

Case study 1: Isla—My feet are numb
- History
- Differential diagnosis
- Nine months ago, she had some painless left foot numbness, diagnosed as lumbar disc prolapse, that resolved with chiropractic treatment over 3 weeks.
- Three months ago, she received Hepatitis B vaccine in preparation for her round-the-world trip.
- Family history is negative for neurological problems.
- Rheumatologic: PAN, SLE, Sjogren’s, etc.
- Infectious or post-vaccination (Myelitis, HIV, Lyme, Neurosyphilis, Guillain-Barré).
- Granulomatous—Sarcoidosis.
- Leukodystrophy (inherited especially).
- B12 deficiency.
- Tumor and Paraneoplastic.
- Vascular lesion.
- Syringomyelia.
- Cauda equina syndrome.
- Other metabolic: Diabetes or ETOH.
Features of MS
- Epidemiology/Causality
- Pathophysiology
- Clinical Presentation
- Geographical: Highest 60/100,000 (Oz, NZ, NA, Eur).
- Autoimmune? Viral? Smoking? Birth month (may be linked to maternal vitamin D levels)?
- Likely link with vitamin D deficiency (onset in spring).
- Possible link with hep B vaccine (prob not).
- Multifocal demyelination.
- Loss of oligodendrocytes.
- Astroglial scarring.
- Preservation of axons.
- Relapsing remitting.
- Progressive (15% of patients).
- Onset age: 15–50.
- Sensory loss in limbs (33%).
- Optic neuritis (~15%).
- Internuclear opthalmoplegia.
- Fatigue: “Exhaustion.”
- Llermitte’s sign.
- Uhthoff’s phenomenon.
This patient's physical examination
- Right eye adducts slowly with 5 beats of slow horizontal nystagmus on the left eye as right eye adducts.
- Tone and power normal.
- Reflexes brisk with right extensor plantar reflex.
- Light touch/vibration reduced with T8 level.
- Decreased proprioception at great toes, ankle normal.
- Heel toe gait unsteady.
- Romberg positive.
Question
The patient has cranial nerve findings and findings in at least two places in the central nervous system (T8 spinal cord and right extensor plantar reflex). Note that by history, the patient also has “two lesions separated in time.”
Diagnosing MS: McDonald criteria 2017
Dissemination in space and time
Clinical presentation
| What evidence for MS does the patient already have? | What additional data is needed for an MS diagnosis? |
|---|---|
|
Two or more relapses AND EITHER objective clinical evidence of two or more lesions OR objective clinical evidence of one lesion together with reasonable historical evidence of a previous relapse |
None |
|
Two or more relapses; objective clinical evidence of one lesion (shows DIT) |
Dissemination in space show by: One or more MRI detected lesions typical of MS OR A further relapse showing damage to another part of the CNS |
|
One relapse; objective clinical evidence of two or more lesions (shows DIS) |
Dissemination in time shown by: Oligoclonal bands OR MRI evidence of a new lesion since a previous scan OR A further relapse |
|
One attack/relapse; objective clinical evidence of one lesion (known as “clinically isolated syndrome”) |
Dissemination in space show by: One or more MRI detected lesions typical of MS OR A further relapse showing activity in another part of the CNS Dissemination in time shown by: Oligoclonal bands OR MRI showing new lesions since a prevous scan OR A further relapse |
|
Insidious neurological progression suggestive of multiple sclerosis (typical for primary progressive MS) |
Continued progression for one year (from previous symptoms or by ongoing observation) plus any two of:
|
Investigations
Cervical MRI shows an intrinsic cord lesion C5–C7.
- Axial scan shows dorsal column involvement.
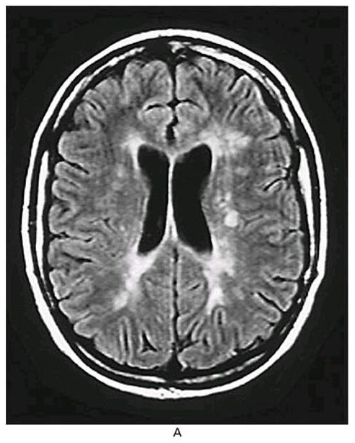
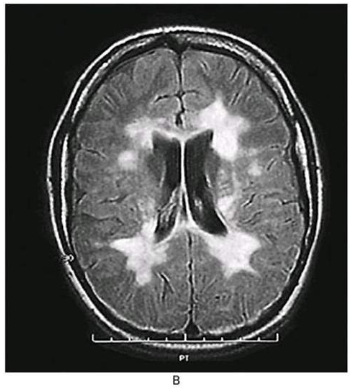
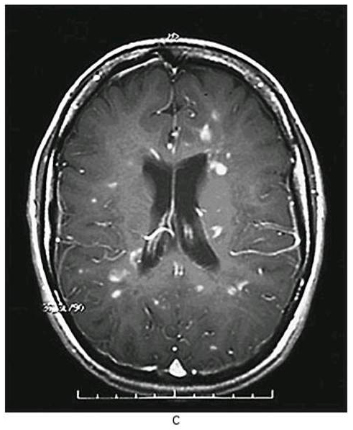
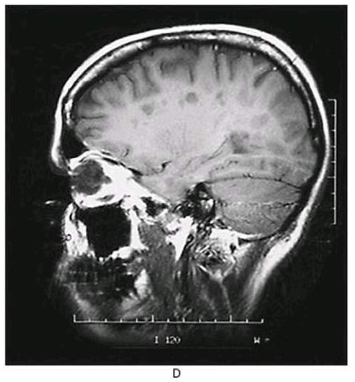
Cerebral MRI shows 6 lesions on T2 imaging.
- 5 are periventricular; one left medial pons.
LP shows pleiocytosis with 35 lymphocytes/mm3, no RBCs, nl protein and glucose.
- Oligoclonal bands seen with no serum abnormalities.
VERs show P100 conduction of 126ms on L and 116 ms on R (nl < 113 with < 7 ms differential).
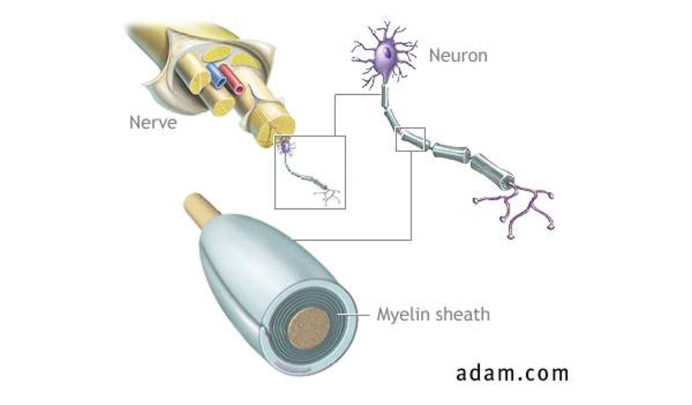
Nerves are made up of axons covered by myelin—allowing uninterrupted speedy transmission.
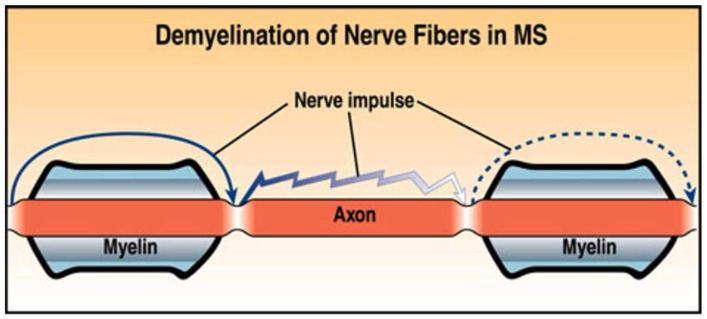
Destruction of the myelin sheath leads to impaired communication between nerve cells and neurological symptoms such as abnormal sensation, vision problems, and weakness.
- Disease-modifying treatment
- Prognosis
- Treatment of Acute Exacerbations.
- Intravenous methylprednisolone for exacerbations.
- Long-term prevention of relapses-multiple agents.
- Disease-Modifying Therapy.
- Alemtuzumab, fingolimod, natalizumab.*
- Primary progressive MS— start with ocrelizumab.
- Disease-Modifying Therapy.
- Monitor with annual MRI and for adverse events (side-effects).
*Natalizumab carries 3/1000 risk of PML (progressive multifocal leukoencephalopathy). Test for JCV (John Cunningham virus) antibody—high titers confer high risk.
Practice Guideline: DMT for Adults with MS.
AAN.com/guidelines (2018). Verified as latest guidelines Oct, 2021.
New treatments are being evaluated all the time. Hot off the presses June 2024: A new trial with another monoclonal antibody, frexalimab, was presented at a conference this spring: Multiple Sclerosis Med Nearly Eliminates Disease Activity on MRI.
- Women better than men.
- Earlier onset is better.
- Remitting is better; once irreversible lesions, prognosis is worse.
- Sensory presentation/CN presentation is better than motor presentation.
Image credits
Unless otherwise noted, images are from Adobe Stock.