The hand is crucial to daily living—from sensing our environment to getting food to our mouths. It is very complex in a biomechanical sense, with 19 bones (not including the 8 carpal bones), 19 joints, and 29 (intrinsic and extrinsic) muscles. This complexity permits basic actions such as swinging a bat, to very intricate movements (like dissecting or playing a cello!). Anything that disrupts the hand’s performance has disabling consequences for the person.
Knowing your hand anatomy and function thoroughly is crucial to understanding pathology, and ultimately restoration of normal operation of life.
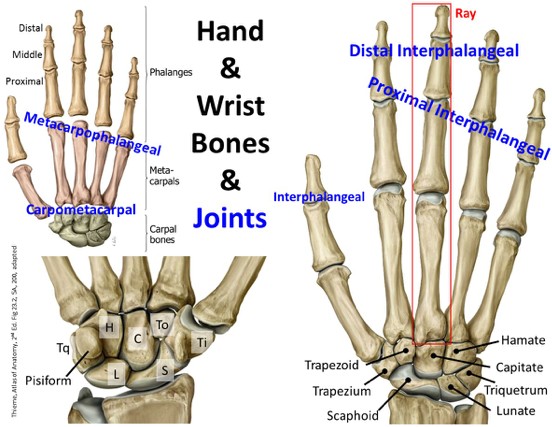
Bones of the wrist and hand
The bones of the hand can be divided into the wrist, or carpus, and the five rays. The term ray is used to describe one metacarpal bone and its associated phalanges. The wrist bones through phalanges were briefly listed in the forearm section; review them here before proceeding.
Figure 11.1
Carpus/Wrist
Hand
Metacarpals
Phalanges
Eight carpal bones arranged in proximal and distal rows of four
Proximal row from lateral to medial: Scaphoid, Lunate, Triquetrum, Pisiform
Distal row from lateral to medial: Trapezium, Trapezoid, Capitate, Hamate
Give flexibility to the wrist and the two rows glide on each other as do the individual bones
Articulate with the base of the metacarpals forming the carpometacarpal (CMC) joints
Hand bones arranged into rays: metacarpals and phalanges, #1 is thumb, #5 is pinky
Articulate with the distal row of carpal bones (CMC joint)
Form the skeleton of the palm
Base articulates with carpal bones, head articulates with phalanges; shaft joins the two
Dorsal aspect of the metacarpal bones forms the “knuckles” (surface anatomy feature)
Thumb: 2 phalanges (proximal and distal)
Digits 2–4: 3 phalanges (proximal, middle and distal)
Each has a base, a shaft, and a head.
Arthrology of the wrist and hand
Radiocarpal (wrist) joint
Hand joints
No articulation with ulna
Movement at the wrist joint consists of two degrees of freedom:
Flexion and extension
Abduction and adduction
Circumduction: Combination of these cardinal movements
Carpometacarpal (CMC) Synovial Joints
Thumb is a saddle: trapezium and base of 1st metacarpal, allows for angular movement in any plane, includingthe important opposition
Very little movement at 2nd and 3rd CMC, and some mobility about 4th and 5th that provide a slight cupping of thepalm (pad to pad opposition of the thumb and little finger) during a tight grasp
Metacarpophalangeal (MCP) joints
1st MCP only flexes and extends
2nd–5th: move in 2 planes: flexion-extension, and adduction-abduction
Interphalangeal joints
All synovial and only flex and extend.
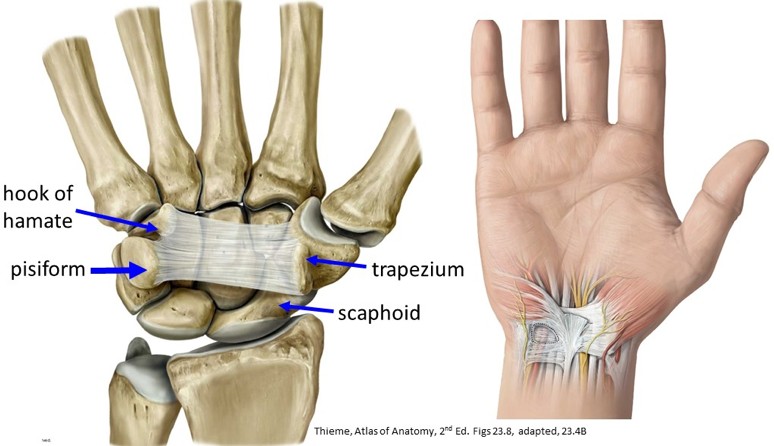
Carpal tunnel
Flexor retinaculum (transverse carpal ligament)
Strong band of fascia across the carpal bones
Fibro-osseous roof of carpal tunnel on volar/palmar side of carpals
Attachment for thenar and hypothenar muscles
Figure 11.2
Question
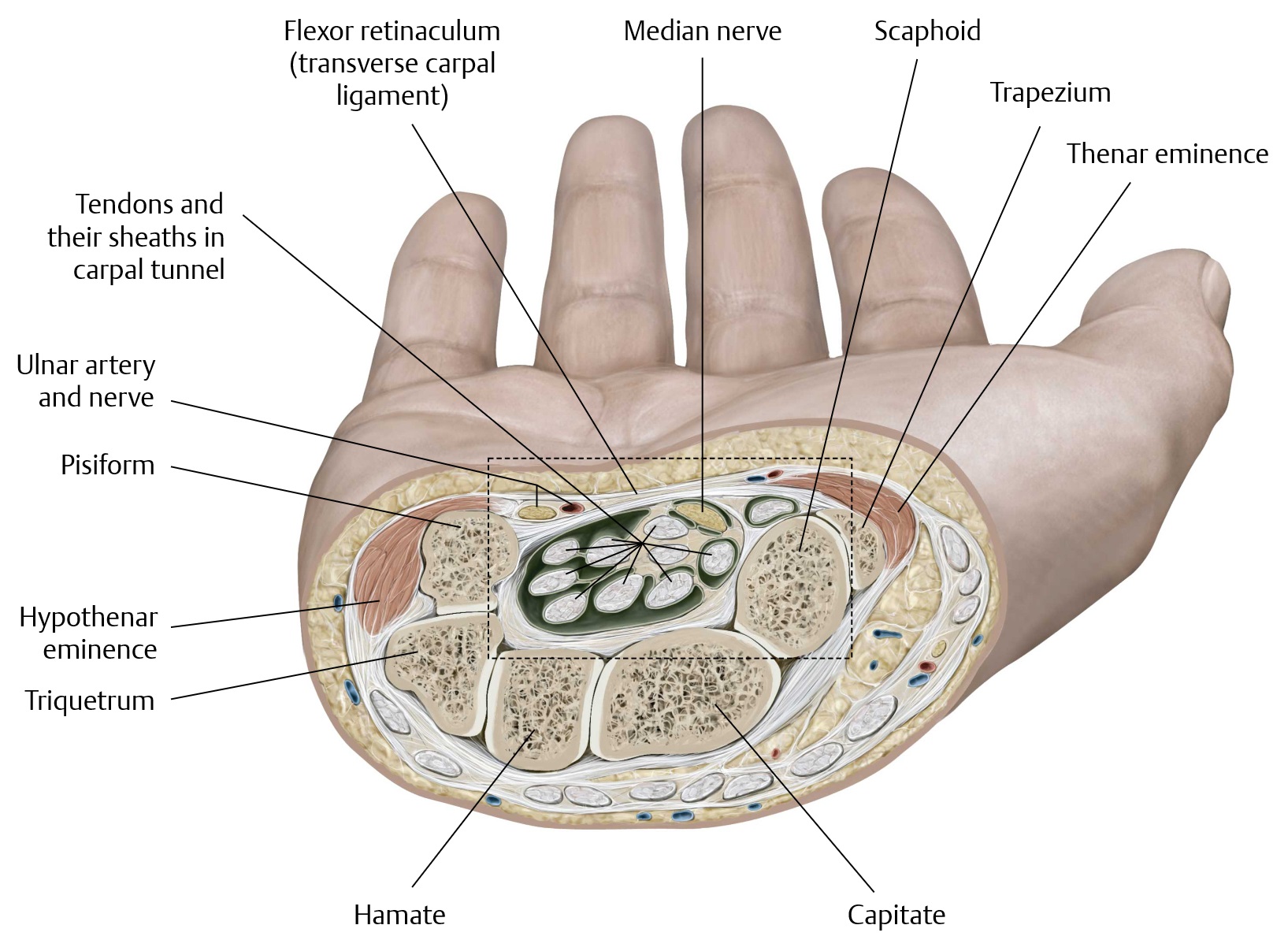
The carpal tunnel is a narrow space—yet it contains ten (10) structures! Can you name them? See Figure 11.3.
Wrist flexors (and extensors) usually attach to the proximal part of the metacarpals and do not course through the carpal tunnel. The flexor carpi radialis tendon appears to be in the carpal tunnel, but it is actually in a separate fibrous compartment and never travels within.
Figure 11.3 Carpal tunnel contents.
Clinical correlation: Carpal tunnel syndrome
Compressive neuropathy: Any process that increases pressure on the median nerve (swelling of tendons) may cause injury to it muscle weakness of the thumb, nocturnal symptoms, and/or tingling or numbness of the skin of the thumb and first two and one-half fingers.
+ Tinel sign: Lightly tap over the median nerve at the tunnel to elicit tingling in the dermatome.
Musculature of the hand
There are 20 intrinsic muscles of the hand: small, but essential to fine control of the digits. The intrinsic muscles of the hand can be group into the following categories (see Figures 11.4–11.9):
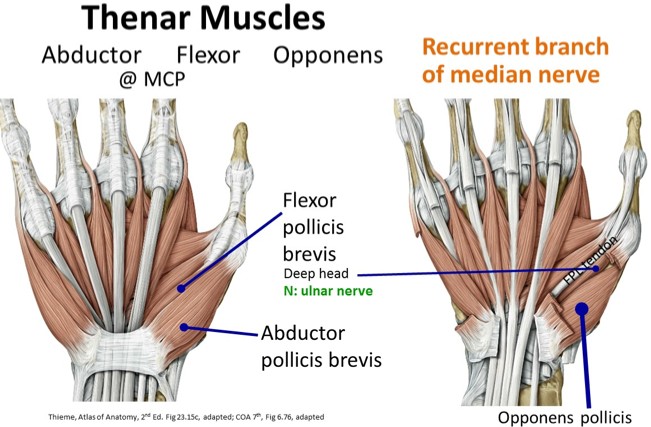
Thenar muscles
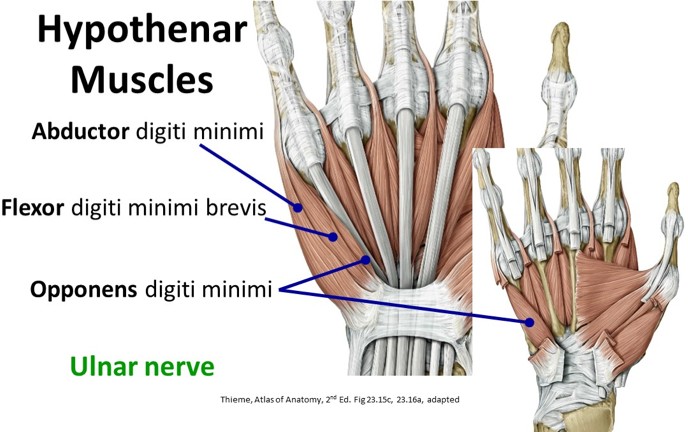
Hypothenar muscles
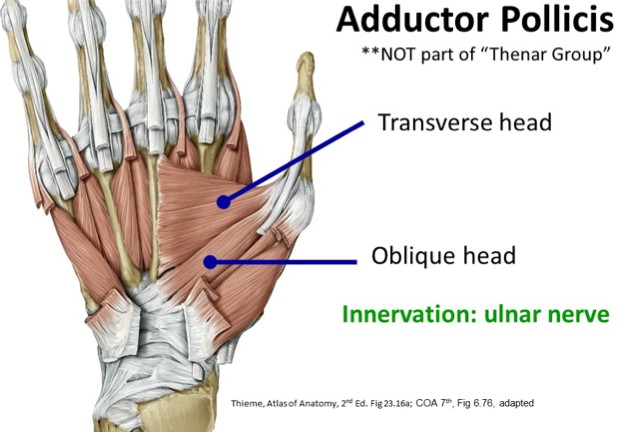
Central muscles (Adductor pollicis and Lumbricals)
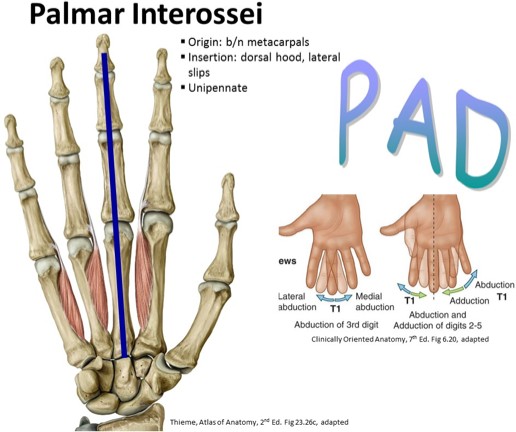
Interosseous muscles (Palmar and Dorsal)
Figure 11.4.
Figure 11.5.
Figure 11.6.
Figure 11.7.
Figure 11.8.
Figure 11.9.
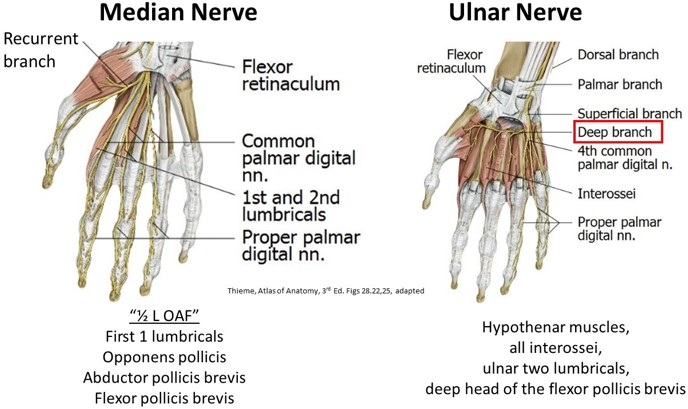
General scheme of innervation of the hand muscles
All of the hand muscles are supplied by the ulnar nerve, except the thenar group and the first two lumbricals (forefingerandlongfinger)whicharesuppliedbythe median nerve.
Recurrent branch of the median nerve: thenar muscles (OAF)
Digital nerves: motor branches innervate the first two lumbricals (1/2L)
Ulnar nerve: divides into a deep branch which supplies the hypothenar muscles, the interossei, the ulnar two lumbricals, and the deep head of the flexor pollicis brevis; and a superficial branch supplying the skin of the ulnar 1½ digits
Consult Tables 11.1–11.6. Only the important origins and insertions are listed.
O= origin, I = insertion, A= action, N= nerve
Table 11.1 Thenar muscles
Muscle
O
I
A
N
Abductor pollicis brevis
adduct thumb
recurrent branch of median nerve
Flexor pollicis brevis
flexes thumb
recurrent branch of median nerve ulnar nerve
Opponens pollicis
opposes thumb
recurrent branch of median nerve
Table 11.2 Hypothenar muscles
Muscle
O
I
A
N
Abductor digiti minimi
abducts 5th digit
ulnar nerve
Flexordigiti minimi brevis
flexes 5th proximal phalanx
ulnar nerve
Opponens digiti minimi
draws 5th metacarpal forward
ulnar nerve
Table 11.3 Central muscles of hand
Muscle
O
I
A
N
Adductor pollicis
adduct thumb
ulnar nerve
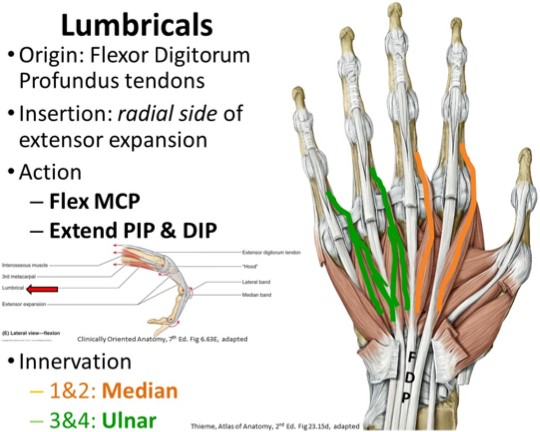
Lumbricals (4)
radial side FDP tendons 2–5
radial side, dorsal extensor expansion 2–5
flex MCP, extend PIP & DIP joints
1&2: Median nerve
3&4: Ulnar nerve
Table 11.4 Interosseous muscles
Muscle
O
I
A
N
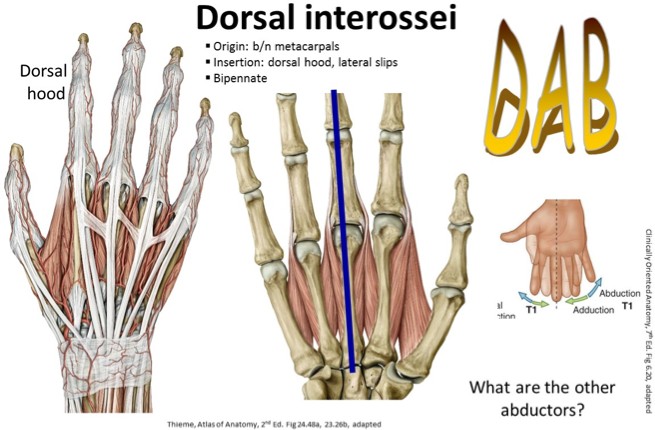
Dorsal interossei
adjacent sides of 2metacarpals
base proximal phalanx, extensor expansions 2–4
abduct digits 2–4; aid lumbricals
ulnar nerve
Palmar interossei
palmar surface metacarpals 2, 4, 5
base proximal phalanx, extensor expansions 2,4,
5
adduct digits 2, 4, 5; aid lumbricals
ulnar nerve
Actions at the hand joints
The movements of the hand are complex, and as such, the muscles can perform more than one function. The following tables are outlines of the cardinal movements of the thumb and fingers and list both the intrinsic and extrinsic muscles.
Movements of the 5th digit are listed in the hypothenar muscle table (Table 11.3) and are more straightforward.
Table 11.5 Digits 2–4 at the DIP, PIP, and MCP joints
Action
MCP Joint
PIP Joint
DIP Joint
Flexion
Lumbricals and interossei
Flexor digitorum superficialis (FDS)
Flexor digitorum profundus (FDP)
Extension
Extensor digitorum
(communis)
Lumbricals and interossei (central slip)
Lumbricals and interossei (terminal slip)
Abduction
Dorsal interossei
Adduction
Palmar interossei
Table 11.6 Thumb
Action
CMC Joint
MCP Joint
IP Joint
Flexion
Flexor pollicis brevis (FPB)
Flexor pollicis longus (FPL)
Extension
Extensor pollicis brevis (EPB)
Extensor pollicis longus (EPL)
Adduction
Adductor pollicis
Abduction
Abductor pollicis longus (APL)
Abductor pollicis brevis (APB)
Opposition
Opponens pollicis
Blood supply of the hand
The hand is in many positions, often applying pressure, and so requires many branched and anastomosing arteries.
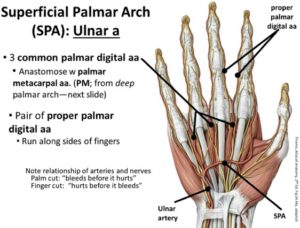
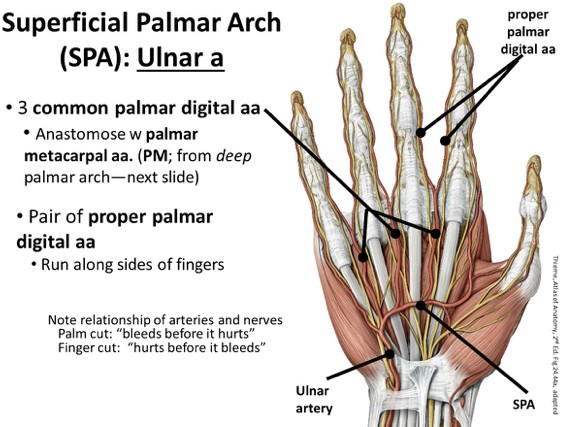
Ulnar artery
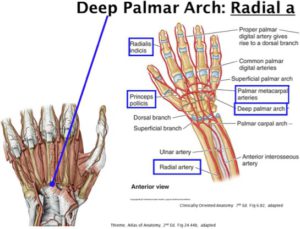
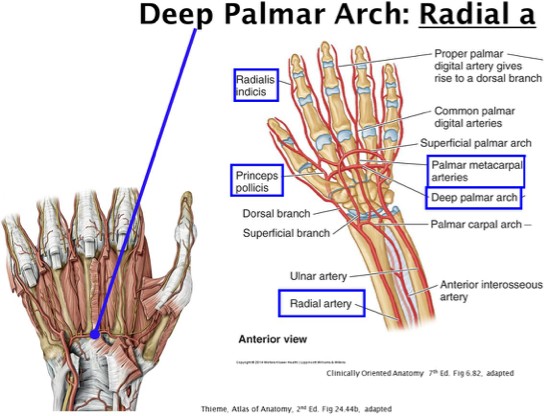
Radial artery
Dorsal venous arch
Figure 11.11
Enters the hand anterior to the flexor retinaculum between the pisiform and the hook of the hamate via the ulnar (Guyon’s) canal.
Lies lateral to the ulnar nerve and divides into two branches
Superficial palmar arch: gives off 3 common palmar digital arteries, which divide into a pair of proper palmar digital arteries (run along the sides of the 2–4 fingers)
Deep palmar branch: Joins the radial artery to complete the deep palmar arch—a second anastomosis in the hand between the radial and ulnar arteries. Palmar metacarpal arteries branch from the deep palmar arch, which anastomose with common palmar digital arteries.
Figure 11.12
Curves dorsally around scaphoid and trapezium, crosses the floor of the anatomical snuffbox
Anastomoses with deep palmar branch of the ulnar artery to form the deep palmar arch (mainly formed by the radial a.)
Runs across the metacarpals just distal to their bases
Across the dorsum of the hand where cephalic and basilic veins arise
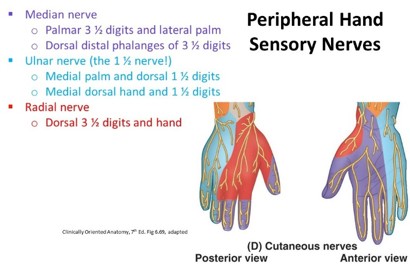
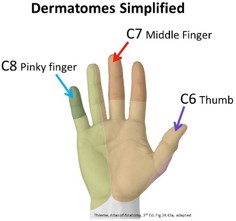
Hand cutaneous sensation
There are two ways to categorize the innervations of the skin of the hand—by the sensory branches of the peripheral nerves, or by dermatomes (segmental).
Note
Knowing both relationships can help you determine if it is a nerve injury or a nerve root injury (i.e., is a median nerve lesion, or is it a lesion at C6?).
Figure 11.13
Figure 11.14
Palmar aponeurosis
Figure 11.15
Very tough deep fascia just deep to the skin that overlies soft tissues and long flexor tendons
Proximal part: continuous with flexor retinaculum; palmaris longus tendon blends/inserts
4 longitudinal digital bands distally attach to bases of proximal phalanges; become continuous with fibrous digital sheaths (see Figure 11.15)
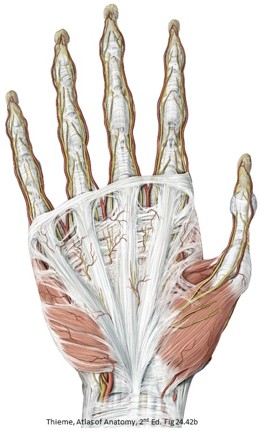
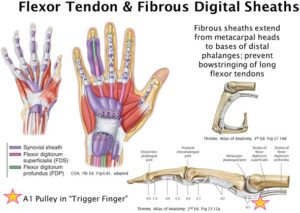
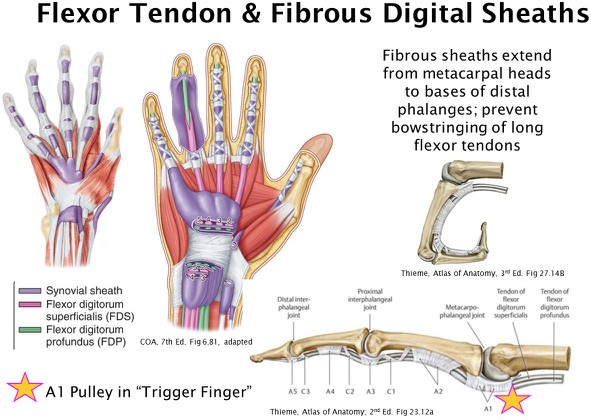
Flexor tendon sheaths
Figure 11.16
In the carpal tunnel and central hand, the FDS and FDP tendons are surrounded by synovial sheaths. These are serous membranes that secrete a lubricating fluid.
Allow the tendons to slide over each other during movement of the fingers
Near base of proximal phalanx: FDS tendon splits around the FDP tendon
FDP tendon attaches to base of distal phalanx; FDS tendon attaches to base of middle phalanx
Fibrous digital sheaths: strong ligamentous tunnels that contain the flexor tendons and their synovial sheaths
Extend from the heads of the metacarpals to the bases of the distal phalanges
Prevent the tendons from pulling away from the digits
Reinforced by the annular and cruciform ligaments (also referred to clinically as pulleys)
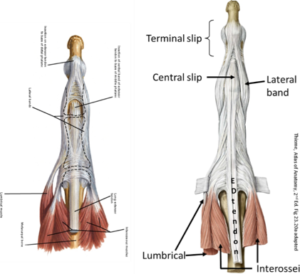
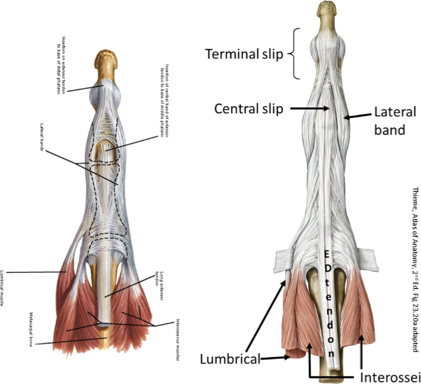
Extensor hoods (dorsal digital expansions)
Figure 11.17
As the four tendons of the extensor digitorum muscle reach the metacarpophalangeal joints (“knuckles”), they flatten and widen to form aponeuroses called extensor hoods over the dorsal surfaces of digits 2–5. Each hood has three parts: a median band and two lateral bands.
Median band: Attaches to the base of the middle phalanx
Two lateral bands: Attach to the base of the distal phalanx
Lumbricals and interossei: Attach to the lateral bands
The median bands permit the extensor digitorum muscle to extend digits 2–5 at the metacarpophalangeal (MCP) joints, while the lateral bands allow the lumbrical and interosseous muscles to extend the interphalangeal (IP) joints of the same digits.