


Lactose-fermenting gram-negative rod and is abundant in the human colon and genital tract.
There are over 150 distinct serotypes that are defined by their surface antigens, O, K, and H.
-
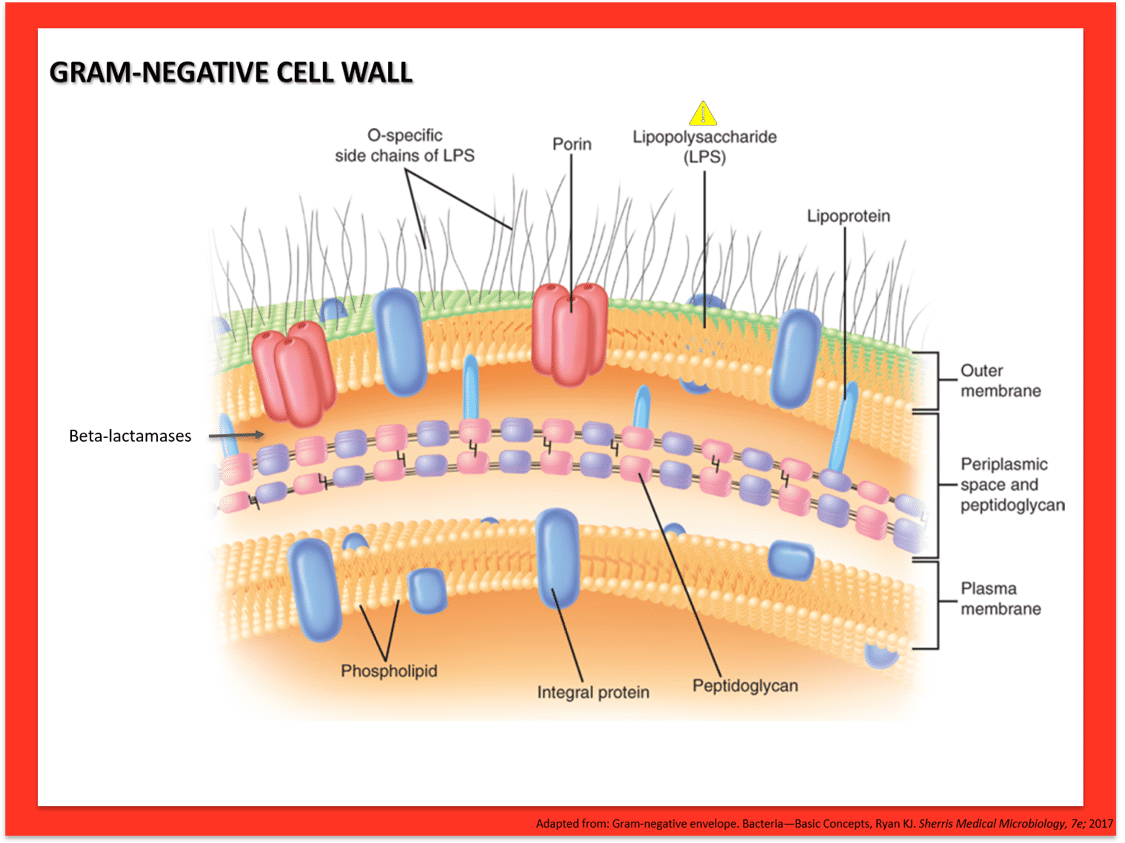
- The O antigen is the polysaccharide unit of LPS.
- The H antigen is flagellar protein.
- The K antigen is a polysaccharide capsule present in some strains.
 E. coli have pili that allow binding to a variety of epithelial cells; these in part predict where colonization and/or disease can occur. Clinical disease occurs opportunistically when organism gains access to usually sterile sites or vulnerable host (urinary tract infections, neonatal sepsis) or new virulent sub-species is acquired, as in diarrheal illnesses when fecal-oral transmission occurs.
E. coli have pili that allow binding to a variety of epithelial cells; these in part predict where colonization and/or disease can occur. Clinical disease occurs opportunistically when organism gains access to usually sterile sites or vulnerable host (urinary tract infections, neonatal sepsis) or new virulent sub-species is acquired, as in diarrheal illnesses when fecal-oral transmission occurs.
E. coli is the most common cause of urinary tract infections.
Neonatal meningitis is acquired during birth and can present with poor tone and respiratory distress. The K1 capsular polysaccharide is the main virulence factor linked with neonatal E. coli sepsis.
Sub-types that cause infectious diarrhea are:
-
- Enterotoxigenic (ETEC): Produces heat-labile toxin (LT) and stable-toxin (ST) that lead to loss of electrolytes from enterocyte; it is the most common cause of traveler’s diarrhea and is generally self-limited.
- Enteropathogenic (EPEC)
- Enteroinvasive (EIEC)
- Enterohemorrhagic (EHEC): EHEC produces Shiga-toxin and is an important cause of bloody diarrhea. It is most commonly associated with O157:H7 serotype. A low infective dose (100organisms) allows for contamination of food over wider distribution networks and larger outbreaks. Hemolytic uremic syndrome with renal failure is a dreaded complication.
- Enteroaggregative (EAEC).
Facultative gram-negative rod with a large polysaccharide capsule, which gives colonies grown on agar a mucoid appearance.
It inhabits the human upper respiratory mucosa and GI tract. It is not as ubiquitous as E.coli but can cause similar opportunistic infections (UTIs, pneumonia, intra-abdominal infections, and sepsis). It is notable as one of the most resistant bacteria in the Enterobacteriaceae family and is a major concern in healthcare-associated infections.
Other than opportunistic infections, distinct clinical entities due to K. pneumoniae include:
-
- Liver abscess, which frequently is associated with K1 or K2 capsular type and is more prevalent in SE Asian regions
- Aspiration pneumonia in chronic alcoholism, where necrotizing infections can be seen and sputum is described as “currant jelly,” reflecting the very mucoid nature of the pathogen
Note: K. pneumoniae pneumonia is not exclusive to alcoholism or aspiration events, but the associated tends to be a board favorite.
Enteric gram-negative rod that causes similar opportunistic infections as K. pneumoniae.
Colonies are easily spotted in the lab with their red pigment. Organisms are water loving (think about the “pink slimy stuff” that accumulates on shower curtains, water fixtures, and toilets).
Enteric gram-negative rod that causes similar opportunistic infections as K. pneumoniae and S. marcescens.
Antibiotic susceptibility is variable, and extensive drug resistance is increasing.
Pseudomonad of most concern in human infections.
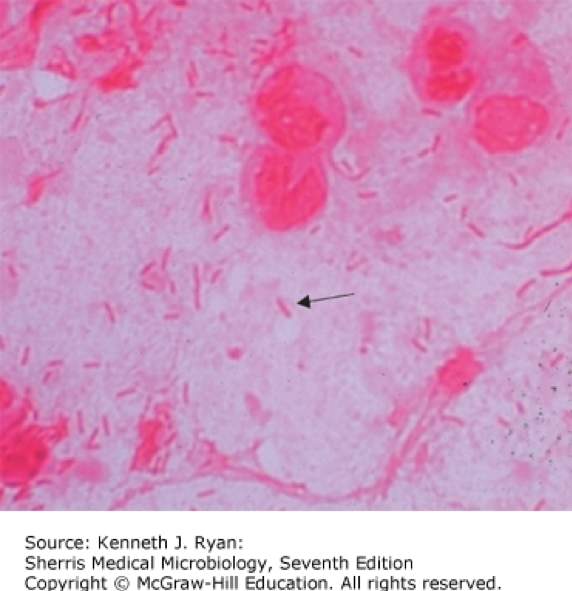
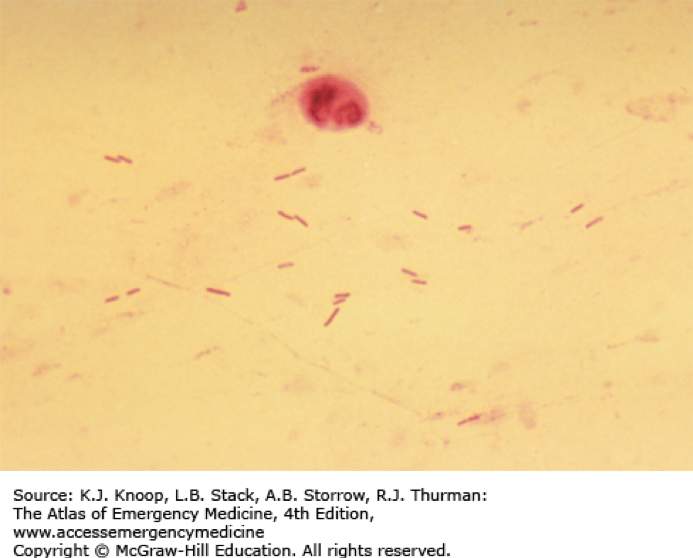 Pseudomonas aeruginosa is an aerobic gram-negative rod that is abundant in environmental water sources. More rarely, it can also inhabit the skin, upper respiratory tract, and GI tract. It is non-lactose-fermenting and oxidase positive, which is typically used to quickly differentiate from other gram-negative infections caused by the Enterobacteraciae. It produces pyocyanin, which gives a blue-green pigment to colonies in the lab, and can be seen clinically on wound infections due to Pseudomonas. Virulence factors include pili and a capsule that facilitate attachment and inhibit phagocytosis. Certain strains are notable for production of thick glycocalyx that produces a biofilm that is particularly difficult to eradicate (see image below).
Pseudomonas aeruginosa is an aerobic gram-negative rod that is abundant in environmental water sources. More rarely, it can also inhabit the skin, upper respiratory tract, and GI tract. It is non-lactose-fermenting and oxidase positive, which is typically used to quickly differentiate from other gram-negative infections caused by the Enterobacteraciae. It produces pyocyanin, which gives a blue-green pigment to colonies in the lab, and can be seen clinically on wound infections due to Pseudomonas. Virulence factors include pili and a capsule that facilitate attachment and inhibit phagocytosis. Certain strains are notable for production of thick glycocalyx that produces a biofilm that is particularly difficult to eradicate (see image below).
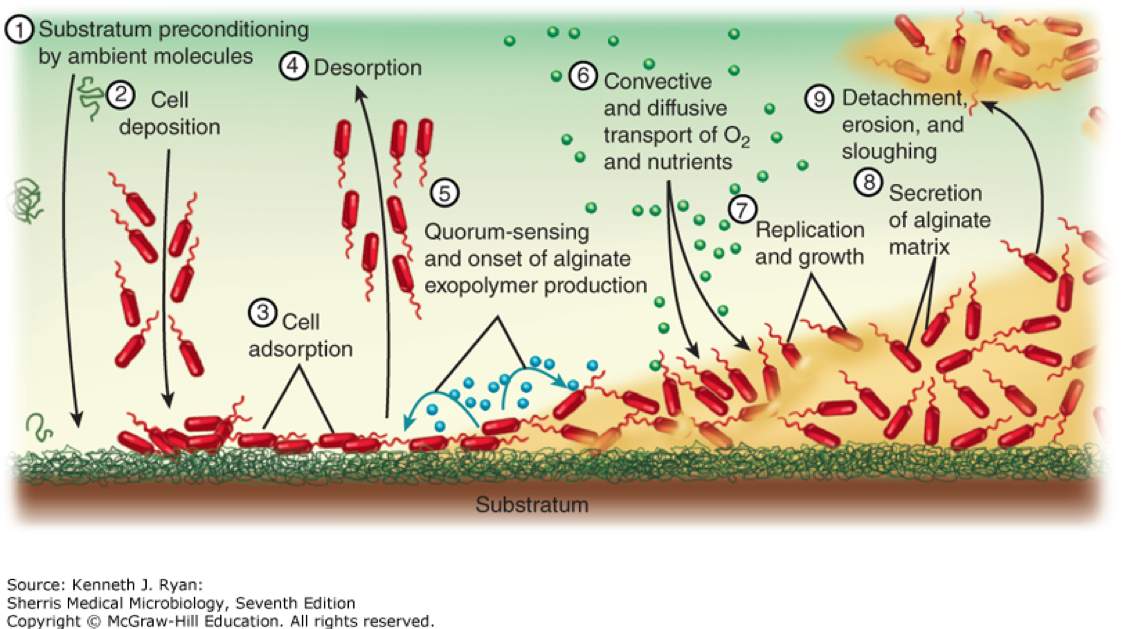
Pseudomonas aeruginosa is one of the most important causes of nosocomial infections. It can be difficult to treat and is associated with poorer outcomes overall. As an opportunist, it can cause infections in virtually all systems:
-
- Bloodstream infections/sepsis
- Pneumonia
- UTI
- Wounds
- Devices infections
- Neurosurgical/CNS
These infections are more common in patients with exposure to broad-spectrum antibiotics and those patients with significant immunosuppression and multiple medical co-morbidities.
Specific clinical syndromes of note include:
-
- Pneumonia in cystic fibrosis or other forms of bronchiectasis or severely altered respiratory anatomy
- Burn infections
- Ecthyma gangrenosum: Cutaneous necrotic popular eruption as a result of P. aeruginosa bacteremia in patients with severe immunosuppression, most often related to myeloablative chemotherapy
- Otitis externa due to P. aeruginosa can occur in immunocompetent persons where it is simply known as “Swimmer’s ear.” A more serious and potentially life-threatening version occurs in uncontrolled diabetes where it is termed “malignant otitis externa.”
- Infectious keratitis or conjunctivitis is frequently associated with contact lenses and contaminated cleaning solution or ophthalmic medications.
- “Hot-tub folliculitis” is a follicular eruption as a result of soaking in hot tubs heavily colonized with the organism. Eruption is most often limited
Treatment of Pseudomonas is difficult to naturally occurring resistant porins that restrict entry to many antibiotics, and variable plasmid mediated resistance mechanisms. They are uniformly resistant to penicillin, ampicillin, 1st- and 2nd-gen cephalosporins, tetracyclines, sulfonamides, ertapenem, and some fluroquinolones. There are few oral agents for use in treating pseudomonal infections.
Current anti-pseudomonal agents are:
-
- Piperacillin-tazobactam
- Cefepime
- Ceftazidime
- Cefoperazone
- Ceftolozane-tazobactam
- Aztreonam
- Ciprofloxacin
- Levofloxacin
- Carbapenems (except ertapenem)
- Aminoglycosides (except streptomycin and kanamycin)
- Polymixins