
Type 1 DM results from an autoimmune process directed against the pancreatic islet beta-cells. We now know that the process that leads to beta-cell loss of function starts years before diabetes is diagnosed clinically.
In the case of Type 1 DM, the preclinical phase is asymptomatic. One focus of research is to identify patients with pre-clinical diabetes and intervene to prevent progression. At this time, no such treatment is available. Overt diabetes occurs when beta-cell mass drops below 20% of normal.
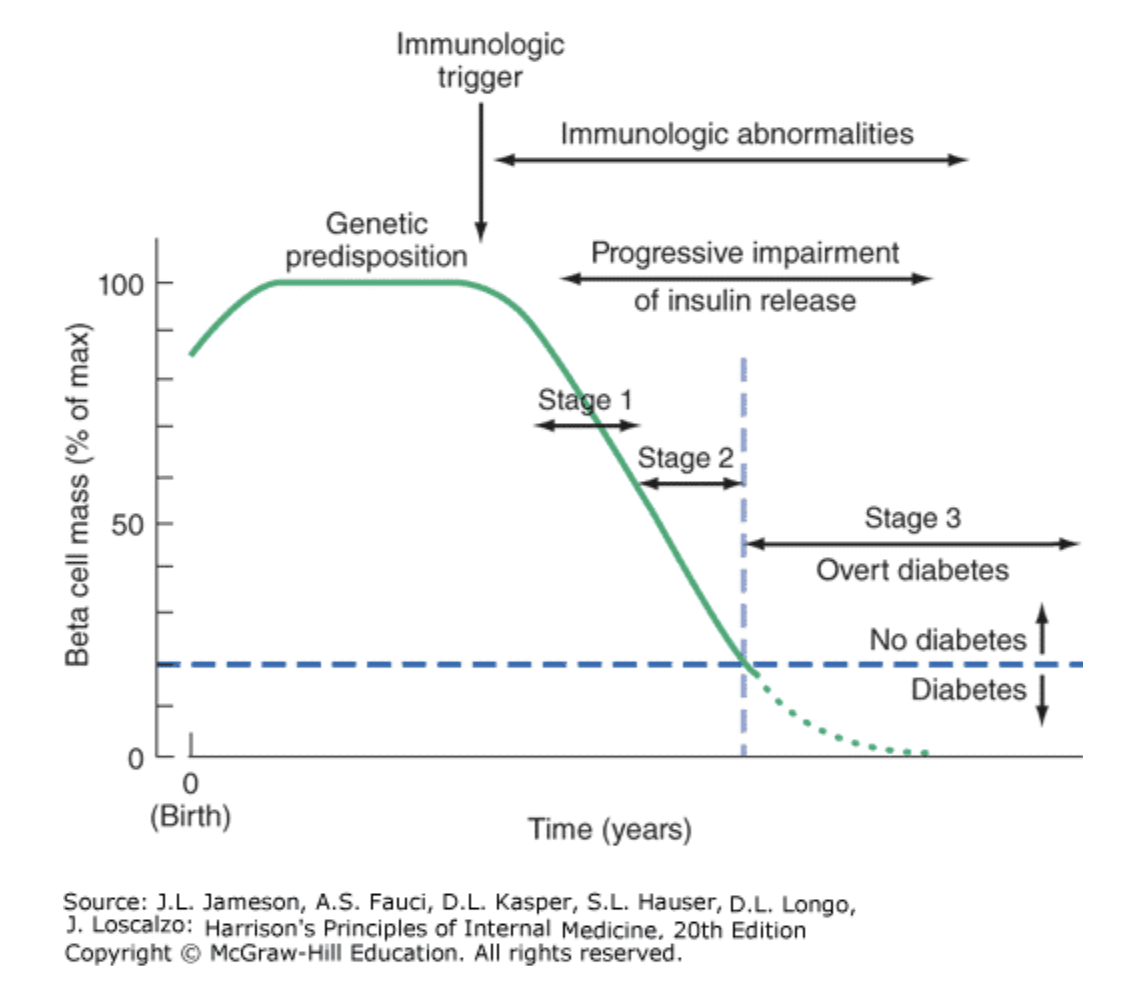
Figure 396-6. Temporal model for development of type 1 diabetes. Individuals with a genetic predisposition are exposed to a trigger that initiates an autoimmune process, resulting in the development of islet autoantibodies and a gradual decline in beta cell function and mass. Stage 1 disease is characterized by the development of two or more islet cell autoantibodies but the maintenance of normoglycemia. Stage 2 disease is defined by continued autoimmunity and the development of dysglycemia. Stage 3 is defined by the development of hyperglycemia that exceeds the diagnostic criteria for the diagnosis of diabetes. The downward slope of the beta cell function varies among individuals and may not be continuous. A “honeymoon” phase may be seen in the first 1 or 2 years after the onset of diabetes and is associated with reduced insulin requirements. Adapted and modified from ER Kaufman: Medical Management of Type 1 Diabetes, 6th ed. American Diabetes Association, Alexandria, VA, 2012. Jameson JL. Harrisons Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018.
Type 2 DM results from the combination of insulin resistance and inadequate insulin secretion. As long as insulin secretion is sufficient to overcome insulin resistance, hyperglycemia doesn’t occur, and you can’t make the diagnosis of DM. However, as beta-cell function declines and insulin secretion drops, hyperglycemia develops and Type 2 DM is diagnosed.
Insulin resistance is a major component of Type 2 DM and is felt to play a major role in the comorbidities of Type 2 DM through mechanisms not yet fully understood. Insulin resistance is addressed in more detail in its own upcoming session.
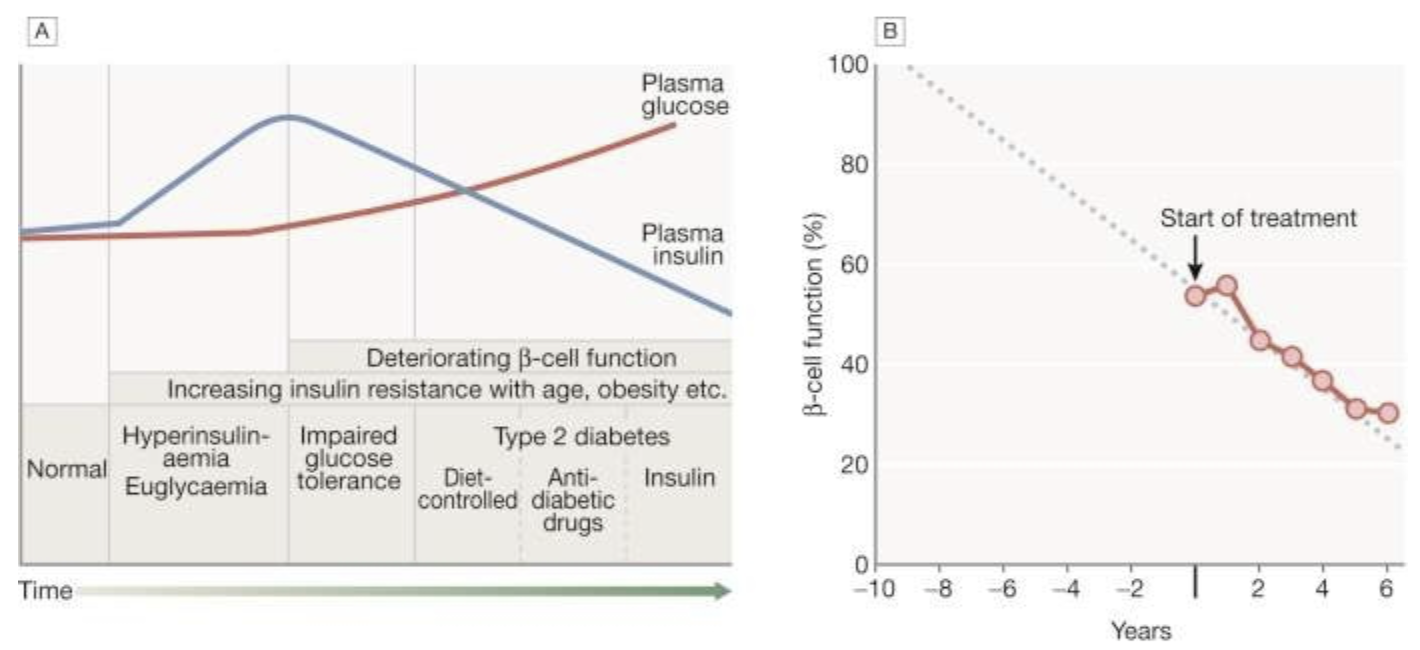
Fig. 20.8 Natural history of type 2 diabetes.
A. In the early stage of the disorder, the response to progressive insulin resistance is an increase in insulin secretion by the pancreatic cells, causing hyperinsulinaemia. Eventually, the β cells are unable to compensate adequately and blood glucose rises, producing hyperglycaemia. With further β-cell failure, glycaemic control deteriorates and treatment requirements escalate.
B. Progressive pancreatic β-cell failure in patients with type 2 diabetes in the United Kingdom Prospective Diabetes Study (UKPDS). Beta-cell function was estimated using the homeostasis model assessment (HOMA) and was already below 50% at the time of diagnosis. Thereafter, long-term incremental increases in fasting plasma glucose were accompanied by progressive β-cell dysfunction. If the slope of this progression is extrapolated, it appears that pancreatic dysfunction may have been developing for many years before diagnosis of diabetes.
B, Adapted from Holman RR. Diabetes Res Clin Pract 1998; 40 (Suppl.):S21–S25.
Ralston SH, Penman ID, Strachan MWJ, Hobson RP, Britton R, Davidson LS. Davidsons Principles and Practice of Medicine. 23rd ed. Edinburgh: Elsevier; 2018.