The nose is the portion of the respiratory tract above the palate. It consists of two parts: an external nose on the face and an internal portion called the nasal cavity. There are two nasal cavities, left and right, separated by the nasal septum.
External nose
The external nose is shaped like a three-sided pyramid, with the base facing down. It projects from the face in order to direct air into the nasal cavities.
Named parts
Dorsum (bridge): The midline margin of the nose where the two sides meet, similar to the center peak in the roof line of your home. It connects the root of the nose (the part between the eyes, continuous with the forehead) and the apex (tip).
Alae (singular: ala): The flared sides of the pyramid, continuous with the upper cheeks.
Nares (nostrils): The external openings of the nose.
The nostrils are separated by the lower border of the nasal septum, called the mobile nasal septum (columella).
Just inside the nostrils is a small skin-lined region called the vestibule. Technically it is the most anterior part of the nasal cavity. It contains stiff hairs called vibrissae.
Figure 34.1. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 35.
The skeleton of the external nose is composed of the nasal bones with small contributions from the frontal bones and maxillae. However, most of the underlying framework of the external nose is made of nasal cartilages.
The bony opening into the nasal cavity seen in the dried skull is the piriform aperture (piriform = “pear- shaped”). It is surrounded by the nasal bones and maxillae.
The cartilages of the nose are attached around the edges of the piriform aperture and are the major supporting structures of the nose. This provides the external nose with considerable mobility.
Paired major alar cartilages are U-shaped structures that surround the nostrils. Each contains a medial and lateral crus. Left and right medial crura join in the midline between the nostrils contributing to the mobile part of the nasal septum (columella). Their inferior margins can easily be felt by palpation. The lateral crura are embedded in the alae of the external nose.
The lateral nasal cartilages are above, attached to the nasal bones and maxillae. In the midline they fuse with each other and with the septal cartilage, which projects backward into the head to connect with the bony nasal septum.
Clinical correlation The size and shape of the external nose is to a large extent dependent on the shape and configuration of the underlying cartilages. They can be reshaped in a surgical procedure called rhinoplasty. This is usually performed for cosmetic reasons or to improve breathing.
Small nasalis muscles attach to the cartilages of the nose. They have two parts that function to dilate (flare) or constrict (narrow) the nostrils. These are muscles of facial expression, so they are innervated by CN VII.
The dorsum of the nose receives small branches from the ophthalmic artery in the orbit (derived from the internal carotid artery).
The alae are supplied by branches of the facial arteries.
Clinical correlation
“Broken nose” is the term used to describe fracture of the nasal bones. In cases of facial trauma, nasal bones account for about 40% of all fractures. They are usually the result of sports injuries or fights.
Nasal septum
Figure 34.2. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 38.
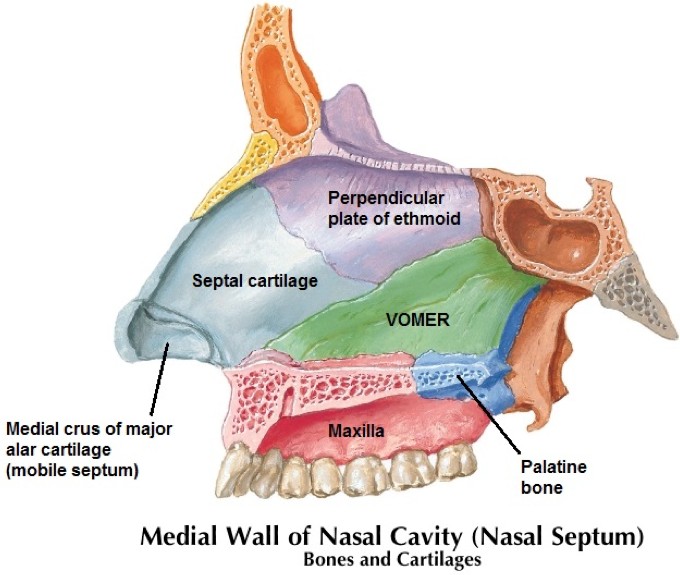
The nasal septum separates the left and right nasal cavities, thus forming their medial walls. It is covered with a mucous membrane and constructed of three parts:
Anterior
The most anterior part between the nostrils is the mobile nasal septum (columella) described earlier. It contains the medial crura of the major alar cartilages and dense connective tissue.
Central
The central portion is the tough septal cartilage.
Posterior
The posterior part is the thin bony nasal septum, made from the perpendicular plate of the ethmoid bone and the plow-shaped vomer.
Clinical correlation
The nasal septum is often not in the midline, so deviated septum is a common disorder. It can be congenital or caused by trauma and can lead to airway obstruction, sinus infections (due to impaired drainage), or snoring and sleep apnea. They may be asymptomatic, but if they are problematic, the treatment is surgical (septoplasty) where the cartilage is reshaped under anesthesia.
Clinical correlation
A septal perforation is a hole through the septal cartilage. This can be a result of infection, nasal piercings, surgery, nasal steroid sprays, or cocaine. Symptoms vary and are more serious the closer to the nostrils, producing bleeding and wheezing noises.
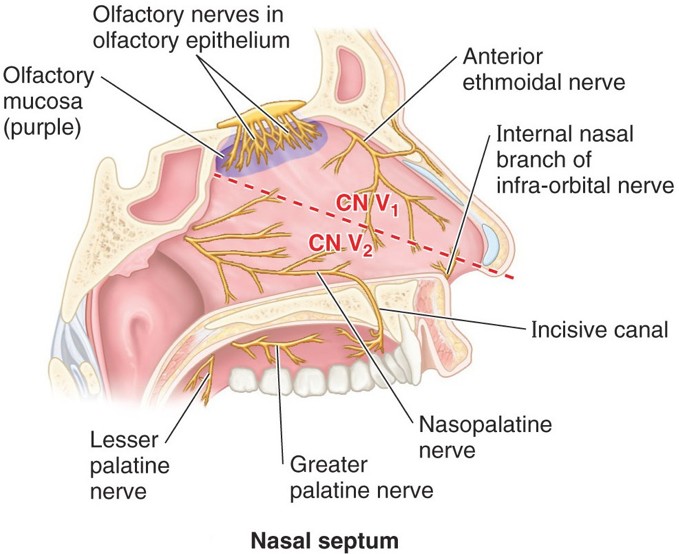
Nerves from both the ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve supply the nasal septum. An oblique line drawn from the nostril to the sphenoidal (paranasal) sinus in the posterior roof of the nasal cavity can be used to demarcate their distributions.
Anterosuperior part: Anterior ethmoidal nerve from V1.
Postero-inferior part: Nasopalatine nerve from V2.
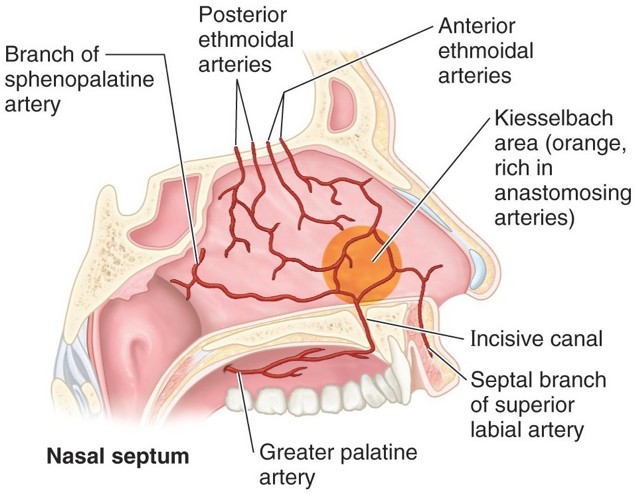
The nasal septum, like the rest of the nasal cavity, receives a rich blood supply from branches of both the internal and external carotid arteries (5 branches total), in order to warm and humidify inspired air.
From the internal carotid:
Anterior and
Posterior ethmoidal arteries (both from the ophthalmic artery).
From the external carotid:
Septal branches of
Sphenopalatine artery (from the maxillary artery)
Superior labial artery (from the facial artery); and
Greater palatine artery (from the maxillary artery), via the incisive fossa.
The five sources of blood listed above anastomose in the anterior part of the nasal septum, forming a network of vessels called Kiesselbach’s plexus.
Clinical correlation
Epistaxsis is bleeding from the nose. 90% of nosebleeds are minor and occur in the region of Kiesselbach’s plexus (anterior epistaxsis).
Bleeding in the posterior nasal cavity (posterior epistaxsis) can be life threatening. The vessels (often the sphenopalatine artery) are larger and not externally compressible, compared to the more common anterior nosebleeds. They are usually associated with coagulopathy and hypertension. The treatment involves remedying the underlying condition, compression of the vessels by packing the nasal cavity, and in some cases, surgical ligation of the damaged vessels.
Nasal cavities
Each nasal cavity is triangular in shape when viewed from the front: narrow above and wider below.
They have openings on each end:
Anterior
Anteriorly, the nostrils (anterior nares) open onto the face.
Posterior
Posteriorly, the choanae (posterior nares) connect the nasal cavities to the nasopharynx.
Boundaries of the nasal cavities
Medial walls
Nasal septum (discussed earlier).
Lateral walls
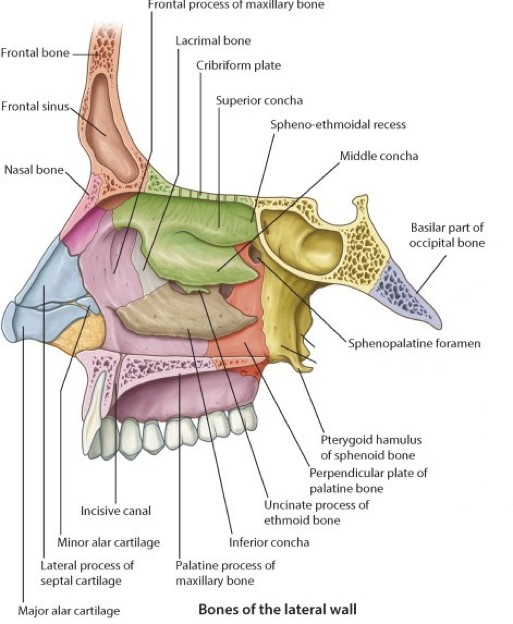
Complex, consisting of bone and cartilage. The bones include the frontal, lacrimal, ethmoid, maxilla, palatine, sphenoid, and inferior nasal concha.
Floor
Hard palate.
Roof
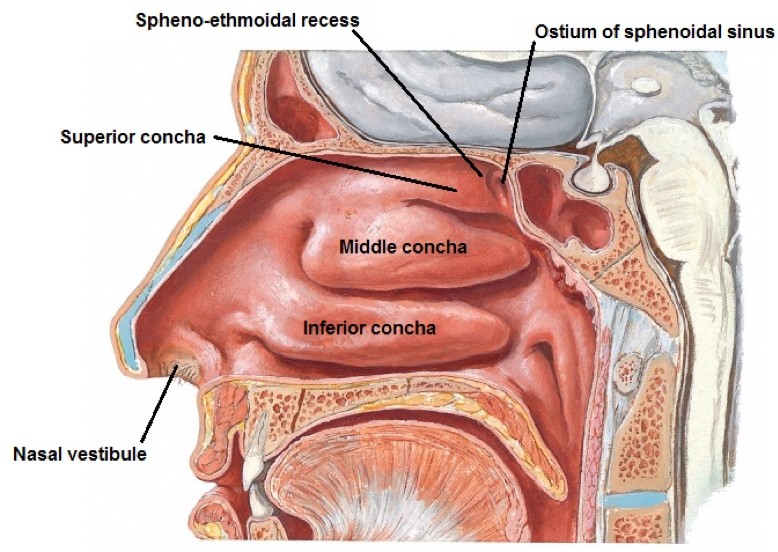
Cribriform plate of the ethmoid bone and body of the sphenoid bone. The uppermost region of the nasal cavity anterior to the curved border of the sphenoid body is the spheno-ethmoidal recess. The ostium of the sphenoid air sinus opens here.
The nasal cavity lies immediately medial to the orbit and inferior to the anterior cranial fossa (containing meninges and frontal lobes of the brain). Head trauma leading to fracture of the cribriform plate may cause cerebrospinal fluid (CSF) to leak into the nasal cavity and out the nostrils. This is called CSF rhinorrhea.
Operations on the pituitary gland can be performed through the nasal cavity by a transphenoidal approach (through the sphenoid body in the roof of the nasal cavity).
Lateral walls of nasal cavities
Figure 34.6. Lateral nasal wall. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 36.
Projecting into each nasal cavity from their lateral walls are three or four thin scroll-shaped bones called conchae (Latin: shell). These are also called turbinates, especially by ENT docs, because they cause turbulence in the airflow. They greatly increase the respiratory surface of the nasal cavities.
The superior and middle conchae are parts of the ethmoid bone.
The inferior concha is the largest of the turbinates and is a separate bone.
The presence of the conchae makes the nasal cavities quite narrow from side-to-side explaining why irritation and swelling of the nasal mucosa easily produces a stuffy nose.
The air passageways deep to the conchae are the superior, middle, and inferior nasal meatuses, respectively. Air flowing above the superior concha enters the spheno-ethmoidal recess.
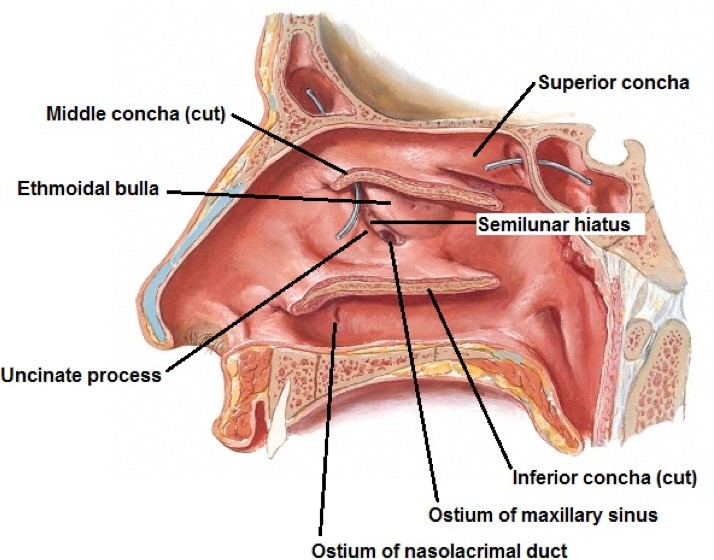
Figure 34.7. Lateral wall of nasal cavity, middle and inferior concha removed. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 36.
Features of the ethmoid bone important to the functions of the nasal cavity are located within the middle meatus and can be observed when the middle concha is removed. See Figure 34.7. These are:
Ethmoid bulla (Latin: bubble): Rounded bulge below the attachment of the middle concha produced by underlying air-filled cavities (described later).
Uncinate process (“hook-shaped”): Curved ridge of bone anterior and inferior to the bulla.
Semilunar hiatus: The curved gap between the bulla and uncinate process.
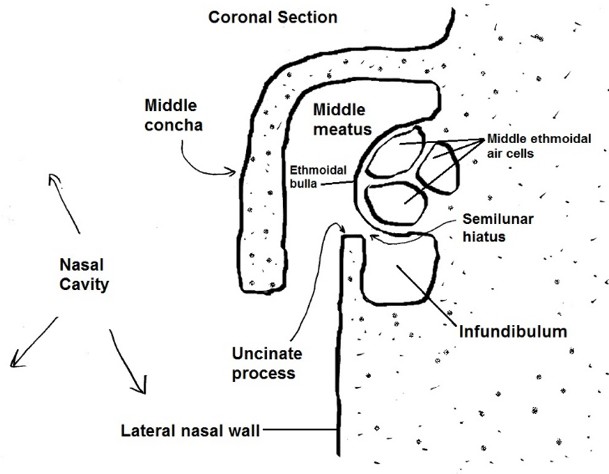
Ethmoid infundibulum: Curved channel deep to the semilunar hiatus; projects forward and upward toward the frontal bone.
Clinicians and surgeons refer to the above structures associated with the middle meatus collectively as the ostiomeatal unit. It is important clinically because this part of the middle meatus receives the drainage of many of the paranasal sinuses.
Figure 34.8. Anatomy of the middle meatus, coronal section, showing the location of the infundibulum, a side channel of the middle meatus into which many of the paranasal sinuses drain. HAND-DRAWN CONLEY- GRAM.
Within the inferior meatus is the ostium of the nasolacrimal duct. This is the inferior extension of the lacrimal sac, located in the anteromedial corner of the orbit. The lacrimal sac collects tears after they have passed across the eyeball when blinking. Tears clean the eyeball and are then disposed of after cilia in the nasal cavities move them to the pharynx,where they are swallowed. Excess tears due to crying or eyeball irritation flood the nasolacrimal duct and cause a runny nose.
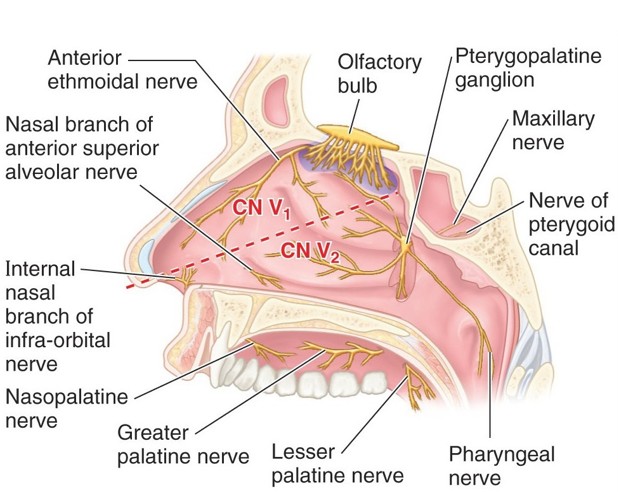
The pattern of nerves to the lateral nasal wall resembles that of the nasal septum, for both general sensation and smell.
Anterior/superior: Anterior ethmoidal nerve, derived from V1.
Posterior/inferior: Nasal branches to the lateral wall are from the greater palatine nerve as it descends from the pterygopalatine ganglion towards the palate. The greater palatine nerve and its nasal branches are derived from V2.
Olfactory nerves, concerned with smell only, are in the mucosa high on the lateral nasal wall above the superior concha, and in a similar region of the nasal septum.
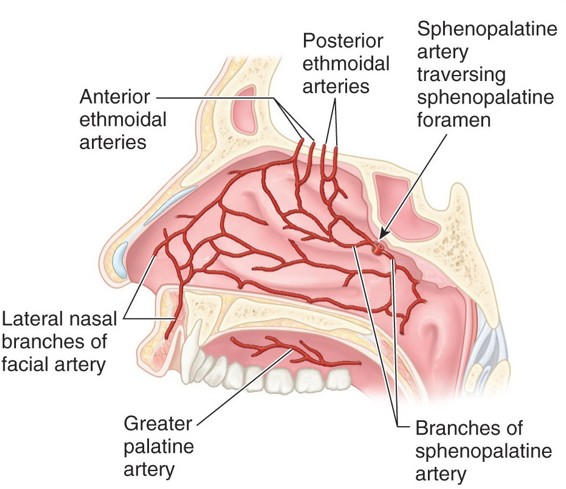
Similar to nasal septum; five arteries contribute and blood is derived from both internal and external carotid arteries.
The most important source is the sphenopalatine artery, a branch of the maxillary artery. This enters the nasal cavity from the pterygopalatine fossa via the sphenopalatine foramen.
Venous drainage of the nasal cavity follows the arteries, to the ophthalmic veins in the orbit and to the pterygoid venous plexus in the infratemporal fossa.
Lymphatics follow those of the pharynx to the deep cervical lymph nodes.
Nasal mucosa
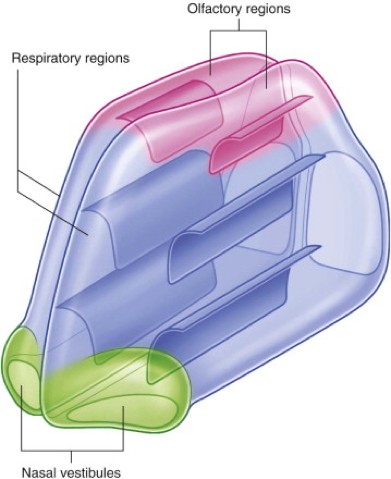
Figure 34.11. Regions of the nasal cavity. Skin lines the nasal vestibules, thick respiratory mucosa lines the respiratory regions, and olfactory neurons arise in the olfactory regions. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.228.
Most of the nasal cavity, including the conchae, meatuses, and septum, contains a thick mucosa with a pseudostratified columnar epithelium (rich with cilia and mucous glands). This constitutes the respiratory region of the nasal cavity, which functions to filter, warm, and humidify the inhaled air. The mucosa contains a massive venous plexus that can dilate rapidly when irritated. The mucous membrane of the conchae is particularly vascular and sponge-like in cross-section, resembling erectile tissue. Nasal congestion results when vessels dilate and mucous glands are overactive. The vestibule of the nasal cavity, just inside the nostrils, is lined by skin, not respiratory mucosa.
High in the nasal cavities, on and above the superior conchae on the lateral walls and in a similar region on the nasal septum, the mucosa thins to form the olfactory region, where the olfactory nerves arise. Lesser volumes of air flow over this region during quiet respiration. Sniffing carries air higher in the nasal cavity so that more of it flows over the olfactory region, allowing one to get a better whiff of odors.
Clinical correlation
Allergic rhinitis is a very common condition (up to 25% of the population). It is a result of exposure to an allergen and the resultant inflammatory cascade. Treatment is removal of the offending allergen and medical therapy for symptomatic relief (intranasal steroid sprays, antihistamines, immunotherapy, etc.).
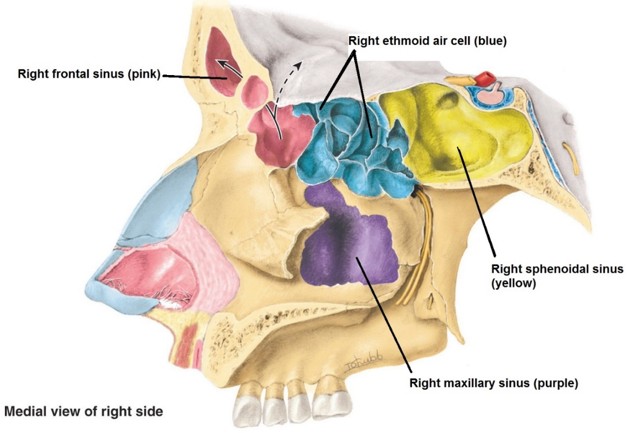
Figure 34.12. The walls between the right paranasal sinuses and the right nasal cavity have been opened and the sinuses color coded. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 7.107.
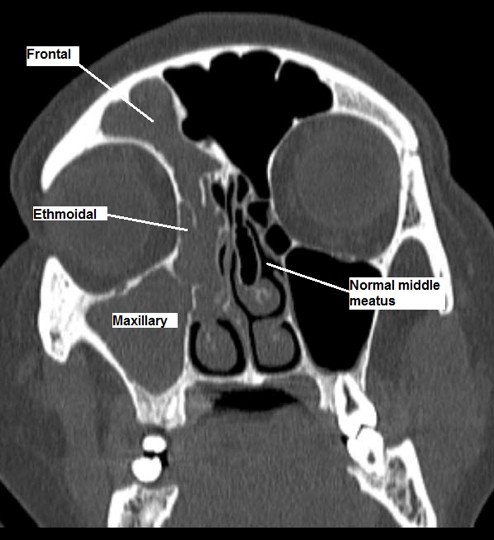
Figure 34.13. Coronal CT image of nasal cavities and adjacent sinuses. GRAY’S ATLAS OF ANATOMY, 2ND ED.
Paranasal sinuses
Figure 34.14.
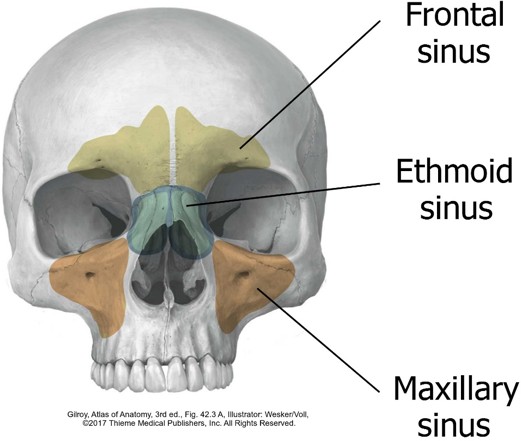
The paranasal sinuses are diverticula of the nasal cavities, growing out into neighboring bones. They are lined by respiratory mucosa and are connected to the nasal cavities via small ostia. They most likely function to increase the mucosal surface area in order to warm, humidify, and filter inspired air. They are also important for vocal resonance. There is speculation that they may also lighten the head and act as collapsible “air bags” that protect the brain and other organs deeper in the head when there is traumatic injury to the face. There are four sets of sinuses, named for the bones in which they are located:
Frontal
Paired, but never of equal size. One sinus may be dramatically larger than the other and cross the midline.
Maxillary
Paired, the largest of the paranasal sinuses. Located below the floor of the orbit.
Sphenoid
Paired, but often asymmetrical. Located within the body of the sphenoid bone below the sella turcica and pituitary gland.
Ethmoidal
Rather than a pair of sinuses, these are small air-filled“cells,” resembling a honeycomb, of variable number and size. The ethmoidal cells are grouped as anterior, middle, and posterior ethmoidal air cells. This organization reflects their development and drainage.
The ethmoid air cells are in close proximity to the orbit, separated from it by an extremely thin lamina of bone called the orbital plate (lamina orbitalis) of the ethmoid bone. Clinicians refer to this “paper thin” layer of bone as the lamina papyracea.
Clinical correlation
Because of their proximity to the orbit and cranial cavity, serious complications could arise from chronic sinusitis. Orbital infections (cellulitis) are most often related to sinusitis. Other conditions such as meningitis or osteomyelitis are rare, but could occur.
Drainage of paranasal sinuses
The locations of the ostia of paranasal sinuses in the nasal cavity is variable, but is typically near the sinuses themselves. This is the general pattern:
Frontal sinus
Infundibulum of middle meatus.
Maxillary sinus
Infundibulum of middle meatus.
Sphenoidal sinus
Spheno-ethmoidal recess.
Ethmoidal air cells
The groups have different drainage patterns:
Anterior cells: Infundibulum of middle meatus.
Middle cells: These produce the ethmoid bulla, so their ostia are on the bulla itself, within the middle meatus.
Figure 34.16. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 45.
Clinical correlation
Note that most of the paranasal sinuses (except the posterior ethmoidal cells and the sphenoidal sinus) drain in or around the ostiomeatal unit (middle meatus). If the unit becomes obstructed, the sinus ostia are blocked, setting up conditions for sinus inflammation. This is known as the ostiomeatal pattern of sinus infection (see Figure 34.17).
Figure 34.17. Ostiomeatal pattern of sinusitis on the right side. Sinus drainage to the middle meatus was blocked, resulting in inflammation of sinuses that drain there (opacities). Compare with normal sinuses on left side. RADPOD.ORG. LABELED FOR FREE USAGE.
From the position of their openings, it can be seen that only the frontal sinus has gravity drainage when the head is upright. The maxillary and sphenoidal sinuses and ethmoid cells do not. In fact, the ostium of the maxillary sinus sits high on its medial wall! All sinuses have a ciliated epithelium that beats toward their ostia. This is the natural mechanism for sinus drainage, not gravity. Under normal conditions, drainage is unidirectional —first carried to the nasal cavity, then to the pharynx where it is swallowed. When the ostia of paranasal sinuses becomes blocked or swollen, the ciliary action cannot empty the sinuses. This sets up an outflow tract stasis where there is backflow contamination of the sinuses, leading to their inflammation, known as sinusitis.
Sinuses can be visualized on skull radiographs or more commonly with CT. Healthy sinuses appear as black (air-filled) spaces. When infected the walls become thickened and the sinuses fluid-filled, producing opacities.
The nasal cavities develop from nasal pits = invaginations of ectoderm on the face. As the nasal pits grow and enlarge, they become known as nasal sacs. The nasal sacs are separated from the oral cavity by a membrane which ruptures during the sixth week of development.
The development of the external nose will be covered with development of the face.
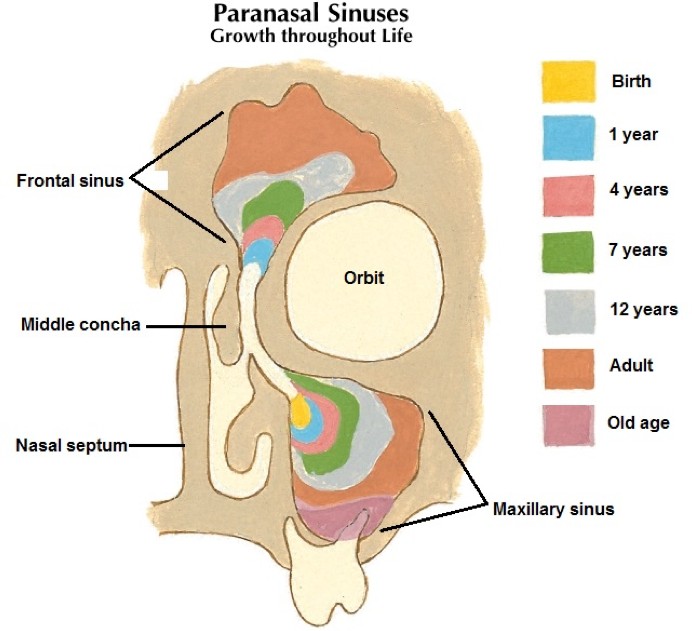
The paranasal sinuses are poorly developed at birth. The maxillary sinuses are the first to begin development, probably during late fetal life. The others are rudimentary diverticula at birth. The maxillary sinuses grow slowly until puberty and are not fully developed until all the permanent teeth have erupted in early adulthood. The frontal sinuses invade the frontal bones during early puberty.
Growth of the paranasal sinuses is an important factor in changing the size and shape of the face during childhood and adolescence and in adding resonance to the voice during puberty.