

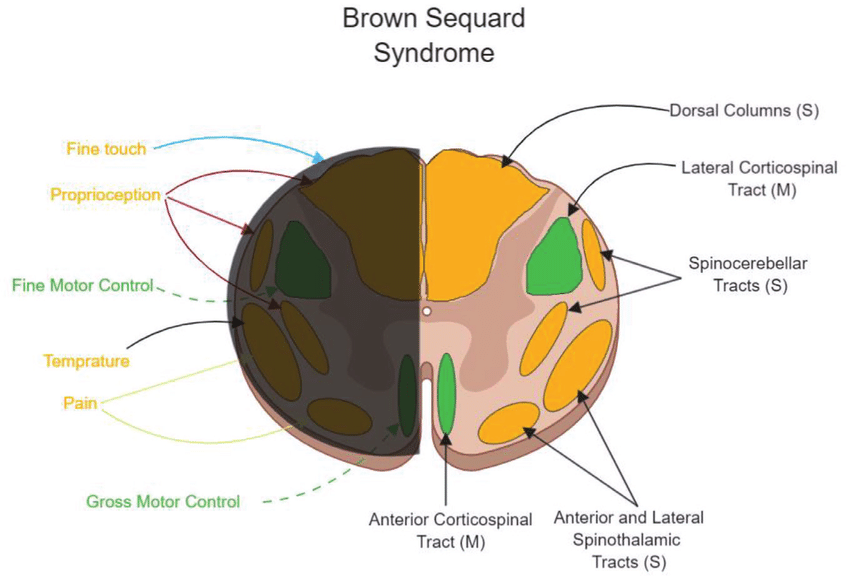
Brown-Séquard Syndrome
- Hemisection of the spinal cord.
- Ipsilateral.
- Weakness.
- UMN signs.
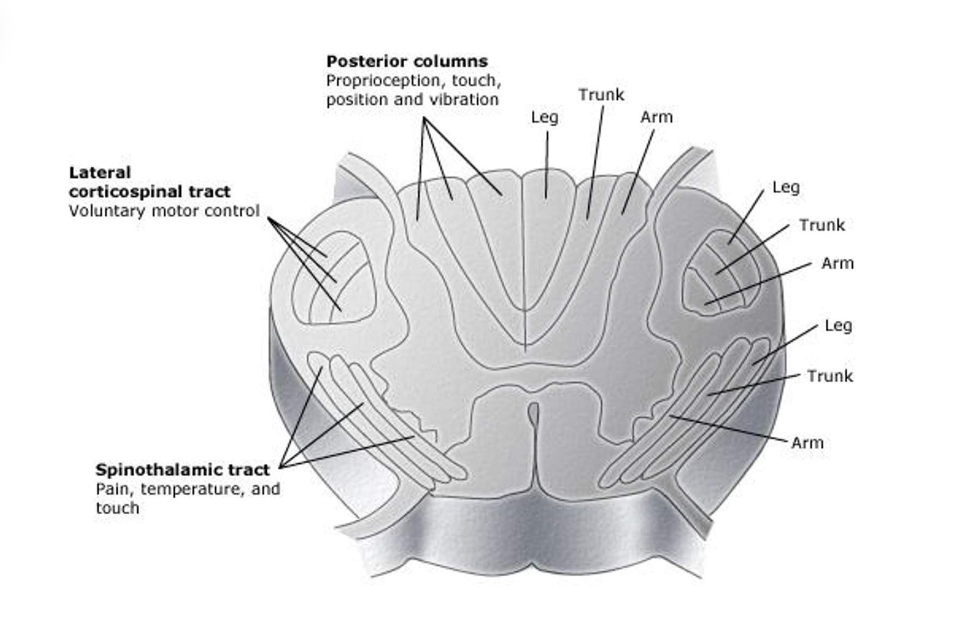
- Loss of position sense.
- Contralateral loss of pain and temperature.
- Light touch sensation usually intact.
The most likely diagnosis is syringomyelia. You should also consider MS in this man. Hemorrhage or tumor affecting the central spiral cord should also be considered.
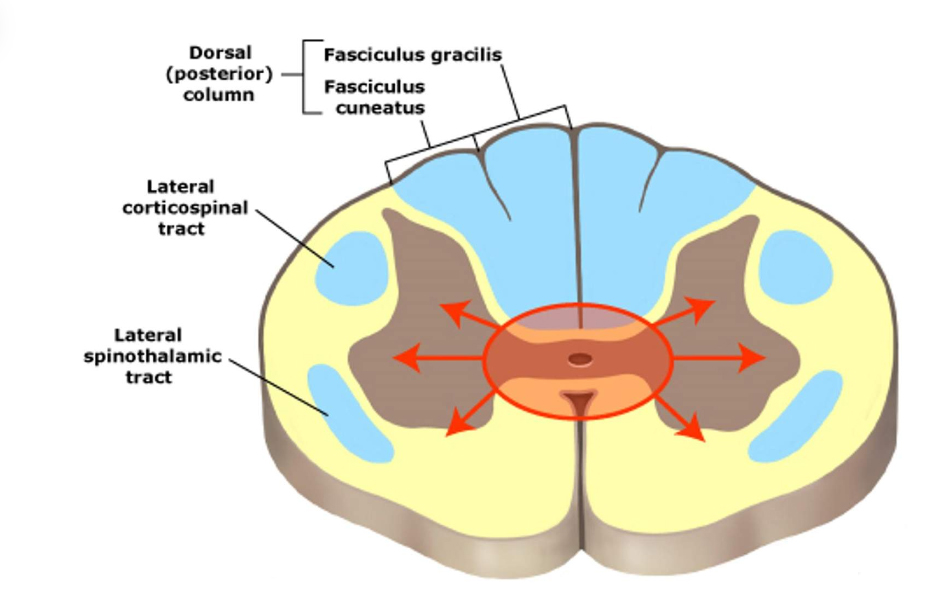
Syringomyelia
 UpToDate, 2008.
UpToDate, 2008.
Central cord lesion caused by CSF collection.
Usual onset in 3rd–4th decade; men > women; slow progression.
Loss of pain/temperature via disruption of the decussate spinothalamic fibers (dissociated sensory loss).
Extension to posterior columns loss of position and vibratory sensation in the feet.
Extension to anterior horns (motor neurons) hand amyotrophy with claw hands and muscle wasting of hands arms.