

Author
Keely Coxon, MD
Dawn DeWitt, MD
In this module
Epidemiology of headaches
- Very high lifetime prevalence: 96% by some estimates.
- Migraines: Very common between ages 25–55.
- Female predominance (headaches overall and migraines); except cluster headaches.
- Headaches are a significant cause of morbidity and missed work.
Approach: First distinguish between . . .
Primary headache.
Secondary headache.
Painful cranial neuralgias.
Other: Sinus infection, toothache.
Primary vs. secondary headaches
| Primary headache | Secondary headache | |
|---|---|---|
|
Cause(s) |
Idiopathic; stress, muscle tension, and eye strain (including prolonged screen time) have been identified as common triggers.
|
|
|
Diagnosis |
Clinical findings; absence of red flags |
Clinical presentation; imaging and/or labs usually obtained as red flags tend to be present
|
|
Management |
Depends on type and symptom severity |
Depends on cause |
Headache history and physical
Temporal profile
3 mo detailed hx of total HA days, severe HA days, medication days. Headache diary recommended.
Key components of the physical exam
- Vital signs.
- Palpation of head and face.
- Neurologic exam.
- Especially fundoscopic exam.
- Cardiovascular exam (carotids, heart, pulses).
Essential elements of the headache history
- Family history of migraine.
- Childhood migraine proxy symptoms: carsickness, gastrointestinal complaints.
- Age of onset.
- Frequency, severity, and tempo over time.
- Triggering, aggravating, or alleviating features.
- Autonomic features.
- Aura features.
- Current and prior treatments.
- Lifestyle features.
- Comorbid conditions.
Source: Rizzoli, P. MD, FAHS and Mullally, W. MD, FAHS. Headache. American Journal of Medicine, vol. 131, No. 1, Jan 2018.
Red flags
Headache “red flags” that could indicate need for evaluation
- New headache in older patients
- Abnormal neurologic examination including papilledema and change in mental status
- New change in headache pattern or progressive headache
- New headache in the setting of HIV risk factors, cancer, or immunocompromised status
- Signs of a systemic illness (e.g., fever, stiff neck, rash)
- Triggered by cough, exertion, Valsalva maneuver
- Headache in pregnancy/postpartum period
- First or worst headache
Source: Rizzoli, P. MD, FAHS and Mullally, W. MD, FAHS. Headache. American Journal of Medicine, vol. 131, No. 1, Jan 2018.
Examples of studies used in further evaluation
- CT or MRI.
- Lumbar puncture.
- Neurologic exam.
- Bloodwork for signs of infection or systemic illness.
Primary headache overview
-
Tension-type headache (TTH)
-
Cluster headache
-
Migraine: With or without aura
Subtypes (not discussed here):
- Hemiplegic
- Vestibular
- Basilar-type
- Ocular
-
Trigeminal autonomic cephalalgias (cluster HA is the classic)
-
Other primary headache disorders
- Ice-pick headache: Primary stabbing HA lasting seconds
- Primary cough headache: Seconds to minutes, if atypical use MRI to exclude Chiari malformation
- Exertional headache
- Cold stimulus headache
Headache pain patterns
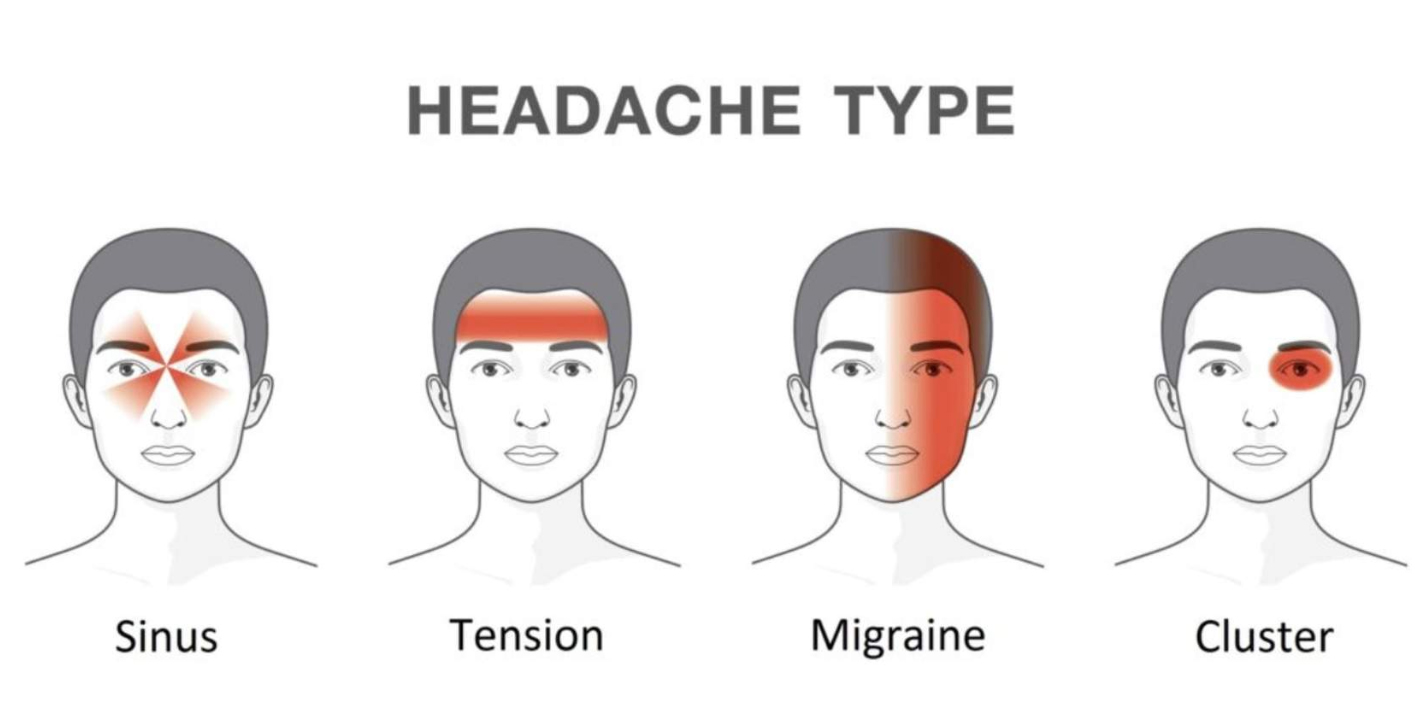
Tension-type headache (TTH)
- Causes
- Signs and Symptoms
- Treatment
- Stress
- Muscle imbalances/bad posture
- Dehydration
- Missing meals
- Squinting or staring at computer screen too long
- Bright light, etc.
- Bilateral, “band-like” pain around the forehead and sides of head
- Often begins at base of neck
- May have tenderness to palpation of pericranial muscles
- No associated aura
- OTC pain relievers: Acetaminophen, NSAIDS, aspirin (beware daily use), Selective 5-HT1B/D serotonin agonists
- Triptans as supplemental abortive therapy if needed
- Avoidance of triggers: Stress
Recommended exercise
- Look up contraindications to:
- Triptans
- Ergotamines
- Gepants
Preventive therapy
- Add CGRP antagonists (calcitonin gene-related peptide antagonists): “Gepants”
*May be effective for patients with significant disability from frequent migraines. Do not use in pregnancy or in patients with CVD. (See UpToDate for a nice detailed discussion.)