Figure 22.1 GRAY’S ATLAS OF ANATOMY, 2ND ED., PG. 291.
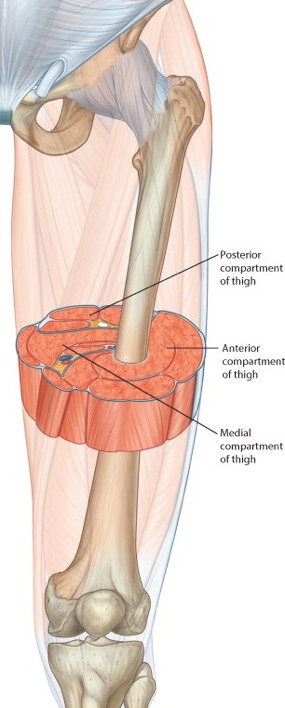
The deep fascia, intermuscular septa, and femur together define anterior and posterior compartments in the thigh.
The anterior compartment contains muscles that flex the hip and extend the knee. The bulk of the musculature in the anterior thigh is made up by the quadriceps femoris.
The posterior compartment of the thigh contains muscles that extend the hip, adduct the hip, and flex the knee. The latter muscles collectively are known as the hamstrings.
A thin intermuscular septum separates the hamstrings from the adductor muscles in the medial thigh. Thus, it is customary to consider the medial part of the posterior compartment as a separate medial compartment or adductor compartment.
Muscles in the anterior compartment are derived from the embryonic dorsal muscle mass and are supplied by posterior divisions of the lumbosacral plexus, while those on the posterior side (and medial side) come from the ventral muscle mass and receive their innervations from anterior divisions of the plexus. This is opposite to the scheme we learned in the arm, but makes sense if you recall that the lower limb underwent rotation in the embryo in an opposite direction to that of the upper limb.
For ease of description and dissection in the lab, we will consider the anterior and medial compartments together in this chapter, even though their muscles come from different primordial muscle masses.
This muscle receives its name from its “four heads,” each having a separate proximal attachment (origin). Distally the heads blend together into a common quadriceps tendon, through which the quadriceps inserts into the base of the patella. The patella is a sesamoid bone that develops within the quadriceps tendon. The quadriceps as a whole extends the leg via the patellar ligament, which attaches the apex of the patella to the tibial tuberosity. The patella protects the quadriceps tendon when kneeling and it acts as a lever, so the quadriceps tendon is moved farther from the center of the knee joint and can mechanically act through a greater arc to extend the leg against gravity and heavy weight bearing. The four parts of the quadriceps femoris are summarized in Table 22.1.
Table22.1
Muscle
Proximal attachment
Distal attachment
Notes
Rectus femoris
Anterior inferior iliac spine and body of ilium
Base of patella via quadriceps tendon
Name “rectus” implies it is “straight.” Only part of the quadriceps to cross the hip joint, so it also flexes the hip.
Vastus medialis
Linea aspera of femur
Quadriceps tendon and medial border of patella
Normal pull on the patella by the rectus femoris causes lateral deviation in patellar tracking.
Contraction of the vastus medialis thus stabilizes the patella and keeps it in proper alignment.
Vastus lateralis
Greater trochanter and linea aspera of femur
Quadriceps tendon and lateral border of patella
Largest member of the quadriceps, it forms the bulk of the lateral thigh. Partially hidden by the iliotibial tract.
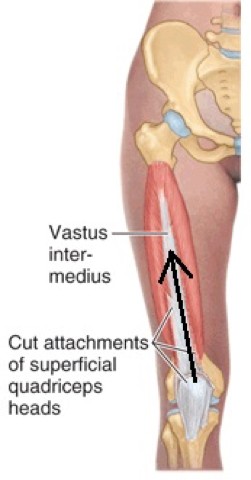
Vastus intermedius
From the anterior, lateral, and medial surfaces of the femoral shaft, extending around the femur in a semicircle when viewed in cross section
Base of patella via quadriceps tendon
Overlapped by the other parts of the quadriceps, so it is hidden from view, unless the rectus femoris is transected.
Action of the quadriceps femoris
The four heads of the quadriceps, acting through the quadriceps tendon, the patella, and the patellar ligament, extends the leg at the knee. The rectus femoris can also flex the thigh at the hip joint.
The quads are important for standing up from a sitting position, for squatting, for climbing stairs, for sprinting and jumping, and for stabilizing the knees in sports that require them to bend and stay bent—like skiing.
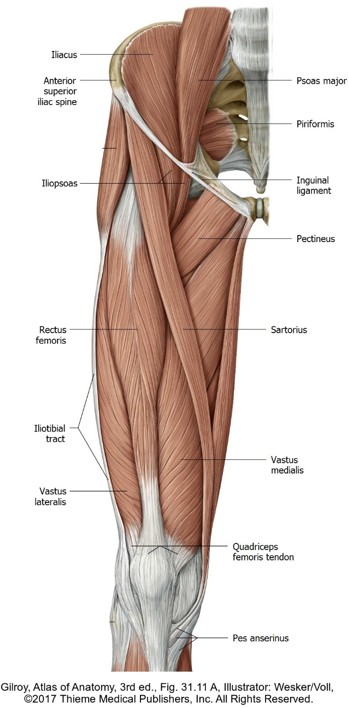
The ribbon-shaped sartorius is the longest muscle in the body. It arises (proximal attachment) from the anterior superior iliac spine and crosses the thigh obliquely, from lateral to medial, to insert (distal attachment) into the upper medial surface of the tibial shaft—medial to the tibial tuberosity.
Two other muscles, the gracilis and semitendinosus, insert nearby, thus forming a conjoined tendon where three muscles attach. This common tendon on the proximal tibia has a webbed appearance—apparently resembling the webbed foot of a fowl—so it has been dubbed the “pes anserinus” (goose’s foot). A bursa is between the muscle tendons of the pes and the tibia to prevent friction between tendons and bone. Inflammation of this anserine bursa (pes anserinus bursitis) is an overuse injury that can occur in runners.
Actions of Sartorius
The sartorius crosses both the hip and knee joints, so it can act on both = it weakly flexes both the hip and knee—it’s not a prime mover of either joint. It can also abduct and laterally rotate the thigh.
The claim to fame of the sartorius is that its contraction helps to cross one limb over the other (sit “cross-legged”). Old-fashioned tailors assumed this position when supporting a garment and sewing—so the sartorius is known as the “tailor’s muscle.” Indeed, the prefix sartus means “to mend”and the word “sartorial” refers to clothing; one who dresses well exhibits“sartorial splendor.” Those who like to hacky-sack also make good use of their sartorius.
Get to know the sartorius, because it is a useful landmark in the thigh: it forms the lateral boundary of the femoral triangle and is in the roof of the adductor canal.
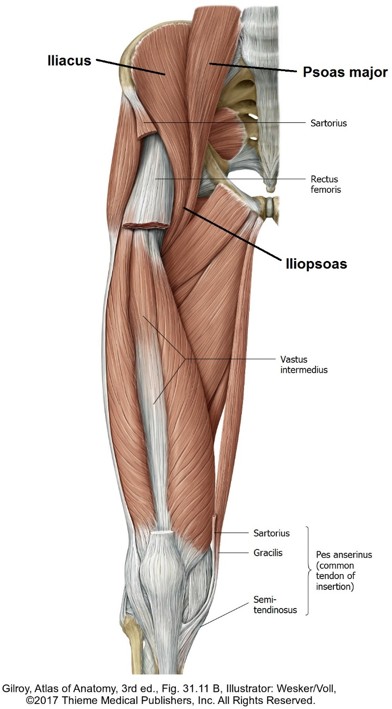
The iliopsoas is a composite muscle formed by union of the psoas major and iliacus muscles. Fusion of the muscles occurs between the inguinal ligament and the superior ramus of the pubis, in the subinguinal space. The tendon of iliopsoas inserts on the lesser trochanter of the femur.
The iliopsoas is the primary flexor of the thigh at the hip joint. It is also an important flexor of the trunk at the hip when the trunk is flexed against gravity (think about this when you do those crunches!).
The psoas major is innervated by ventral rami of L-1 to L-3 spinal nerves and the iliacus by branches of the femoral nerve.
Clinical correlation
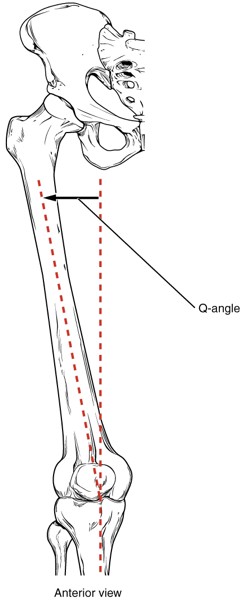
The line of force exerted by the quadriceps is lateral to the joint line, due to the pull on the patella by the strong rectus femoris and vastus lateralis. This tends to cause the patella to track laterally when the quads contract. The line of pull of the quadriceps relative to the patella is a clinical measure referred to as the Quadriceps angle or Q angle. It is larger in females than in males.
Contraction of the medial-most fibers of the vastus medialis (referred to as the vastus medialis obliquus) is important for counteracting the lateral tracking of the patella induced by the Q-angle. Weakness in the vastus medialis may lead to patellar tracking problems and predispose the patient to inflammatory conditions (chondromalacia patellae) or even patellar dislocation. Yikes—sadly, Dr. Conley has experience with this.
Figure 22.2 OPENSTAX COLLEGE, ANATOMY & PHYSIOLOGY, CONNEXIONS WEB SITE, PUBLIC DOMAIN.
The femoral nerve is derived from the lumbar plexus and is formed by the ventral rami of L-2, L-3, and L-4 spinal nerves. The integrity of the femoral nerve can be evaluated by eliciting the knee-jerk reflex with a tap on the patellar ligament below the patella with a reflex hammer.
It passes into the thigh under the inguinal ligament. Once in the anterior compartment, the femoral nerve is in the femoral triangle,anterior to the iliopsoas muscle and lateral to the femoral artery.
The femoral nerve has a short course in the thigh, before dividing into numerous branches:
Muscular branches innervate the quadriceps femoris, sartorius, and pectineus (described with the muscles of the medial thigh compartment).
Cutaneous branches include the anterior cutaneous nerves of the thigh and the saphenous nerve, a long nerve which has no function in the thigh, but supplies skin of the medial leg and medial foot.
The continuation of the external iliac artery distal to the inguinal ligament. Its pulse can be located at the mid-inguinal point, half way between the pubic symphysis and the anterior superior iliac spine. Upon entering the femoral triangle in the proximal thigh, the femoral artery lies medial to the femoral nerve and lateral to the femoral vein. At the apex of the femoral triangle, the femoral artery enters and traverses the adductor canal, which transports the artery to the posterior thigh through a gap in the adductor magnus muscle. Once in the popliteal fossa, the vessel changes its name to the popliteal artery.
The largest branch of the femoral artery, it is the chief source of blood to the thigh muscles. It branches from the posterior side of the femoral artery in the femoral triangle and curves around the femur into the posterior compartment of the thigh.
The deep artery of the thigh gives off the lateral and medial circumflex femoral arteries. These form a circular anastomosis around the trochanters of the femur. The medial circumflex femoral artery is the primary source of blood to the femoral neck and head in the hip joint. Damage to the artery can lead to avascular necrosis of the femoral head.
The proximal continuation of the popliteal vein after the latter emerges from the adductor canal. The femoral vein passes through the femoral triangle medial to the femoral artery. Within the triangle, the femoral vein receives blood from the deep vein of the thigh (profunda femoris vein) and from the great saphenous vein. At the base of the femoral triangle, the femoral vein passes deep to the inguinal ligament to become the external iliac vein in the abdominopelvic cavity. Adios femoral vein!
The largest superficial vein in the lower limb and the longest vein in the body. From Greek, it translates to “visible,” presumably because it is readily seen by the naked eye, especially when it has varicosities. It arises from the venous plexus on the dorsum of the foot and ascends along the medial leg and thigh within the superficial fascia. It enters the femoral vein (a deep vein in the thigh) through a hole in the fascia lata (deep fascia of the thigh), within the femoral triangle.
Clinical correlation
The great saphenous vein is commonly harvested and segments of it used as vessels for coronary artery bypass graft (CABG) procedures, to bypass stenotic or blocked arteries and revascularize areas of myocardium not receiving adequate blood supply.
Femoral triangle
We briefly encountered the femoral triangle earlier in our discussion of the inguinal region. It is located in the proximal part of the anterior thigh compartment. The triangle is upside-down with its base located adjacent to the inguinal region and its lateral borders formed by muscles.
Base: Inguinal ligament
Lateral border: Sartorius muscle
Medial border: Adductor longus muscle
Apex: Intersection of sartorius and adductor longus muscles
Floor: Iliopsoas and pectineus muscles
Roof: Fascia lata (deep fascia of thigh)—the saphenous opening (hole in the fascia lata for the great saphenous vein) is in the roof of the triangle.
Contents of the femoral triangle
Femoral nerve, femoral artery, and femoral vein, lined up lateral to medial along the base of the triangle. The femoral artery and vein are contained within the femoral sheath, a diverticulum of transversalis fascia extending out from the abdominal cavity under the inguinal ligament.
Deep artery and vein of the thigh (profunda femoris artery and vein).
Medial and lateral circumflex femoral arteries and veins.
Inguinal lymph nodes (superficial nodes are outside the fascia lata; deep nodes are deep to it).
The lateral cutaneous nerve of the thigh briefly enters the upper lateral corner of the triangle.
Subinguinal space
The space behind the inguinal ligament provides a corridor for structures passing between the abdominopelvic cavity and thigh.
there is loose connective tissue, lymphatic vessels, and a few deep inguinal lymph nodes. This part of the subinguinal space is known as the femoral canal. It is a potential space into which the femoral vein can expand when there is increased venous return from the lower limb, or if venous return is slowed above (as in a Valsalva maneuver), and the vein backfills.
is the sharp, concave edge of the lacunar ligament, formed by the reflection of inguinal ligament fibers onto the superior ramus of the pubic bone. Lacunar = from lacuna = “lake,” meaning a depression or pit, because the ligament is adjacent to the femoral canal.
Clinical correlation
The femoral canal is a weak spot into which abdominal contents could herniate. Femoral hernias are rare and more common in women than men, presumably because of their wider pelvic skeletons. Femoral hernias are associated with a higher risk of complications than inguinal hernias, because a herniated bowel could become strangulated on the sharp rigid edge of the lacunar ligament.
summary
The topographic arrangement of neurovascular structures within the subinguinal space (lateral to medial) can be remembered with this clever mnemonic: NAVEL
Femoral Nerve, Femoral Artery, Femoral Vein, and an Empty space with Lymphatics
Get to know the location of the femoral artery at the mid-inguinal point, just inferior to the inguinal ligament. The pulsations of the artery can be felt here. This is a pressure point to reduce blood flow to the lower limb in the case of hemorrhage. If you can locate the position of the femoral artery, you will know the femoral vein is just medial to it.
Cardiac catheterization procedures used to evaluate and treat heart conditions often use the femoral vessels as access routes to the heart. Central venous lines (central venous access) are often placed in the femoral vein.
Adductor canal (Hunter’s Canal)
Figure 22.7 NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 487.
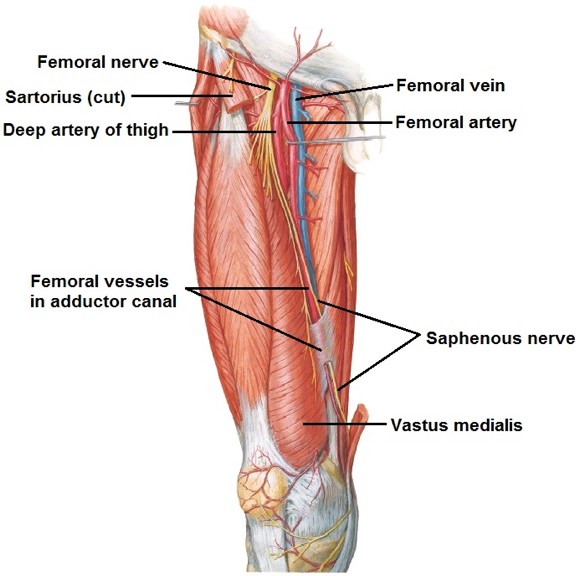
This is a narrow passageway (~15 cm long) located deep to the sartorius muscle, sandwiched between the vastus medialis and adductor muscles in the thigh. It transmits the femoral artery, femoral vein, and saphenous nerve (a cutaneous branch of the femoral nerve). The femoral vessels move from the anterior thigh to the popliteal fossa via the adductor canal. The saphenous nerve passes through the proximal part of the canal, but exits through its medial wall to become subcutaneous at the medial knee.
The adductor canal begins at the apex of the femoral triangle (where the sartorius crosses over the adductor longus) and ends posteriorly at the adductor hiatus, a gap in the tendon of the adductor magnus muscle just above its attachment to the medial condyle of the femur. Here the adductor canal empties into the popliteal fossa.
Medial compartment of the thigh
Muscles
All muscles of the medial compartment are innervated by the obturator nerve, with two exceptions, listed in Table 22.2.
Table 22.2
Muscle
Proximal attachment
Distal attachment
Actions
Notes
Pectineus
Superior ramus of pubis
Posterior femur proximal to linea aspera
Adducts and flexes thigh at hip
Located medial to the iliopsoas in the floor of the femoral triangle.
Innervated by the femoral nerve.
Gracilis
Body of pubis
Upper medial tibia via pes anserinus
Adducts thigh at hip; flexes leg at knee
Long, slender, “graceful” muscle. The most medial muscle in the compartment. The only muscle in the compartment that crosses two joints.
Adductor longus
Body of pubis
Linea aspera of femur
Adducts thigh at hip
The most anterior of the three adductor muscles. Forms medial boundary of femoral triangle.
Adductor brevis
Body and inferior ramus of pubis
Linea aspera of femur
Adducts thigh at hip
The “baby” of the adductor muscle family.
Adductor magnus: “Big Daddy” of the adductor family, has two parts
Adductor part (anterior part)
Inferior pubic ramus and ramus of ischium
Huge fan-like insertion along entire length of linea aspera
Adducts thigh at hip
Innervated by obturator nerve
Hamstrings part (posterior part)
Ischial tuberosity
Fibers are vertical; insert on the adductor tubercle on the medial condyle of the femur. Just above the adductor tubercle, the muscle contains a gap = the adductor hiatus, which is the distal opening of the adductor canal.
Extends thigh at hip
Receives its names because:
its action at the hip is similar to that of the hamstrings
it is located deep in the medial compartment, adjacent to the hamstrings
it is innervated by the tibial part of the sciatic, the same nerve that innervates the hamstrings.
Summary of muscles in the medial compartment
(Please study Table 22.2 for details of the muscles.)
With the exception of the hamstrings part of adductor magnus, all the muscles in the medial thigh run obliquely from medial to lateral = thus they produce adduction of the thigh.
Since most of the muscles of the medial thigh have their pubic attachments anterior to their femoral attachments, they produce weak hip flexion in addition to adduction.
The gracilis is the only muscle of the medial thigh to cross two joints; thus it acts at both the hip and knee.
All the muscles in the medial compartment are supplied by the obturator nerve, except for the pectineus (femoral nerve) and the hamstrings part of the adductor magnus (tibial part of the sciatic nerve).
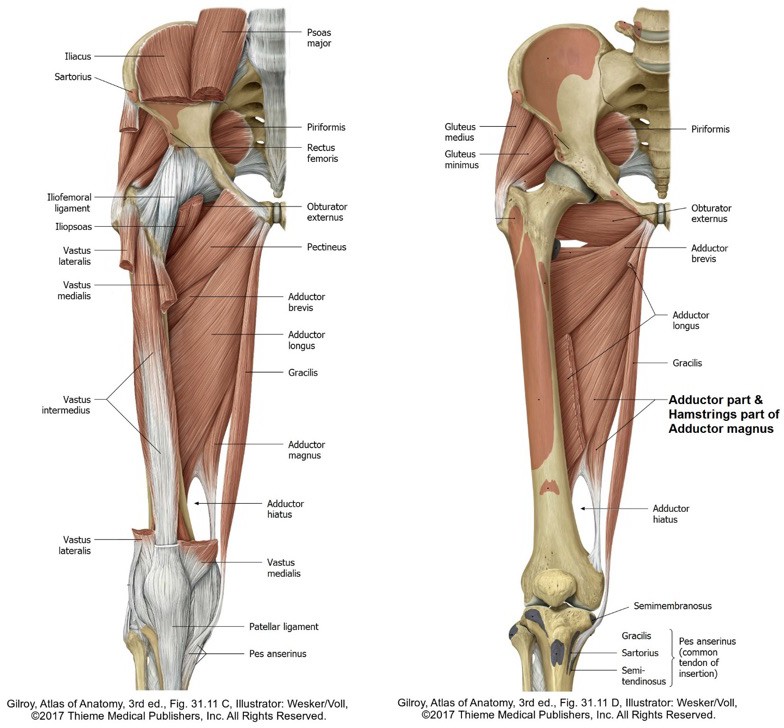
Figure 22.8 Muscles of the medial compartment: superficial (left) and deep (right) dissections.
Clinical correlation
A "groin pull" is a strain or tear of muscles in the medial compartment of the thigh. It is commonly found in athletes who participate in sports that require sudden forceful adduction of the thigh (e.g., soccer, hockey). They are graded in severity from 1st degree to 3rd degree, with 3rd degree being the most severe, involving complete tearing of the muscle. They are normally treated with ice, pressure, stretching, and strengthening regimens.
The obturator nerve supplies muscles in the medial compartment as well an area of skin on the medial thigh. We encountered this nerve earlier in the course: It is a branch of the lumbar plexus, formed from the ventral rami of L-2, L-3, and L-4 spinal nerves. It passes along the lateral pelvic wall and exits the pelvic cavity via the obturator canal. In the thigh, it divides into anterior and posterior branches; these are separated by the adductor brevis muscle. The anterior branch supplies the adductor brevis, adductor longus, and gracilis. The posterior branch takes care of the anterior part of the adductor magnus. The obturator nerve also sends sensory branches to the hip and knee joints.
Clinical correlation
Obturator nerve blocks are sometimes used to alleviate pain and muscle spasticity in young patients with cerebral palsy. Spasticity of the adductor muscles may cause the thighs and knees to bang together, or cross one another in a scissor-like fashion ("scissor gait"). This can impact hip joint growth and development. To affect all the adductor muscles, the nerve block must be done above the division point of the obturator nerve into its anterior and posterior branches, or each branch must be individually blocked. Knowledge of the regional anatomy is important here.
Blood supply
The chief source of blood to the medial compartment (heck, to ALL thigh compartments) is the deep artery of the thigh (profunda femoris). The obturator artery supplies some blood to the thigh and hip joint—but it mainly supplies pelvic structures.