PhD · Clinical Assistant Professor, Department of Translational Medicine & Physiology
Office: PBS 41C
Table of Contents
What is peritoneum?
Figure 1. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.1.Peritoneum is a serous membrane. Recall that serous membranes are associated with body cavities and visceral organs within them.
Question
What is the function of a serous membrane? What are the names of the two other serous membranes we encountered earlier in our course?
Parietal peritoneum lines the walls of the abdominopelvic cavity— part of the body cavity inferior to the diaphragm.
Visceral peritoneum is applied to the outer walls of many organs in the abdominopelvic cavity (e.g., stomach, intestines), much the same way that the visceral pleura forms the outermost layer of the lungs themselves.
The parietal and visceral peritoneum are a continuous layer that form the peritoneal sac. The potential space between the two layers is the peritoneal cavity—normally it contains only a thin layer of serous fluid, for lubrication purposes.
The development and subsequent arrangement of abdominal organs in the abdominopelvic cavity causes the peritoneal sac to be much more complex than the simple pleural and pericardial sacs we studied earlier—yet their basic plans are the same.
Innervation and blood supply of the peritoneum
Figure 2. Nerve supply/dermatomes of abdominal wall—these supply the parietal peritoneum. GRAY’S ANATOMY FOR STUDENTS, FIG. 4.38.
The parietal peritoneum receives blood and innervation from the same vessels and nerves that supply the body wall adjacent to it. Blood supply is via the posterior intercostal, lumbar, and epigastric (superior and inferior) arteries. The nerves supplying the parietal peritoneum are derived from the ventral rami of spinal nerves T-6 to L-1. T-12 is the subcostal nerve and the nerves derived from L-1 are the iliohypogastric and ilioinguinal nerves. Since it is supplied by somatic nerves, pain from the parietal peritoneum is usually well localized.
The visceral peritoneum receives blood and innervation from vessels and nerves associated with the organs it invests. Sensory information (stretch and irritation) is transmitted to the spinal cord along visceral afferent neurons. Pain is dull and diffuse and poorly localized—it is often referred to the dermatomes associated with the dorsal root ganglia that contain the cell bodies of the neurons. For example, pain from peritoneum associated with the stomach (a foregut organ—more on this later) is usually referred to the epigastric region of the abdominal wall (T-6 to T-9 dermatomes).
Mesenteries and peritoneal ligaments
Figure 3. GILROY, ATLAS OF ANATOMY, 3RD ED., FIG. 14.1B.
A mesentery is a double layer of peritoneum (with adipose tissue sandwiched between) that attaches organs to the body wall. Visceral peritoneum becomes continuous with parietal peritoneum in mesenteries. Mesenteries support organs and provide a conduit for nerves and vessels to reach organs from the body wall. Mesenteries also allow certain organs to have some mobility, for example, when the organ undergoes muscular contractions (peristalsis).
Omenta (singular = omentum) and peritoneal ligaments are also double-layered peritoneal structures that connect organs to the abdominal wall and to one another. Omenta are structures only associated with the stomach.
Development of the peritoneal cavity and mesenteries
Figure 4. THE DEVELOPING HUMAN, FIGURE 8-4.
As described earlier (Week 4 of human development), folding of the embryonic disc created a “tube-within-a-tube” body design. The inner tube is the primitive gut tube, composed of endoderm and splanchnic mesoderm. Three regions of the primitive gut tube are recognized. From cranial to caudal these are the foregut, midgut, and hindgut. More details are given later during your digestive system block.
Folding of the embryo also creates the definitive arrangement of the horseshoe-shaped intraembryonic coelom (future body cavity and serous sacs). The caudal limbs of the coelom extend below the diaphragm as left and right coelomic ducts. The peritoneal cavity arises from the coelomic ducts.
Lateral folding of the embryonic disc brings together the coelomic ducts and wraps them around the primitive gut tube, giving rise to the peritoneal cavity. The ducts are separated from one another dorsal to the gut tube by a partition of splanchnic mesoderm called the dorsal mesentery.
Ventral to the gut tube, in the region of the midgut and hindgut, the two coelomic ducts fuse, so in these regions the peritoneal cavity is shaped like the letter U in cross-section (see Figure 17.5).
Splanchnic mesoderm gives rise to visceral peritoneum; parietal peritoneum is derived from somatic mesoderm. This is the basis for the innervation of these tissues.
Figure 5. Midgut and hindgut = Dorsal mesentery only.
Figure 6. Foregut = Dorsal and ventral mesentery. THE DEVELOPING HUMAN, 10TH ED
In the region of the foregut, where the stomach and liver develop, the coelomic ductsventralto the gut tube do not fuse. Instead aventral mesenteryconnects the abdominal foregut to the ventral body wall. As the liver develops it will partition the ventral mesentery into two parts: one connecting the stomach to the liver and the other attaching the liver to the ventral body wall.
Elongation and rotation of the digestive tube in the abdomen during development destroys the simple arrangement of gut tube connected to the dorsal body wall by a dorsal mesentery. The result is that only some abdominal organs in the adult are suspended from the body wall by mesenteries = intraperitoneal. Others become fused to the dorsal body wall as their dorsal mesentery is obliterated = secondarily retroperitoneal.
Figure 7. Intraperitoneal (left) and retroperitoneal (right) organs. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.52.
Intraperitoneal organs
Retroperitoneal organs
In the adult, organs that have mesenteries are surrounded by visceral peritoneum, except for the area where the stalk of the mesentery joins the organ. These organs are said to be intraperitoneal. Note that this doesn’t mean they are within the peritoneal cavity—they aren’t—they project into the peritoneal cavity and are invested by visceral peritoneum, so they are technically outside the peritoneal sac (remember that the peritoneal cavity is the potential space between parietal and visceral layers of peritoneum).
Some non-digestive organs in the AP cavity originally develop in the posterior body wall and are dorsal to the peritoneal sac. These organs are said to be retroperitoneal. The terms “subperitoneal” and “extraperitoneal” are sometimes used. The kidneys and suprarenal glands are examples. Clinicians and anatomists often say these organs are in the “retroperitoneum.”
Certain parts of the gut tube that were once intraperitoneal (suspended by the dorsal mesentery) later lose their mesentery as they become fused to the body wall during development. These organs only have peritoneum on their anterior and lateral surfaces. Although they resemble other retroperitoneal organs, they are classified as secondarily retroperitoneal, since they once had a mesentery.
The obliteration of the mesentery dorsal to the organ (pictured in Figure 7) produces what is called fusion fascia, a tissue plane between organ and body wall. Surgeons mobilize secondarily retroperitoneal organs by incising peritoneum adjacent to the organ and then dissecting along the fusion fascia plane.
Figure 8. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-3.
Survey of the peritoneal cavity
The peritoneal cavity has two subdivisions called the greater and lesser sacs.
Greater sac
The greater sac makes up most of the peritoneal cavity. It extends from the diaphragm to the pelvic cavity. It is anterior to the stomach and liver and surrounds the intestines and spleen.
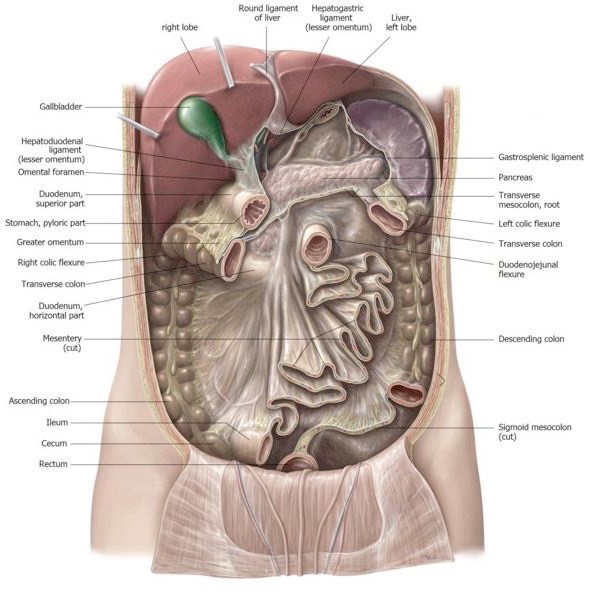
Figure 9. Abdominal wall opened to show the greater sac. GILROY, ATLAS OF ANATOMY, 3RD ED., FIG. 14.3A.
Lesser sac
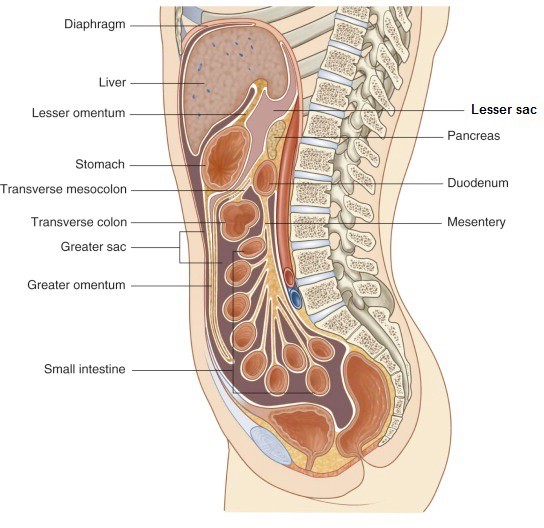
The lesser sac (also called the omental bursa) is a narrow space posterior to the stomach. It is connected on the right side to the greater sac by a passageway called the omental foramen. The lesser sac is a cul-de-sac . . . the only way in and out is via the omental foramen.
Figure 10. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.53.
For ease of study, some anatomists divide the peritoneal cavity into three regions:
supracolic
infracolic
pelvic regions.
The supracolic and infracolic regions are separated by the transverse colon. The pelvic region is below the pelvic brim, within the pelvic cavity.
Supracolic region
The supracolic region contains the liver, gallbladder, and stomach, as well as the lesser sac.
Infracolic region
The infracolic region is defined by the box-shaped colon (ascending, transverse, and descending). It is filled mainly by coils of small intestine.
Pelvic region
The pelvic region is also filled with loops of small intestine. In the female, the uterus, ovaries, and Fallopian tubes are related to the pelvic part of the greater sac.
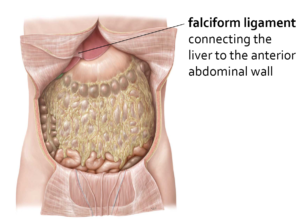
A double layer of peritoneum that spans from the liver to the midline of the internal ventral body wall. It is part of the ventral mesentery of the foregut. The inferior free margin of the falciform ligament is curved(concave), thus its name (falciform = “sickle-shaped”).
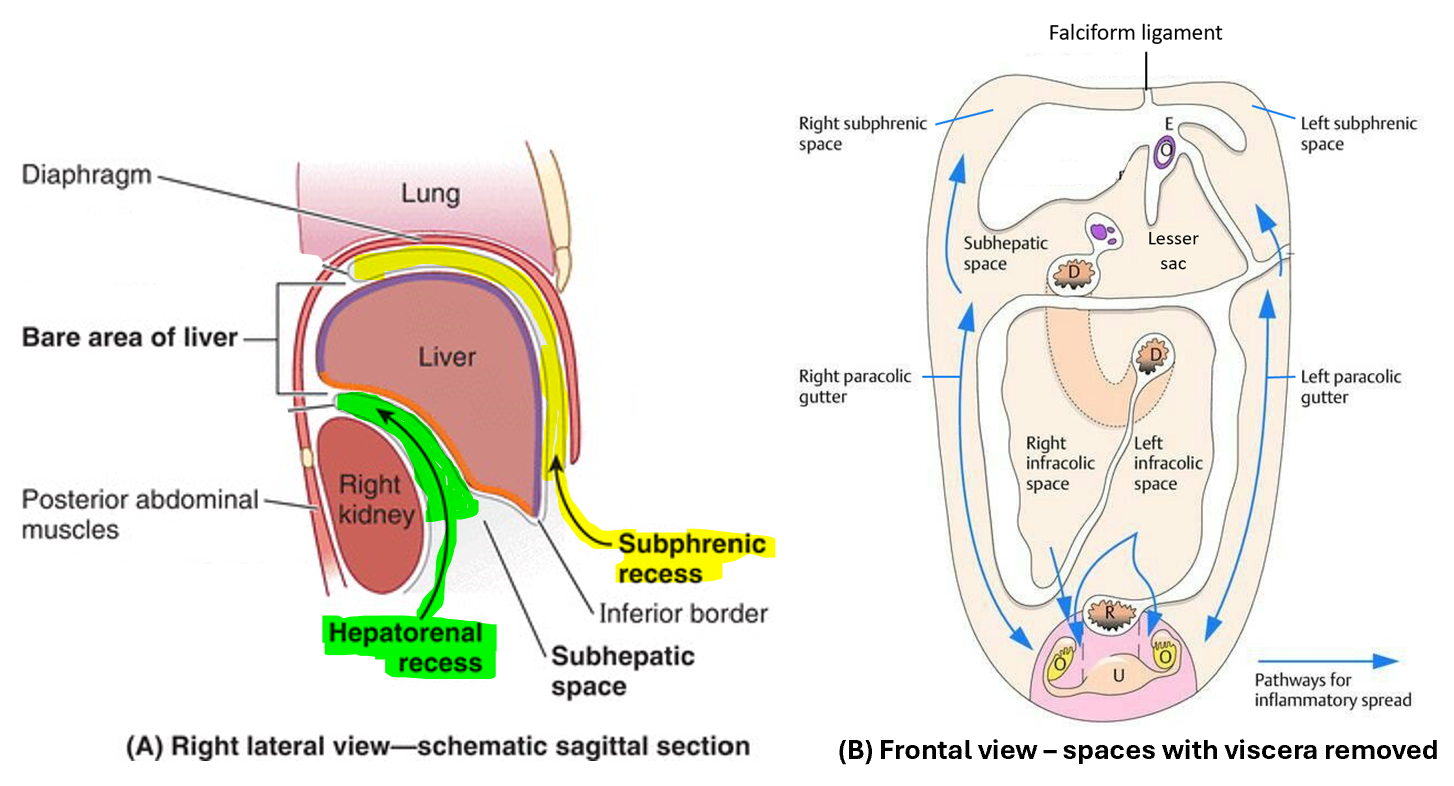
The falciform ligament divides the peritoneal cavity in the region of the liver and diaphragm into left and right portions. Tracing each of these portions superiorly leads into narrow spaces between the liver and diaphragm. These are the left and right subphrenic recesses.
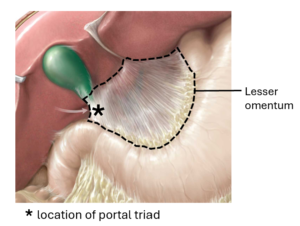
This double layer of peritoneum connects the inferior surface of the liver to the lesser curvature of the stomach and first part of the duodenum. It has anterior and posterior layers. The lesser omentum, like the falciform ligament, is part of the ventral mesentery of the foregut. Due to rotation of the stomach during development, both the stomach and the lesser omentum are positioned vertically in a coronal plane.
Figure 12. GILROY, ATLAS OF ANATOMY.
The lesser omentum has a free vertical border on the right; enclosed within this border (between the two layers of peritoneum) is the portal triad (common bile duct, hepatic artery proper, and hepatic portal vein).
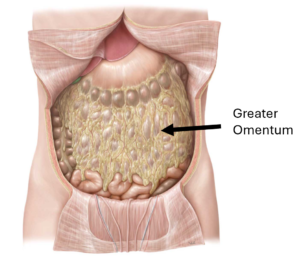
The greater omentum is a large, fatty peritoneal structure that hangs from the greater curvature of the stomach and first part of the duodenum. Like the lesser omentum, much of it is oriented in a coronal plane. The greater omentum is the dorsal mesentery of the stomach—this will be difficult for students to appreciate without knowledge of stomach development (covered with the digestive system)—but if traced posteriorly, the greater omentum does attach to the posterior abdominal wall. In addition to support and fat storage functions, it has been shown that the greater omentum contains lymphoid tissue and thus may be involved in immune functions. Also, it is mobile and has been known to move and surround areas of inflammation within the abdomen, presumably to prevent the spread of infection and promote healing. This may be how it earned its nickname “the abdominal policeman” (bestowed by a British surgeon in 1906).
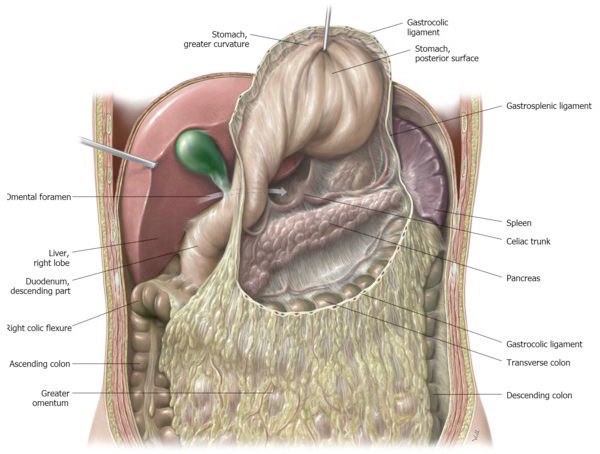
Figure 14. Greater omentum transected and stomach elevated to show lesser sac. GILROY, ATLAS OF ANATOMY, 3RD ED.
This space (normally filled with a small amount of serous fluid) is the part of the peritoneal cavity posterior to the stomach and lesser omentum. Thus, the posterior wall of the stomach faces into the lesser sac. Behind the lesser sac are the abdominal aorta and pancreas, both of which are retroperitoneal (= behind the peritoneum).
The lesser sac and greater sac communicate through a narrow opening posterior to the edge of the lesser omentum called the omental foramen (foramen of Winslow). With a finger placed in the omental foramen, the structures of the portal triad can be palpated anteriorly, while posterior to the omental foramen is the inferior vena cava, behind the peritoneum.
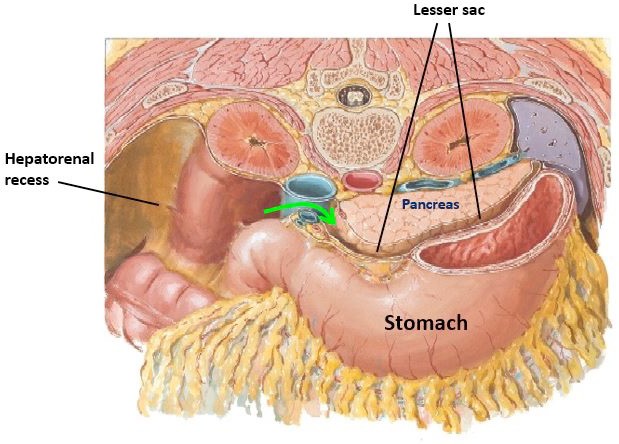
Figure 15. Transverse section showing lesser sac between stomach and pancreas. Green arrow indicates omental foramen. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 267.
This is the part of the greater sac on the right side into which the omental foramen opens. It is bordered anteriorly by the right lobe of the liver and gallbladder and posteriorly by the anterior surface of the right kidney (packed in fat and behind the peritoneum). The right colic (hepatic) flexure is inferior. The hepatorenal recess communicates with the right paracolic gutter (described later). Thus, it is possible for pus or fluid from the lesser sac to leak through the omental foramen into the hepatorenal recess, then slide down the right paracolic gutter into the pelvic cavity.
Clinical correlation
Although rare, an ulcer in the posterior wall of the stomach (peptic ulcer), if large enough, could perforate the stomach wall, causing gastric contents to enter the lesser sac behind the stomach. An abscess in the lesser sac could result. If pus and gastric contents pass out of the omental foramen, a more generalized peritonitis might occur.
Clinical correlation
The hepatorenal recess is the most posterior part of the greater sac. Therefore, abnormal contents in the peritoneal cavity often accumulate in the hepatorenal recess when the patient is supine (lying on their back). Since it is normally a potential space (as are all the parts of the peritoneal cavity), demonstration of the hepatorenal recess with imaging studies (like ultrasound) is an indication of pathology (e.g., ascites or hemoperitoneum occupying the space).
Infracolic region: Spaces and mesenteries
The infracolic region or compartment is bordered above by the transverse colon and its mesentery (transverse mesocolon) and laterally by the ascending and descending colons. It is filled with coils of the small intestine (jejeunum and ileum).
Parts of the greater sac, these are vertical grooves formed where the visceral peritoneum reflects from the lateral surfaces of the ascending and descending colons to become parietal peritoneum on the ventral body wall. The right gutter communicates above with the hepatorenal recess. Both gutters communicate below with the pelvic portion of the greater sac.
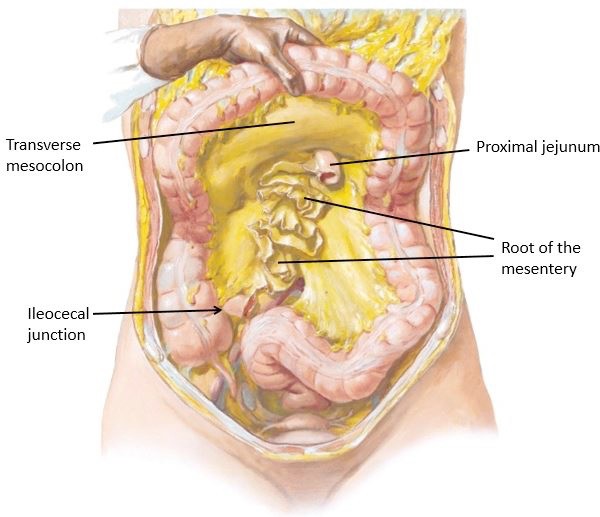
Figure 16. Transverse colon elevated; mesentery of the small intestine transected with small intestine removed. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 265.
This is the mesentery of the transverse colon. It attaches to the posterior abdominal wall horizontally across the lower pancreas and the second (descending) part of the duodenum on the right. It ends on the left at the left colic (splenic) flexure and on the right at the right colic (hepatic) flexure. The middle colic vessels reach the transverse colon through the transverse mesocolon.
The convoluted portions of the small intestine, the jejunum and ileum, are supported by the mesentery (also called mesentery of the small intestine or mesentery proper). It stretches diagonally from left to right across the posterior abdominal wall, beginning above at the sharply-bent duodenojejunal junction and terminating below in the right lower quadrant at the ileocecal junction.Between these two points, the mesentery is described as “fan-shaped and fluted”—the surface area where the mesentery attaches to the intestine is said to be 40 times larger than the footprint it produces where attached to the posterior body wall (Hollinshead’s Textbook of Anatomy, 5th ed.). The mesentery supports the jejunum and ileum and its many intestinal blood vessels, lymphatic vessels, and nerves.
The cecum is an odd structure. It is the first part of the large intestine, continuous above with the ascending colon. Unlike the ascending colon, the cecum is a blind pouch and is not secondarily retroperitoneal. It is surrounded by visceral peritoneum and since it is not fixed to the body wall is somewhat mobile.
Behind the cecum is an area of the greater sac known as the retrocecal recess. Clinically, this space often contains the appendix. The root of the appendix is attached to the cecum and the lumen of the appendix communicates with the cecal cavity. The rest of the appendix is mobile; the location of the tip is variable. A 2015 paper reported of the 377 cadaveric cases studied, 44% of appendices were tucked up into the retrocecal recess—the most common site in the study. By the way, the appendix has a small mesentery—the meso-appendix. It supports the appendicular vessels.
Figure 17. GILROY, ATLAS OF HUMAN ANATOMY, 3RD ED., FIGURE 14.7.
Supports the portion of the large intestine distal to the descending colon, the sigmoid colon, and its vessels and nerves. Apparently, ancient anatomists thought the sinuous profile of this part of the large bowel resembled the Greek letter sigma ∑. The attachment of the sigmoid mesocolon to the posterior body wall really resembles an inverted V—it stretches from the left iliac fossa, across the left iliac vessels, and down over the sacrum in the posterior pelvic wall.
Figure 18. Summary: Spaces/recesses of the peritoneal cavity.
Pelvic portion of the greater sac
Figure 19. Peritoneal pouches in female pelvis. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 340.
The abdominal and pelvic cavities are continuous (abdominopelvic cavity = a single cavity) at the pelvic brim. Peritoneum from the abdomen continues inferiorly from the infracolic region into the pelvic cavity. As it passes from the anterior abdominal wall backwards, it drapes over the bladder and rectum in the pelvic cavity.
Phenotypical male
In the absence of a uterus, a peritoneal recess is created between the bladder and rectum: the rectovesical pouch.
Phenotypical female
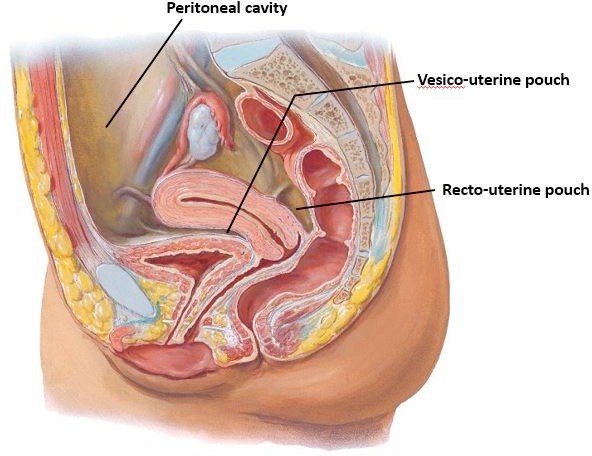
When present, the uterus and fallopian tubes cause a transverse fold of peritoneum to be raised up over these organs, extending to the lateral pelvic wall. This is the broad ligament, a double layer of peritoneum similar to a mesentery. The ridge of peritoneum created by the broad ligament and uterus within the pelvis creates two peritoneal recesses between organs: the vesico-uterine pouch between bladder and uterus, and the deeper recto-uterine pouch (pouch of Douglas) posteriorly between rectum and uterus. These pouches are parts of the greater sac.
Clinical correlation
The rectovesical and recto-uterine pouches are the inferior-most extensions of the peritoneal cavity in the two sexes. They normally contain loops of small intestine and a small amount of serous fluid. Under pathological conditions, fluids can accumulate in the pouches when the individual is upright (e.g., ascitic fluid, hemoperitoneum, abscesses). In females, an ectopic pregnancy can rupture and bleed into the recto-uterine pouch.



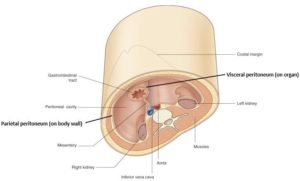
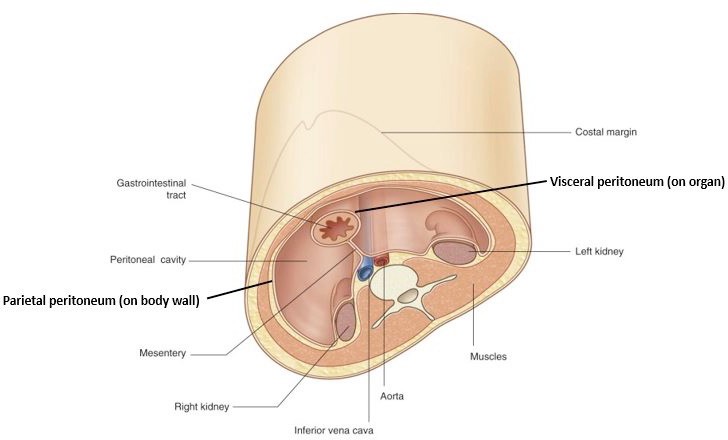
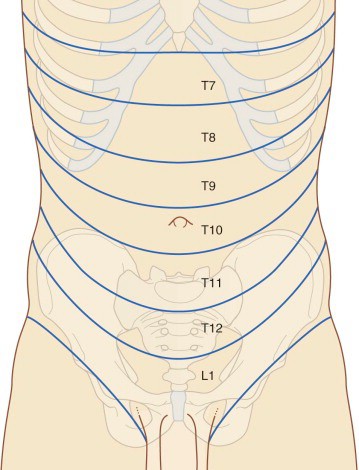
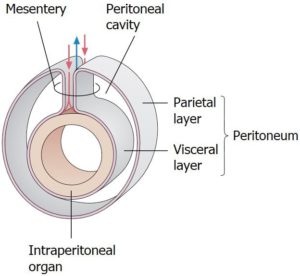
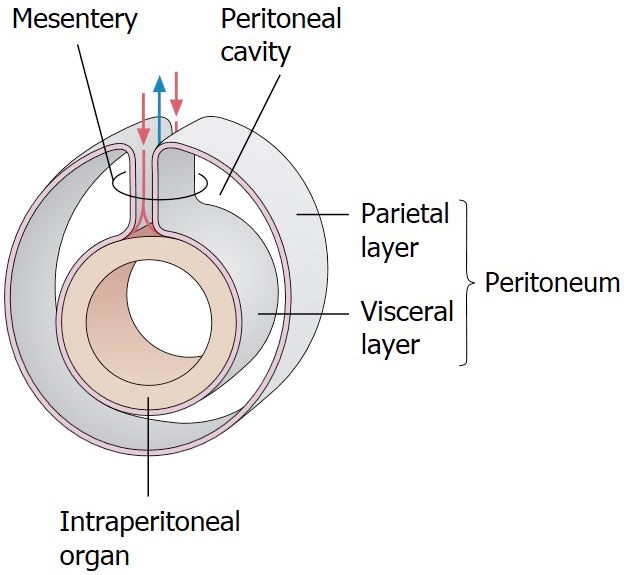
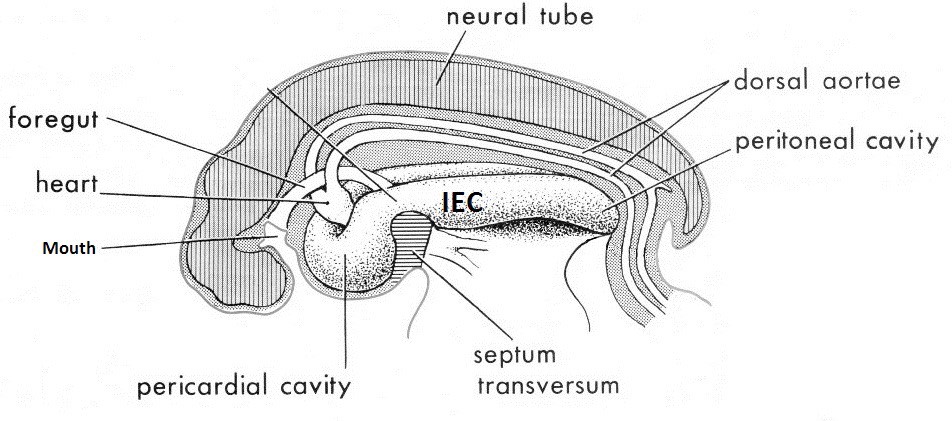
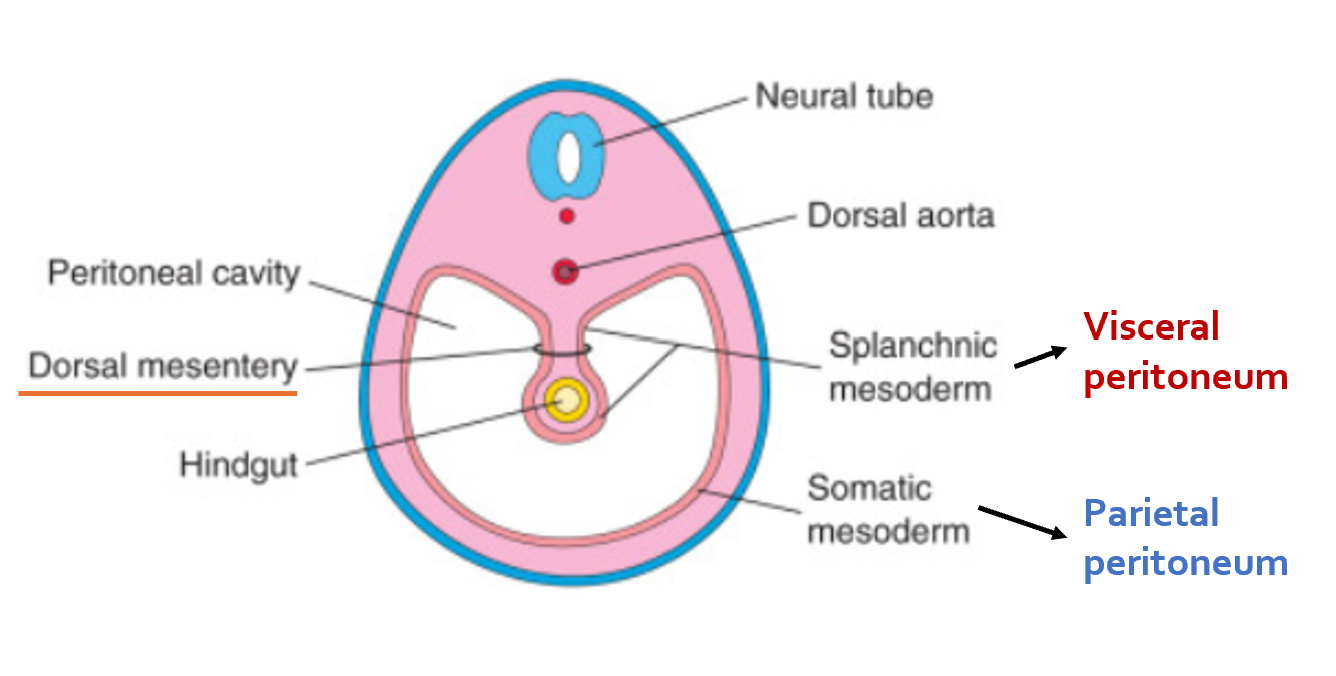
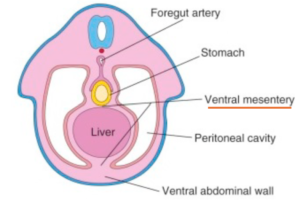
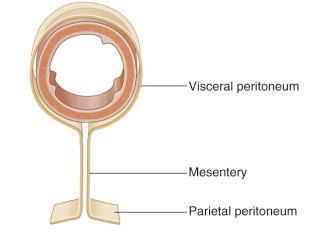
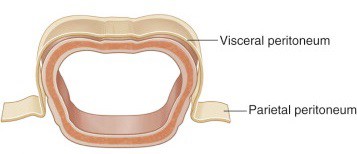
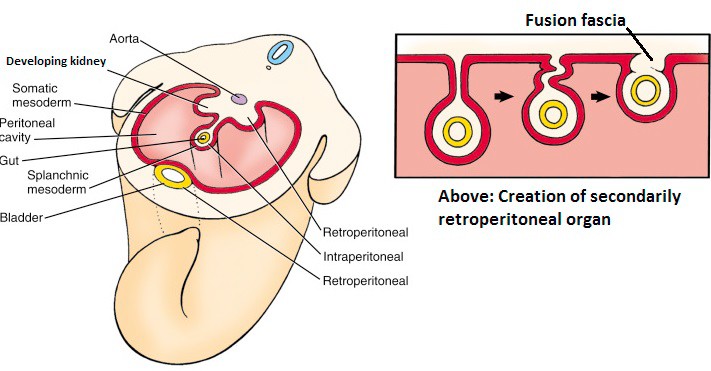
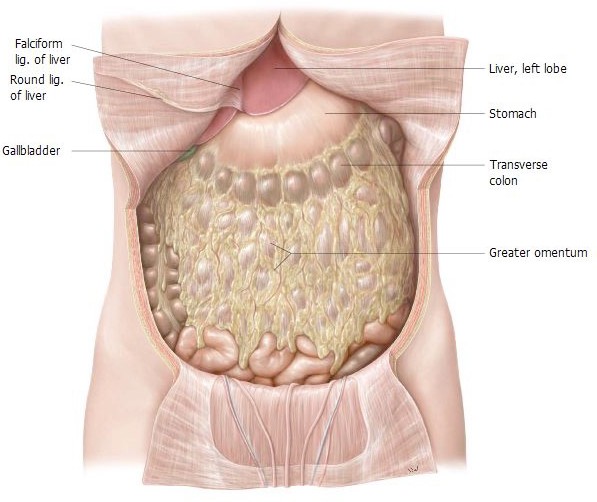 Figure 9. Abdominal wall opened to show the greater sac. GILROY, ATLAS OF ANATOMY, 3RD ED., FIG. 14.3A.
Figure 9. Abdominal wall opened to show the greater sac. GILROY, ATLAS OF ANATOMY, 3RD ED., FIG. 14.3A.