

- Migraine with aura: Aura onset precedes or accompanies HA with sx increasing over ~5 minutes and lasting 5–60 minutes.
- Aura: “. . . fully reversible set of neurologic symptoms, often visual or sensory symptoms, that typically develops gradually, recedes, and is then followed by headache accompanied by nausea, vomiting, photophobia, and/or phonophobia.”
- Visual symptoms: Scotomata (negative sx); scintillations (positive sx).
- Migraine without aura (most common): Unilateral, pulsating, n/v, photo/phonophobia, moderate/severe pain, aggravation with activity.
- Ocular migraines (“classic aura without headache”).
- Basilar: Brainstem-predominant symptoms
- Vestibular: Transient vestibular or balance problems without experiencing an actual headache.
- Hemiplegic migraines: Have a rare type of aura that features unilateral weakness, likely due to transient cortical depression.
Criteria for diagnosis
ICHD-3 (Beta) Migraine without aura8
- At least 5 headache attacks fulfilling the criteria B–D.
- Attacks last 4–72 hours.
- With at least 2 of the following characteristics:
- Unilateral location.
- Pulsating quality.
- Moderate or severe pain intensity.
- Aggravation by or causing avoidance of routine physical activity.
- At least 1 of the following during headache:
- Nausea and/or vomiting.
- Photophobia and phonophobia.
- Not better accounted for by another ICHD-3 diagnosis.
ICHD-3 = International Classification of Headache Disorders, 3rd edition.
Criteria for diagnosis
- Same diagnostic criteria as migraine without aura (see prior slide); plus aura.
- Aura can precede headache symptoms by hours to days; generally subsides 5–60 mins prior to onset of headache.
- Common aura: Scintillating scotoma, photophobia, phonophobia, nausea/GI upset.
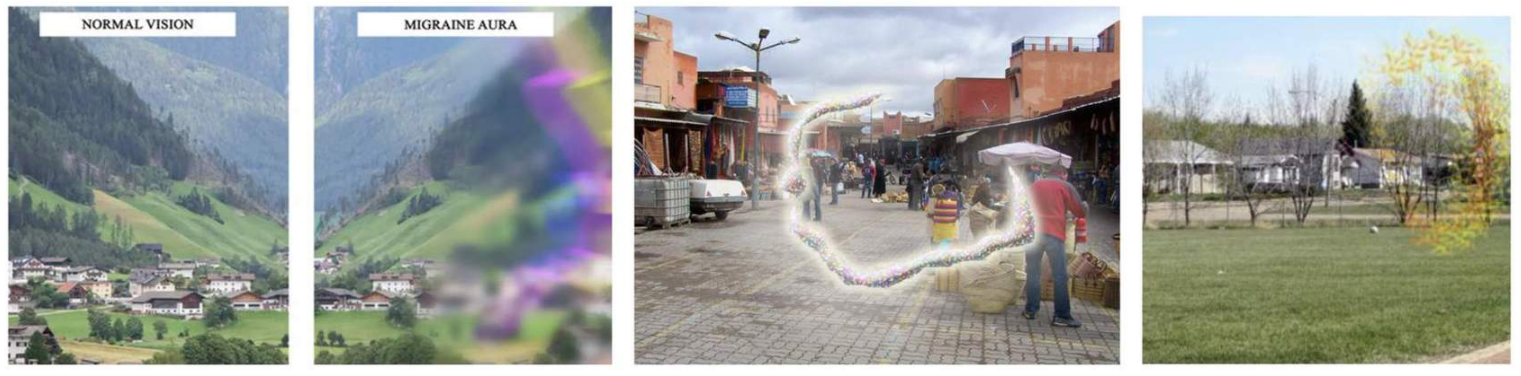
Tap the image to enlarge.