Instructions for Chapter 17 Worksheets
- Make basic measurements and evaluate for ischemia, infarction, and atrial abnormality.
- Diagnose LVH if criteria listed in Chapter 17 are present.
- Evaluate clinically.
Clinically-Based Critical Thinking: Interpretation
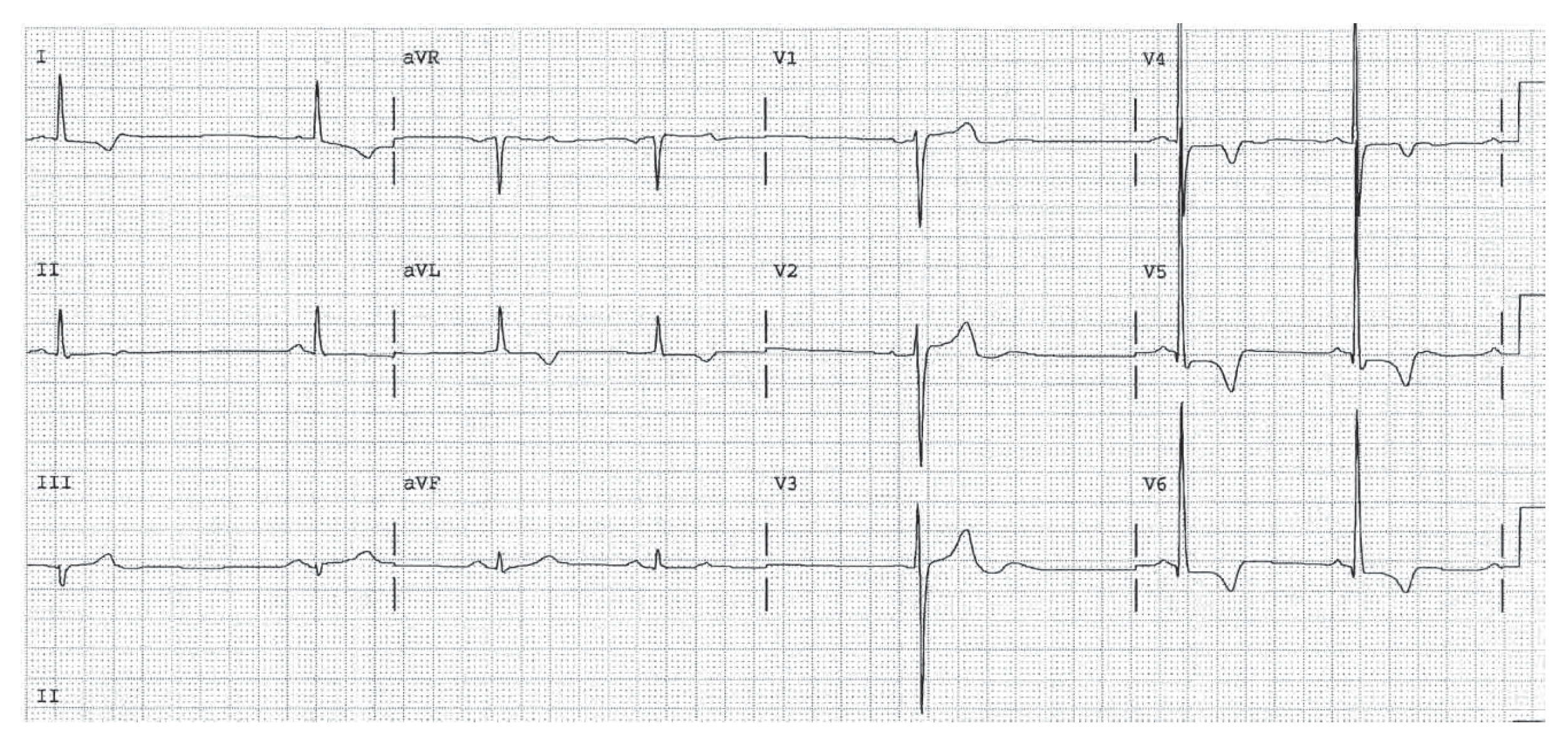
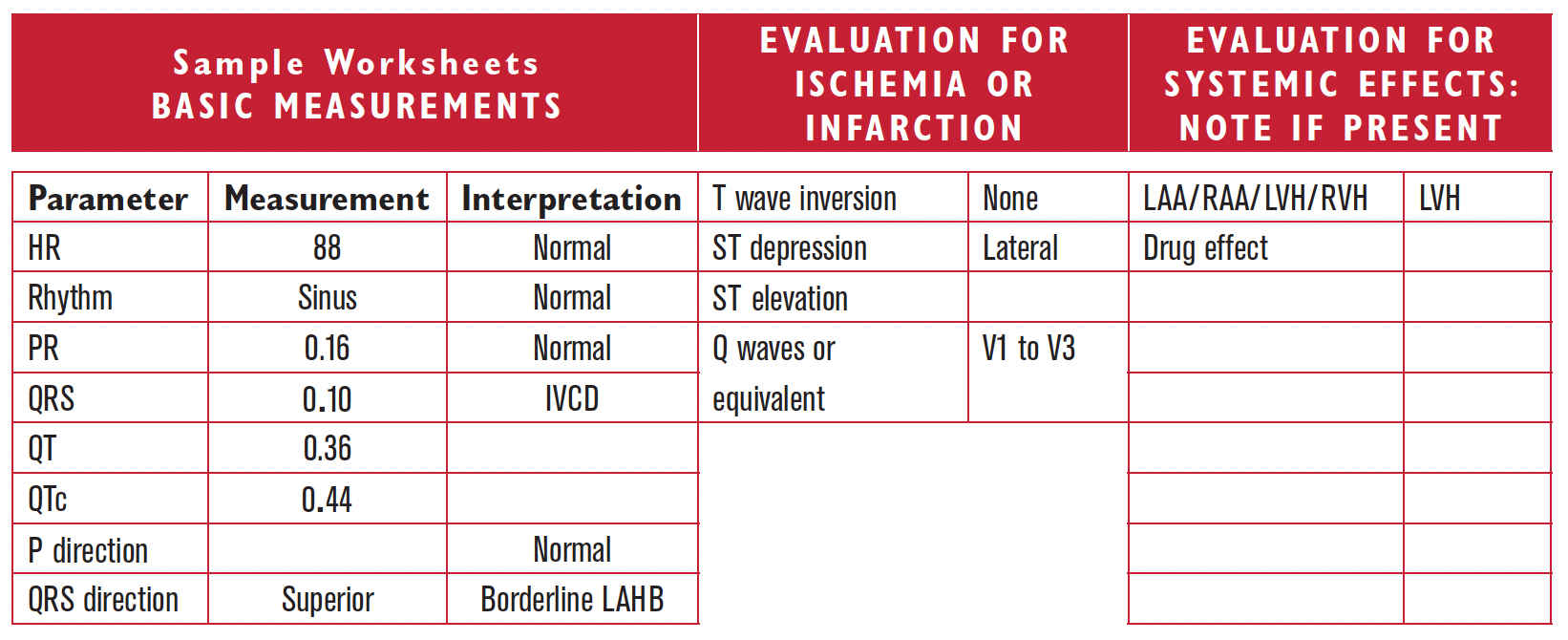
LVH is present by voltage since RI + SIII = 25. There are Q waves (this is not poor R wave progression; these are Q waves) in V1, V2, and V3, and so Q wave infarction criteria of the septum and anterior wall are present as well. A careful inspection of leads I, V5, and V6 shows ST segment depression, which may be due to LVH or to ischemia or infarction. Possible associations include HTN, poorly controlled, with coexistent coronary disease.