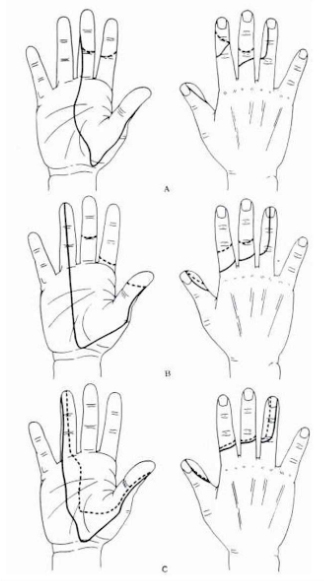
 Approximate areas of sensory changes for median nerve lesions.
Approximate areas of sensory changes for median nerve lesions.
A = small area
B = average area
C = large area
Light touch: Continuous line
Pin prick: Dotted line
Modified from Head and Sherren (1905) Brain, 28, 116.
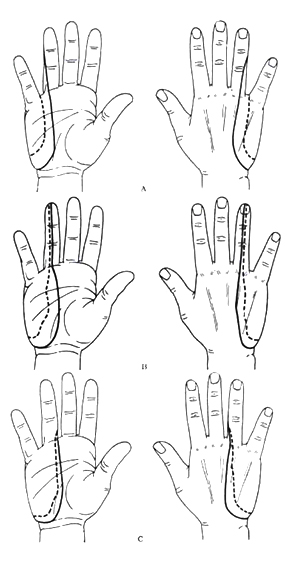 Approximate areas of sensory changes in ulnar nerve lesions.
Approximate areas of sensory changes in ulnar nerve lesions.
A = small area
B = average area
C = large area
Light touch: Continuous line
Pin prick: Dotted line
Modified from Head and Sherren (1905) Brain, 28, 116.
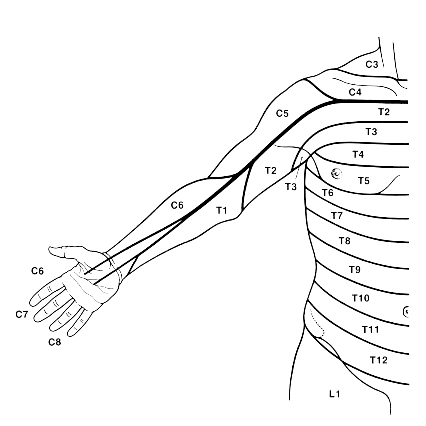
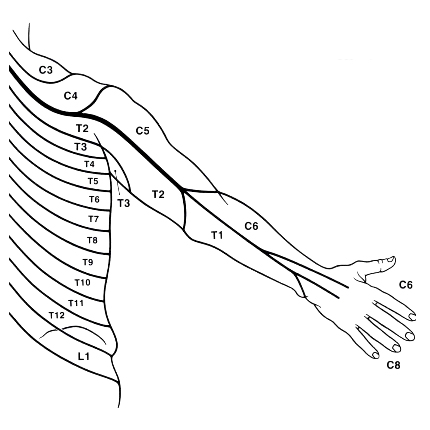
There is considerable variation and overlap.
This variation also applies to the innervation of the fingers, but the thumb is usually supplied by C6 and the little finger usually by C8 (see Inouye and Buchthal (1977) Brain 100: 731-748).
There is considerable variation and overlap.
This variation also applies to the innervation of the fingers, but the thumb is usually supplied by C6 and the little finger usually by C8 (see Inouye and Buchthal (1977) Brain 100: 731-748).
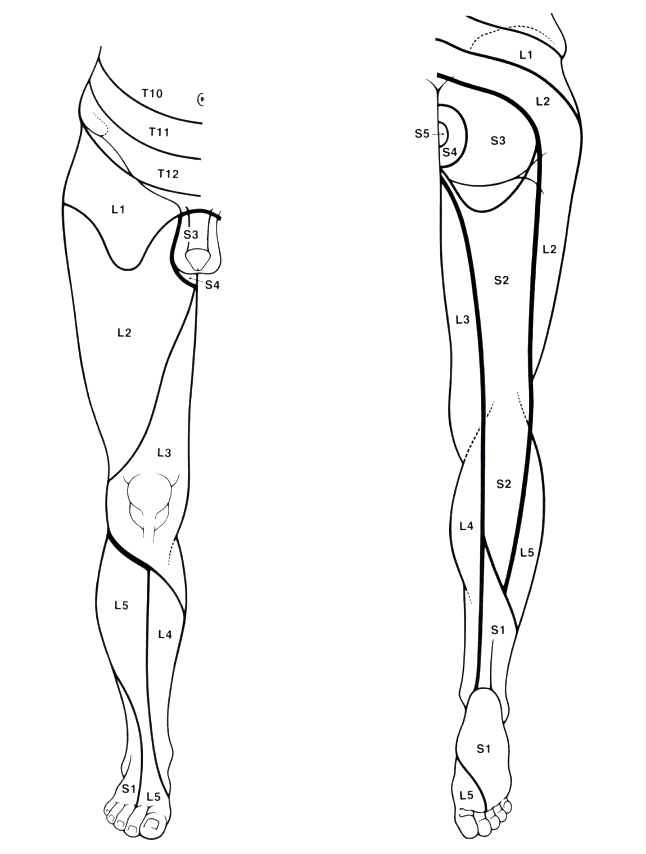
This is most likely cauda equina syndrome, which is a medical emergency and requires urgent surgical consultation.
- Complete neurological examination of the lower extremities and a sensory level should be done, with comparison of strength, sensation, and reflexes to exclude a systemic disease process.
- Peri-anal sensation and rectal tone are an important part of the examination for cauda equina.
- You’re probably thinking that this exam is embarrassing; while that is true potentially for you and the patient, this is a life, or at least mobility-threatening condition, and I often will explain to the patient that if they feel embarrassed, I am happy to talk it through with them or to have a chaperone in the room, while doing everything possible to protect their privacy. I am always careful to explain both what I am doing and my findings as I go along.
Approximate distribution of dermatomes on the perineum
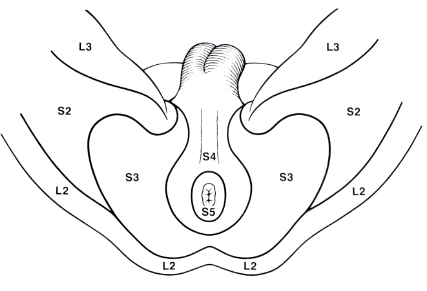
See Inouye and Buchthal (1977) Brain 100: 731–748.
Findings that argue for disc herniation:
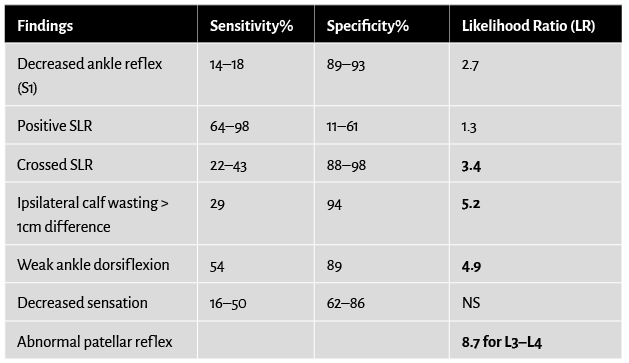
95% of patients with a “herniated” disc have “sciatica.” Deyo, Spine, 1997; McGee, EBMPD, 2007.
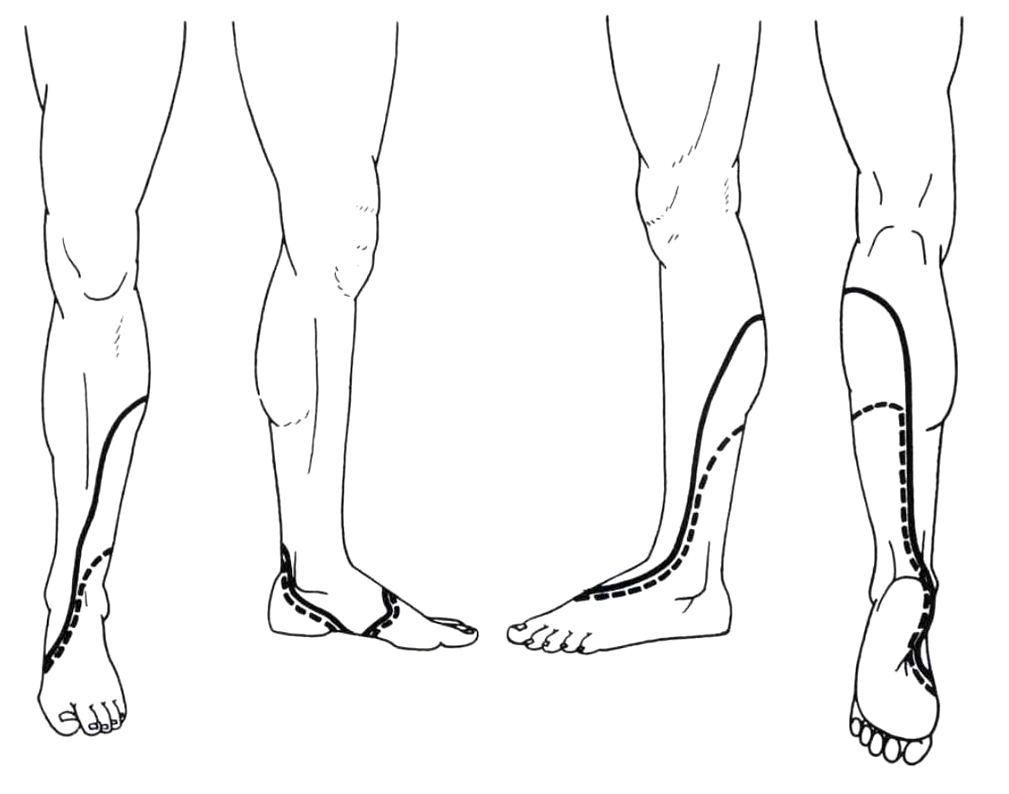
Light touch: Continuous line
Pin prick: Dotted line
Light touch: Continuous line
Pin prick: Dotted line
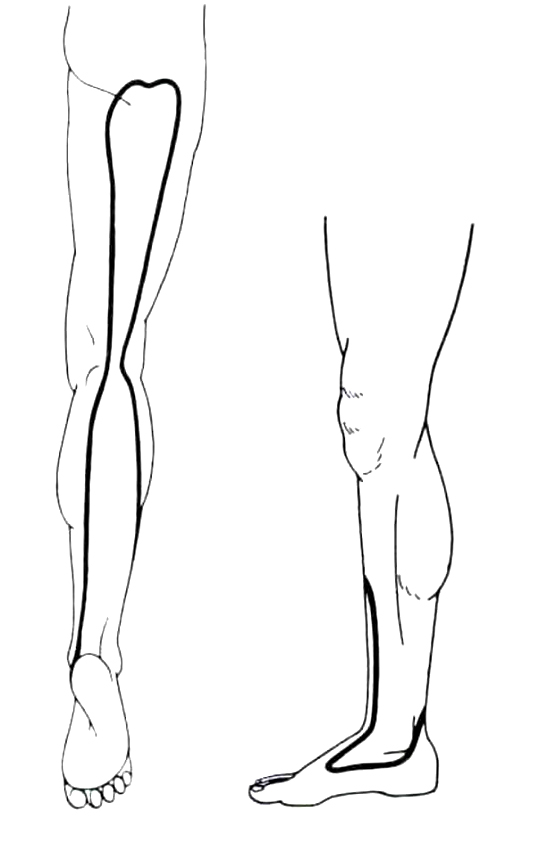
Approximate areas with considerable variation and overlap. (See Inouye and Buchthal (1977) Brain 100: 731–748.)