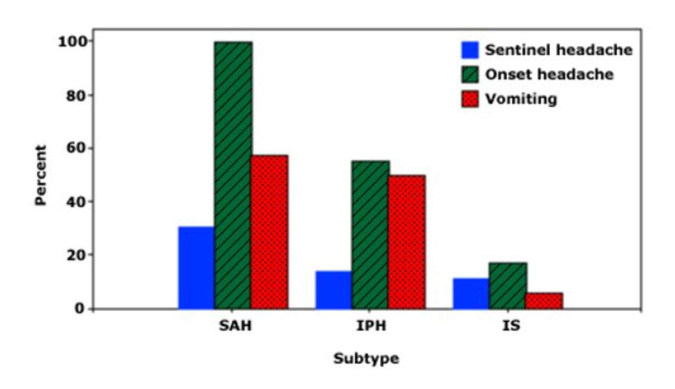
- Onset: SAH is usually sudden, ICH worsens over minutes to hours; ask for sx of SAH “sentinal bleeds”
- Patient may complain of the “worst headache of [their] life,” especially in subarachnoid hemorrhage.
- Specific neurologic deficits depend of location of hemorrhage (see “localizing stroke” slide).
- Other complaints may include: Nuchal rigidity, vision changes, nausea/vomiting
Demographics: Seen most commonly in patients with HTN.
Primary causes (80%–85%)
- HTN.
- Cerebral amyloid angiopathy.
Secondary causes (15%–20%)
- Hemorrhagic conversion of ischemic stroke.
- Stimulant drugs.
- Vascular malformation: Aneurysm, AVM, venous angioma, cavernoma, dural AV fistula.
- Coagulopathy: Hereditary, acquired, iatrogenic (anticoagulants, antiplatelets).
- Neoplasm.
- Trauma.
CT
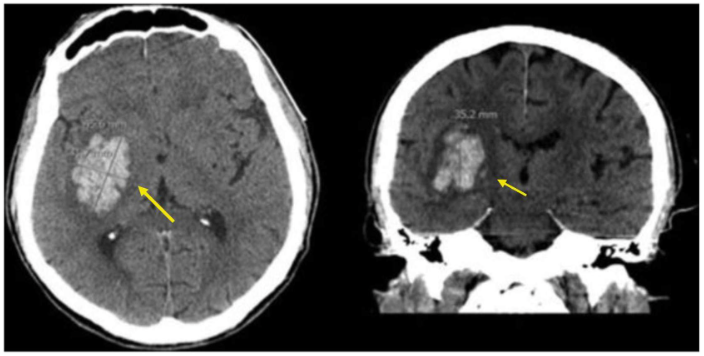
Non-Contrast CT Findings (Examples)
- Often used for hyperacute stroke imaging can we/should we give tPA?
- Benefits: Allows for fairly accurate measurement of hematoma volume, and can be done serially to monitor evolution.
- Findings
- First 72 hours: Bleed shows up as hyperintensity, with surrounding hypodense edematous area.
- 3–20 days after initial stroke: Lesion becomes less intense and may appear to shrink; may develop irregular, abscess-like ring border.
- Contrast CT-angio (“CTa”) can help determine risk of hematoma enlargement “spot sign” = contrast extravasation into hematoma.
MRI Benefits vs. CT
- Higher degree of sensitivity for detecting small strokes.
- Deoxyhemoglobin is identifiable as a blood degradation product in early strokes, due to its paramagnetic properties.
- Good for detecting causes of secondary intracranial hemorrhage, (e.g., vascular malformations).
Do not give tPA!
The goal is to stop the bleed, not make it worse.
- Patients often require treatment in the ICU or a dedicated stroke unit.
-
Bleeding management: All anticoagulant and antiplatelet drugs should be discontinued, at least temporarily, upon presentation.
- HTN management:
- For systolic BP 150–220 mmHg, lower to ~140 mmHg.
- For systolic BP > 220 mmHg, aggressively lower to ~140–160 mmHg.
- Other considerations:
- Management of intracranial pressure/mass effect (mannitol commonly used).
- Intubation/mechanical ventilation.
- Seizure prophylaxis (levetiracetam [Keppra] most commonly used).
- +/- surgical evacuation of hematoma.
Most common cause of stroke (87%).
Lack of perfusion to a certain area of the brain due to blockage or disruption of arterial blood flow.
- Artero-embolic (large-artery disease): Atherosclerotic disease.
- Lacunar (small vessel disease): Microatheroma, microembolism.
- Cardioembolic: Afib, valvular disease.
- Other: Arterial dissection, vasospasm, vasculitis, hypercoagulable states.
- Idiopathic.
-
Specific neurologic deficits depend on area of the brain affected by stroke (see “stroke localization”).
-
Onset of ischemic stroke can be “stuttering” while embolic stroke is usually sudden, similar to hemorrhagic events.
-
Recognition of stroke may be delayed if person lives alone or deficits are subtle important: can affect management (+/- tPA).
-
Severe headache less likely with ischemic events—you may recall from the previous section that severe headache is much less likely with ischemic strokes.
-
Current recommendation = ok to give tPA if:
- No evidence of hemorrhage on initial imaging (usually non-contrast CT).
- Stroke is believed to have occurred within 4.5 hours of “last known normal”
- Stroke is considered “disabling” to individual (perceived benefit of intervention > risk).
Endovascular intervention
- Thrombectomy decreases morbidity and mortality in major acute ischemic strokes.
- Goal reperfusion time: 90 mins.
Blood pressure
- Goal BP < 180/105 (> 120 systolic); prefer IV labetolol, nicardipine, or clevlidipine.
Oxygenation
- Goal is > 94% SaO2.
- Patients may require intubation due to compromise of respiratory drive (esp if brainstem involvement).
Aspirin, Statin therapy and DVT prophylaxis
- Initiate as soon as safe.
First-line imaging in acute stroke.
Advantages
- Quick to perform can determine if patient is candidate for tPA.
- Less expensive than MRI.
Disadvantage
- Small infarcts may not be discernible on CT; MRI has better sensitivity and is often obtained after CT.
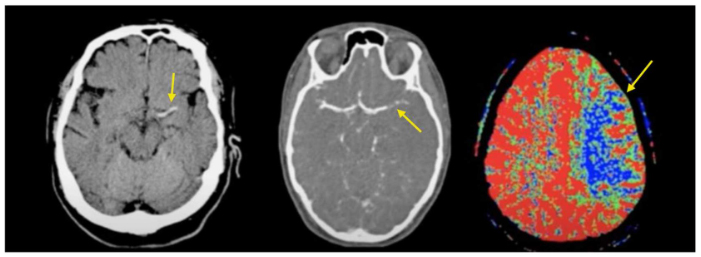
CT Stroke Series (left to right): Non-contrast CT demonstrating acute thrombus; CT angio demonstrating occlusion of L MCA; decreased perfusion.
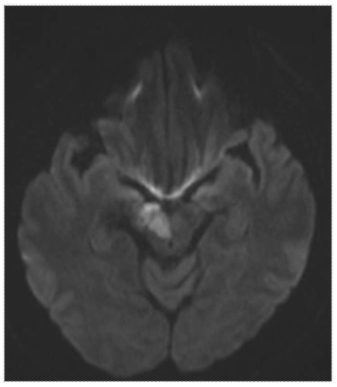
Acute midbrain infarction on DWI
Hyperacute
- Hyperdense segment of occluded vessel may be seen; usually MCA.
- Loss of gray-white matter differentiation in affected area.
- Cortical hypodensity with parenchymal swelling and gyral effacement.
Acute
- Continued parenchymal swelling and gyral effacement mass effect.
Subacute
- Edema begins to subside.
- “CT fogging phenomenon” = cortical petechial hemorrhages increase attenuation of affected cortical areas, which can lead to affected area being mistaken as normal.
Chronic
- Edema diminishes even further; begin to see gliosis as hypodensity on CT.
- Involve brief focal neurologic or speech deficit, depending on affected area.
- Usually last < 5 mins, but can be up to 1 hour in duration.
- R/O stroke: Most hospitals begin workup with appropriate stroke protocol.
- Further workup (if no stroke demonstrated):
- Sleep apnea workup.
- Cardiology workup: r/o PFO (Patent Foramen Ovale).
- Including echo with bubble study.
- Carotid imaging: If > 70% stenosis, significant risk of recurrent event.
- A1C.
- LDL.
Must address any underlying etiology.
- Blood pressure management.
- High-dose statin.
- Antiplatelet therapy.
- Blood glucose control.
- Dietary changes:
- Reduction in carbohydrate (sugar), fat.
- Exercise.
Recommendation summary
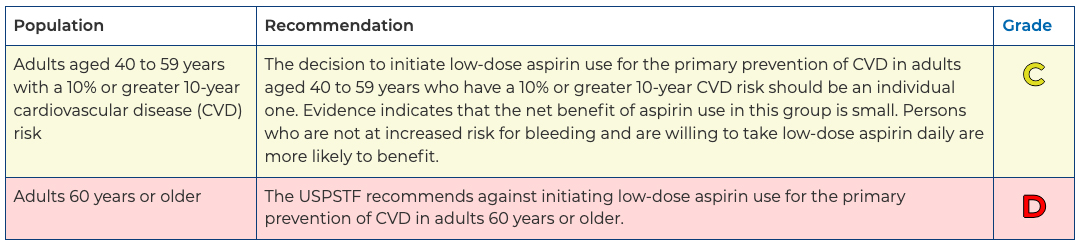
Aspirin Use to Prevent Cardiovascular Disease: Preventive Medication. Final Recommendation Statement. United States Preventive Services Taskforce. April 26, 2022.