The forearm is the intermediate segment of the free upper limb, between the elbow and wrist. Like the arm, it contains anterior and posterior compartments. However, in the forearm two bones are interposed between the compartments, the radius and ulna.
Bones of the forearm
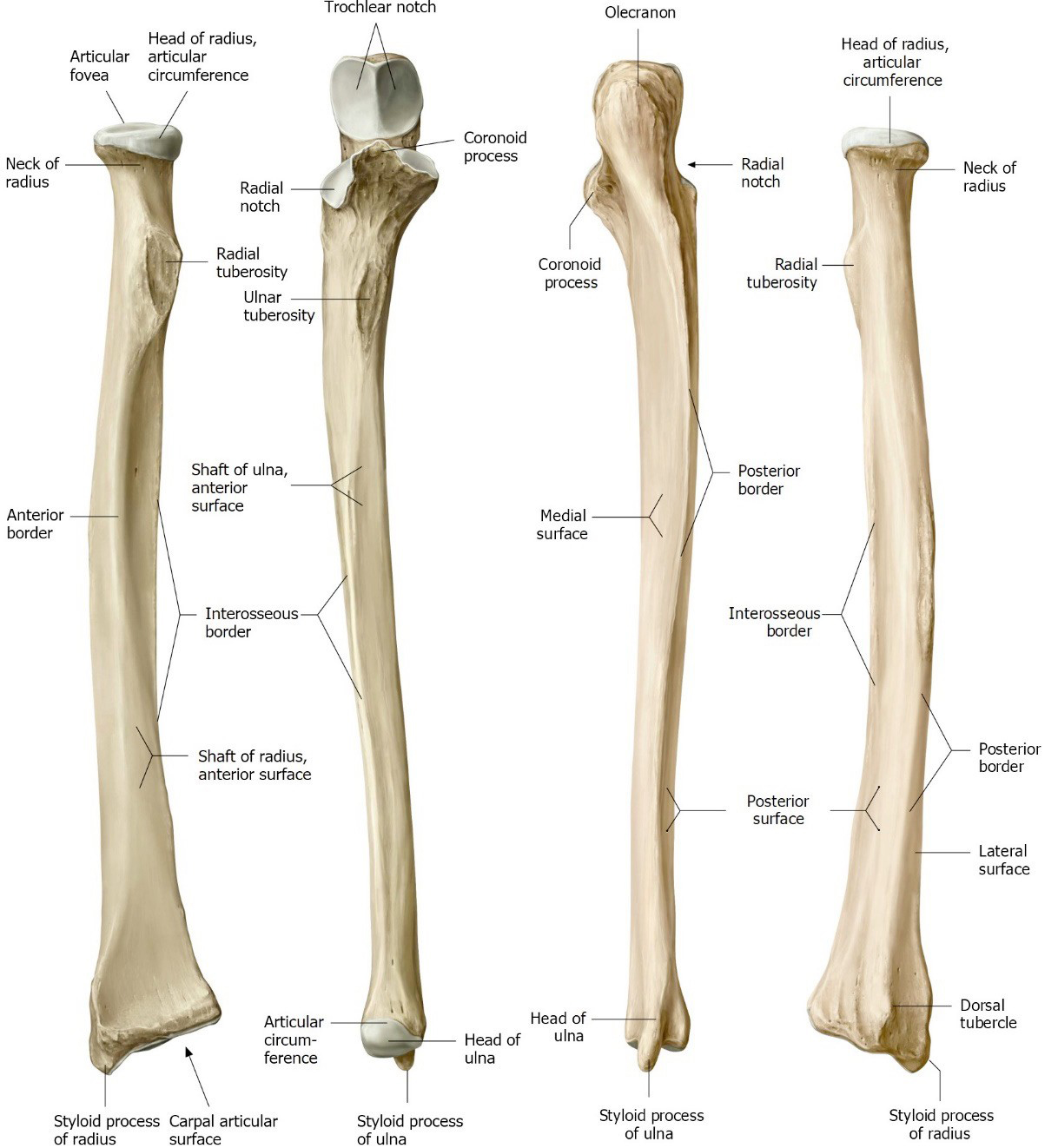
The radius is the pre-axial bone; the ulna is postaxial (recall this by assuming the anatomical position). Both are classified as long bones. When the forearm is supine, the radius and ulna are parallel. The two bones complement one another in terms of their shapes: proximally the radius is narrow while the ulna is wide; distally the radius is wide, and the ulna is narrow. The radius and ulna are joined in three places:
Figure 10.10 Radius and ulna. Anterior view (left); posterior view (right). GILROY, ATLAS OF ANATOMY, 3RD ED., THIEME PUBLISHING, FIGS. 26.1 A AND B.
Interosseous membrane
An interosseous membrane stretches between their shafts, binding them firmly and causing them to behave as one bone. For example, the two bones move together at the elbow when it is flexed or extended.
Synovial joints
At their ends, the bones are joined by synovial joints. These are the proximal and distal radio-ulnar joints (described later in this chapter). These allow the radius to rotate around the ulna, producing the movements of supination and pronation that are unique to the forearm.
Radius
Ulna
The proximal radius contains two important features:
A circular head. The distal part of the head is concave so that it can fit around the capitulum of the humerus at the elbow. The circumference of the head articulates with a groove in the proximal ulna (radial notch), forming the proximal radio-ulnar joint.
Distal to the head, the radial tuberosity projects medially toward the ulna. Do you recall the significance of the radial tuberosity?
The central part of the radius (diaphysis) is the shaft (body). The ulna has one too.
The distal radius has these features:
A wide concave surface that articulates with carpal bones at the wrist.
A groove (ulnar notch) that articulates with the ulna at the distal radio-ulnar joint.
A sharp styloid process (Latin, stylo– = resembling a post) that projects laterally—a good landmark for finding the pulse of the radial artery.
A small bump on the dorsal side, the dorsal tubercle of the radius (Lister’s tubercle), serves as a pulley for the tendon of a thumb muscle (extensor pollicis longus).
The proximal part of the ulna resembles the business end of a wrench as it fits around the distal humerus at the elbow joint. It has two prominent projections: the coronoid process anteriorly and the olecranon posteriorly. Between these is a deep groove = the trochlear notch. The trochlea of the humerus of course fits here. Two important muscles in the arm insert onto the coronoid process and the olecranon, respectively. Do you recall which ones?
Distally, the ulna narrows to form a rounded head. The styloid process projects distally from the head toward the wrist and is easily palpable on the posterior side.
Note
Both radius and ulna have styloid processes at their distal ends. They can be palpated simultaneously between the thumb and index finger of the opposite hand. Don’t confuse them on a lab exam!
Conley's clues
To avoid confusion, say: radial styloid or ulnar styloid.
Clinical correlation
A Colle’s fracture is the most common type of distal radius fracture. They occur proximal to the wrist joint in the metaphyseal (growth-plate) region of the radius and are usually caused by a fall on an outstretched hand (FOOSH)—a pronated forearm with wrist extended.
Figure 10.11 Dinner fork deformity.
They can occur in all adult age groups but are most common in patients with osteoporosis. They usually present with posterior displacement and/or angulation of the distal radius bone fragment. If the angulation is severe enough, it is known as a “dinner fork deformity.”
Treatment depends on the type of fracture (there are many classification schemes) and age of the patient. Non-displaced fractures can be treated conservatively with casting. More severe fractures may require surgery (open reduction) and fixation with devices to hold the bone in place (e.g., screws, plates, or pins).
Fasciae of forearm
Like the arm, the superficial fascia in the forearm contains superficial veins (many) and cutaneous nerves. Deep fascia of the forearm (antebrachial fascia) is incredibly snug around the muscles; in fact, some forearm muscles take their origins from the deep fascia. The deep forearm fascia keeps the muscles fastened down in layers so that their tendons can slide back and forth to move the wrist, hand, and fingers. The anterior and posterior compartments of the forearm are defined by the deep fascia, the medial and lateral intermuscular septa, the radius and ulna, and the interosseous membrane. Compartments contain muscles, nerves, and vessels.
Forearm muscles
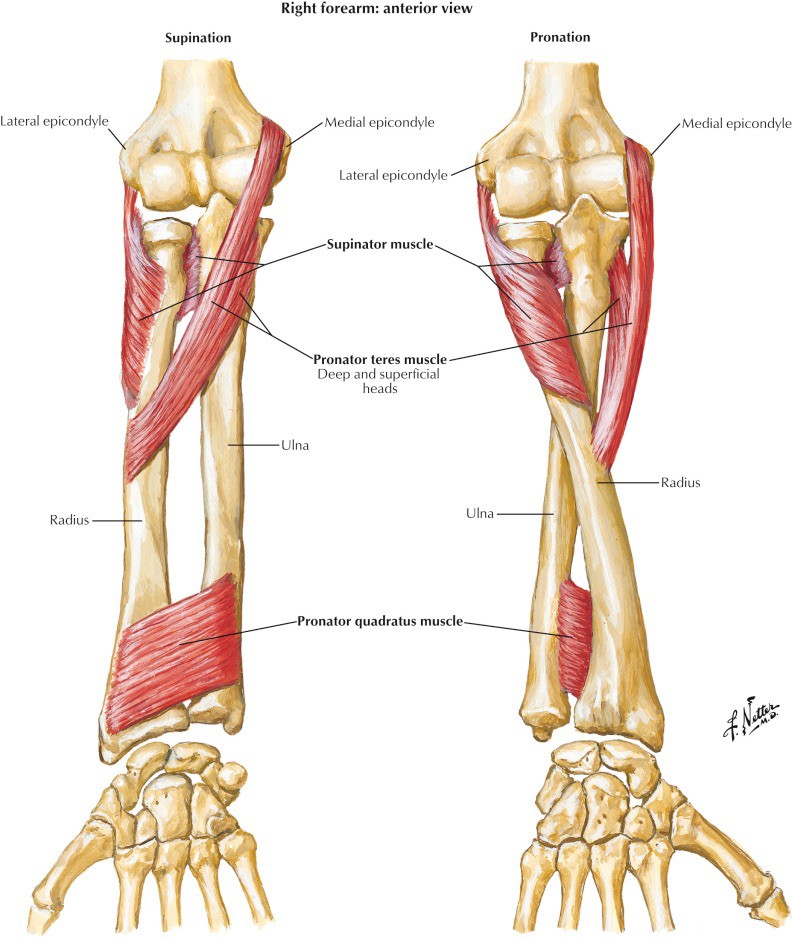
Figure 10.12 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 430.
The forearm contains a bewildering number of muscles. Understanding them is complicated since most of them cross several joints. They are arranged in layers within the anterior and posterior compartments. Most of them have a long, fusiform shape, with fleshy bellies proximally (their origins) and long tendons that taper distally to concentrate the pull of the muscle at a distal attachment (insertion). This gives the muscles precise targeted actions that contribute to the incredible dexterity of the wrist and hand. We will tackle the muscles in a couple of different ways: first, as an overview, we will lump them into functional groups; then we will investigate them by layers within the compartments. The latter method is recommended when dissecting and studying the muscles in the lab.
These movements of the forearm are each produced by two pairs of muscles that act upon the radio-ulnar joints.
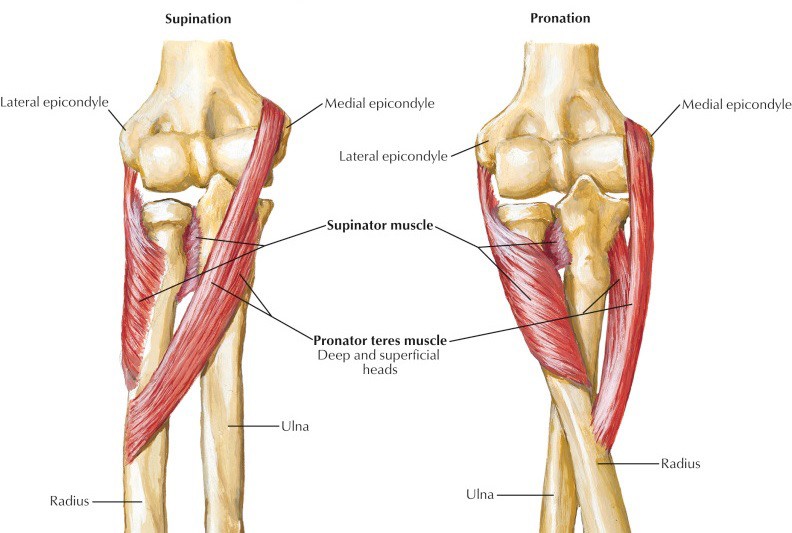
The muscles producing pronation are the pronator teres and pronator quadratus. These are in the anterior compartment. When the forearm is pronated, the radius crosses the ulna.
Muscles that produce supination include the supinator (in the deep posterior compartment) and the biceps brachii (discussed earlier with the arm).
These muscles act to flex or extend the wrist. Some, depending on their positions, can also adduct or abduct the wrist. These movements are also known as ulnar deviation and radial deviation, respectively.
In the anterior compartment are the flexor carpi radialis and flexor carpi ulnaris.
On the posterior side are the extensor carpi radialis (longus and brevis = two separate muscles) and extensor carpi ulnaris.
The fingers are moved by short muscles within the hand (intrinsic muscles) and long muscles outside the hand (extrinsic muscles). The extrinsic finger muscles are in the forearm.
There are two flexors of the digits in the anterior forearm: the flexor digitorum superficialis and flexor digitorum profundus. The names describe their actions and relative locations to one another (profound = deep).
Muscles that extend the digits are in the posterior forearm. The extensor digitorum sends tendons to the medial four digits. Additionally, the pinky finger and index finger receive a second muscle tendon: the extensor digiti minimi to the little finger and extensor indicis to the index finger.
Like the other four digits, the thumb is moved by both intrinsic muscles within the hand and extrinsic muscles with their origins in the forearm. All these muscles include the name “pollicis” since the Latin word for thumb is pollex.
The flexor pollicis longus is deep within the anterior compartment.
Two thumb extenders and an abductor are in the posterior compartment: extensor pollicis longus and brevis and the abductor pollicis longus.
Conley's clues
Dissecting the long-winded names is helpful. Actions, attachments, and locations are all there! Example: The flexor carpi radialis is a muscle that flexes the wrist (carpus is another namefor wrist) located on the lateral (radial) side of the forearm. Piece of cake!
Do you see a pattern here?
The anterior compartment contains pronators of the forearm and flexors of the wrist, digits, and thumb.
The posterior compartment contains a forearm supinator and extensors of the wrist, digits, and thumb (as well as an oddball = an abductor of the thumb).
Now, let’s take a deeper dive into the forearm compartments.
Anterior compartment of forearm
Muscles
A good strategy is to organize the muscles into three layers:
superficial
intermediate
deep.
Superficial layer
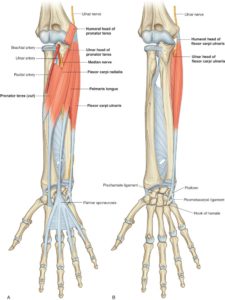
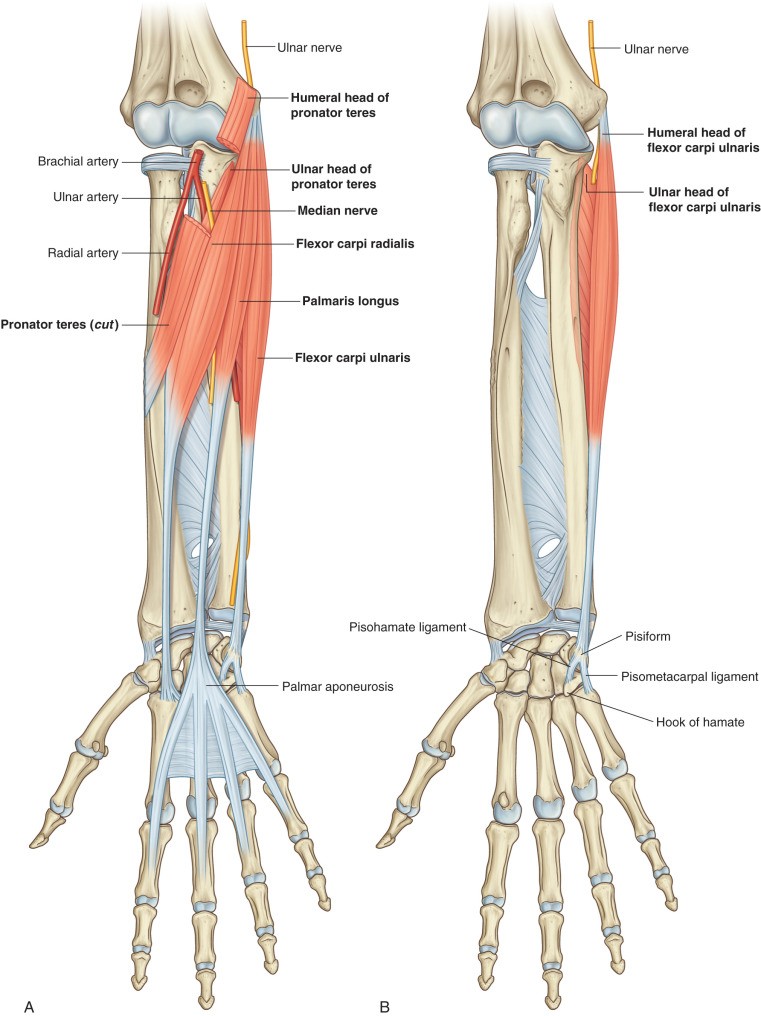
Figure 10.14 Anterior compartment of forearm: Superficial layer of muscles. Drake, Gray’s Anatomy for Students, 4th ed., Fig. 7.85.
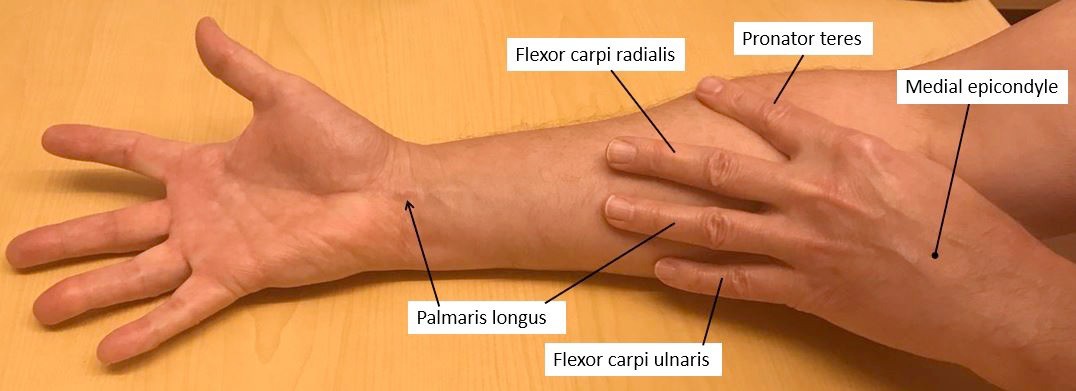
Four muscles. All originate from the medial epicondyle of the humerus, via a common flexor tendon. Since these muscles cross the elbow joint, they all can act as weak flexors of the elbow, assisting the biceps brachii and brachialis. However, their more important functions occur distally.
Pronator teres: Originates via two heads, a humeral head from the common flexor tendon and an ulnar head from the coronoid process. The median nerve passes through a gap between the two heads. It inserts into the shaft of the radius. Pronates the forearm.
Flexor carpi radialis: Originates from the common flexor tendon. Inserts on the 2nd metacarpal bone. Flexes and abducts the wrist.
Palmaris longus: Functionally not very important, it is probably a vestige of a muscle that flexed the metacarpophalageal (MCP, knuckle) joints that was later replaced by more evolved muscles in the hand. Arises from the common flexor tendon. Has a small muscular belly and a long, thin tendon. Inserts into an aponeurosis on the palm of the hand. Weak flexor of the wrist. It is missing in a substantial number of folks (~15%) on one or both sides. Although it’s not much of a wrist flexor, the palmaris longus is useful as a guide to locating the median nerve at the wrist (the nerve is just lateral to the palmaris longus tendon) and its tendon can be harvested and used as a graft in reconstructive hand surgery.
Flexor carpi ulnaris: Originates via two heads, a humeral head from the common flexor tendon and an ulnar head. The ulnar nerve passes between the two heads.Inserts onto the pisiform—one of the carpal bones of the wrist. Flexes and adducts the wrist.
All muscles in the superficial layer are innervated by the median nerve except the flexor carpi ulnaris, which is supplied by the ulnar nerve.
Conley's clues
Place a forearm in the supine position, then four fingers of the other hand on the forearm extending distally from the medial epicondyle. The fingers simulate the positions of the four muscles in the superficial layer. Look, I’ve got a palmaris longus!
Figure 10.13
Clinical correlation
Medial epicondylitis (“golfer’s elbow”) is an overuse tendinopathy of the common flexor tendon. It is associated with sports that require repetitive forearm or wrist flexion, including golf, bowling, and weightlifting. The hallmark is pain and tenderness on the inside of the elbow at the medial epicondyle. It can be treated with medications, support from an elbow brace, and/or physical therapy.
Intermediate layer
Deep layer
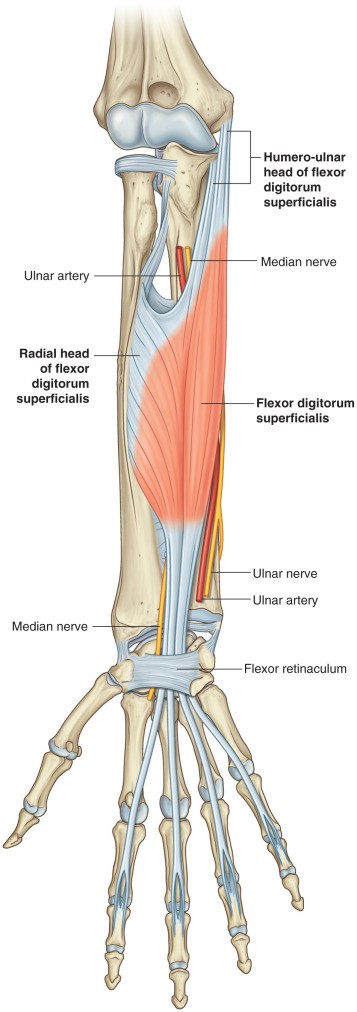
Figure 10.15 Anterior compartment of forearm: Intermediate muscle layer. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.86.
One muscle: The flexor digitorum superficialis (FDS). This muscle is deep to the muscles in the superficial layer. It has a wide origin from the common flexor tendon, coronoid process of ulna, and shaft of the radius. All the points of origin are connected proximally by an arched membrane, under which the median nerve and ulnar artery pass. Distally, the fleshy belly of the FDS divides into four tendons which pass through the carpal tunnel into the hand where they insert on the middle phalanges of the medial four fingers. FDS acts as a flexor of the joints it crosses. It can flex the wrist and the metacarpophalangeal (MCP) joints, but its most important action is to flex the proximal interphalangeal (PIP) joints of the medial four digits.
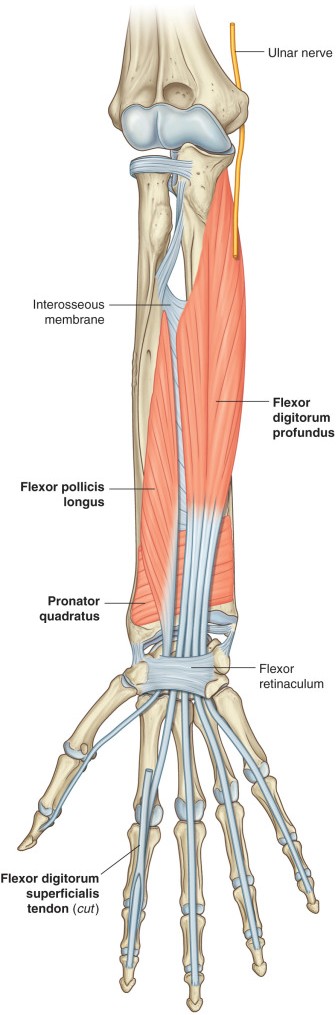
Figure 10.16 Anterior compartment of forearm: Deep layer of muscles. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.86.
Three muscles, deep to the intermediate layer; these muscles are adjacent to the shafts of the radius and ulna and the interosseus membrane.
Flexor pollicis longus: The extrinsic flexor muscle of the thumb. Being outside the hand, it requires a long tendon to do its job. Originates from the anterior surface of the radius, it has a characteristic unipennate muscle fiber arrangement (the muscle fascicles are located on one side of the tendon). From this fleshy belly in the forearm, the tendon passes through the carpal tunnel to insert on the thumb’s distal phalanx. Flexes the interphalangeal (IP) and MCP joints of the thumb.
Flexor digitorum profundus (FDP): The deep flexor muscle of the medial four digits (profundus = deeply placed, think of the word profound). It arises from the anterior surface of the ulna and the interosseus membrane. The fleshy belly of the FDP divides into four tendons distally and these pass through the carpal tunnel and the palm of the hand deep to the tendons of the FDS. The tendons of the FDP insert on the distal phalanges of the medial four digits. The primary function of the FDP is to flex the distal interphalangeal (DIP) joints. It can also contribute to flexion of the proximal interphalangeal (PIP), metacarpophalangeal (MCP), and wrist joints.
Pronator quadratus: The deepest muscle in the anterior compartment, it is underneath the FDP and flexor pollicis longus in the distal part of the forearm. Originates from the ulna and inserts on the radius. Its width can be imagined by placing four fingers across the anterior forearm, with the pinky finger at the wrist.
All the muscles in the deep layer of the anterior compartment are innervated by the anterior interosseus nerve (a deep branch of the median nerve), except the medial (ulnar) half of the flexor digitorum profundus, which is supplied by the ulnar nerve. Therefore, the FDP has a dual innervation = lateral (radial) two tendons supplied by the anterior interosseous nerve and medial (ulnar) two tendons supplied by the ulnar nerve.
Conley's clues
The name describes its action and shape (quadratus = four sides). Don’t be a and miss this one on an exam!
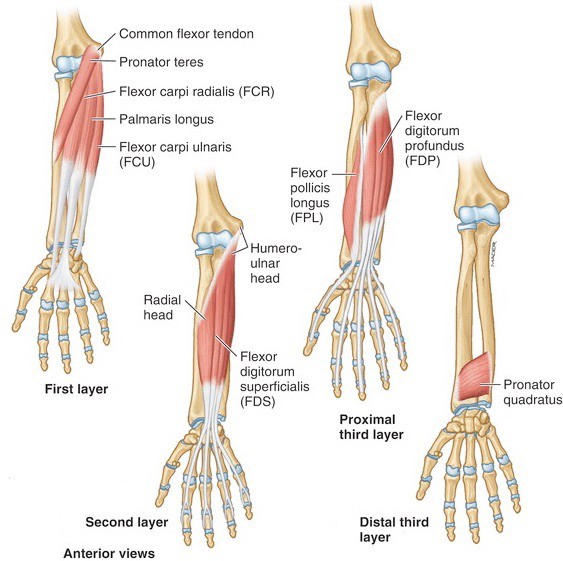
Figure 10.17 Summary of muscle layers in anterior compartment of forearm. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.59.
Table10.3 Muscles in the Anterior Compartment of the Forearm
Muscle
Proximalattachment (origin)
Distal attachment (insertion)
Innervation
Primary actions
SUPERFICIAL LAYER
Pronator teres
HUMERAL HEADMedial epicondyle via common flexor tendon
ULNAR HEAD Coronoid process
Shaft of radius
Median nerve
Pronates forearm
Flexor carpi radialis
Medial epicondyle via common flexor tendon
2nd metacarpal
Flexes and abducts hand at wrist
Palmaris longus
Medial epicondyle via common flexor tendon
Palmar aponeurosis of hand
Flexes hand at wrist
Flexor carpi ulnaris
HUMERAL HEAD Medial epicondyle via common flexor tendon
ULNARHEADOlecranon
Pisiform bone
Ulnar nerve
Flexes and adducts hand at wrist
INTERMEDIATELAYER
Flexor digitorum superficialis
Medial epicondyle via common flexor tendon, Coronoid process of ulna, Shaft of radius
Middle phalanges of medial 4 digits
Median nerve
Flexes PIP joints of medial 4 digits; Assists with flexion of MCP and wrist joints
DEEPLAYER
Flexor digitorum profundus
Shaft of ulna and interosseous membrane
Distal phalanges of medial 4 digits
Medial (ulnar) part: Ulnar nerve
Flexes DIP joints of digits 4 and 5; Assists with flexion of PIP, MCP, and wrist joints
Flexes DIP joints of digits 2 and 3; Assists with flexion of PIP, MCP, and wrist joints
Flexor pollicis longus
Shaft of radius and interosseous membrane
Distal phalanx of thumb
Anterior interosseous nerve
Flexes interphalangeal (IP) and MCP joints of thumb
Pronator quadratus
Anterior surface of distal ulna
Anterior surface of distal radius
Anterior interosseous nerve
Pronates forearm
Nerves
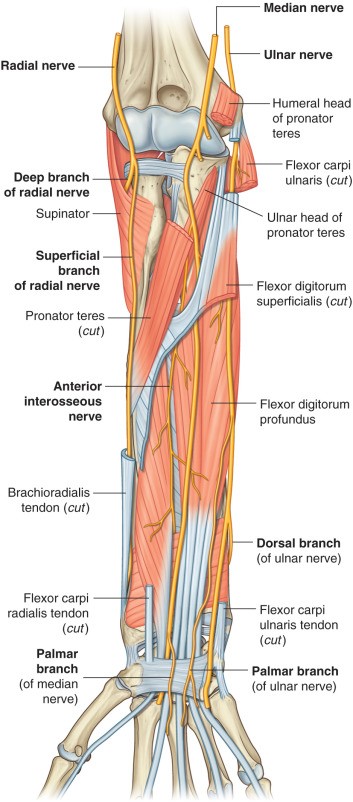
Figure 10.18 Nerves in the anterior forearm. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.89.
The median and ulnar nerves supply the anterior compartment of the forearm and course through it to the hand.
Median nerve: The key player in supplying muscles in the anterior compartment. At the elbow, the median nerve and brachial artery leave the arm and enter the cubital fossa (described later in this chapter) in the proximal part of the anterior forearm. The median nerve leaves the cubital fossa by squeezing between the two heads of the pronator teres. From here it passes deep to the proximal attachments of the flexor digitorum superficialis (FDS) and runs toward the wrist on the deep surface of the FDS. At the wrist it enters the hand through the carpal tunnel. Since it runs down the center (midline) of the anterior forearm, the nerve is called “median.”
Muscles in the superficial and intermediate layers of the anterior compartment that are supplied by the median nerve receive motor fibers from the nerve in the proximal forearm, in or near the cubital fossa. Thus, a lesion of the median nerve proximal to the elbow would affect forearm muscles, while a lesion of the nerve in the mid- or distal forearm would not.
The largest branch of the median is the anterior interosseus nerve. It branches just distal to the pronator teres and dives deep, running distally in the deep layer of the anterior forearm in a groove between the flexor digitorum profundus (FDP) and flexor pollicis longus muscles. It supplies the three muscles in the deep layer, except the ulnar portion of the FDP.
The palmar branch of the median nerve arises just proximal to the wrist. It is a cutaneous nerve that passes into the superficial tissues of the palm of the hand, coursing external to (outside) the carpal tunnel.
Conley's clues
Since the palmar branch arises from the median nerve proximal to the carpal tunnel and does not pass through the tunnel, numb skin on the palm of the hand is not a symptom of carpal tunnel syndrome (entrapment of the median nerve in the carpal tunnel). However, a lesion affecting the median nerve at a more proximal site would produce a numb palm.
Clinical correlation
Entrapment of the median nerve near the elbow is called pronator syndrome. One cause is compression of the nerve between the two heads of the pronator teres.
Much less common than carpal tunnel syndrome, it is seen more often in women and has also been associated with well-developed forearm muscles (e.g. weightlifters). Symptoms include pain in the forearm, numbness and tingling in the palm of the hand and first three fingers, and hand muscle weakness. Entrapment of the median nerve between the two heads of the pronator teres would not normally affect the anterior forearm muscles—why?
Ulnar nerve: Has a small role in the forearm; its major functions are in the hand. After running down the medial side of the arm, the ulnar nerve very briefly enters the posterior compartment of the arm as it swings behind the medial epicondyle of the humerus. Here is runs in a groove between the medial epicondyle and olecranon. This bony groove is covered by a fibrous band, converting the groove into the cubital tunnel. The ulnar nerve enters the anterior compartment of the forearm between the two heads of the flexor carpi ulnaris. From here, it proceeds distally with the ulnar artery toward the wrist between the flexor carpi ulnaris and flexor digitorum profundus. The nerve and artery enter the hand, not through the carpal tunnel, but via a separate fibrous passageway, the ulnar canal (Guyon’s canal).
Proximal to the wrist, the ulnar nerve gives off two cutaneous branches. The dorsal branch of the ulnar nerve winds around the wrist to the dorsum of the hand. The palmar branch of the ulnar nerve supplies the skin on the hypothenar eminence of the palmar hand. These two branches together supply the swath of skin characteristic of the ulnar nerve in the hand = pinky finger, half the ring finger, and the ulnar portion of the palm and dorsum.
Clinical correlation
The ulnar nerve is large and quite superficial (subcutaneous) as it passes behind the medial epicondyle. It can be easily palpated here—if you dare! Compression of the nerve against the bone is an excruciating experience, causing pain, tingling, and temporary numbness in the hand. This phenomenon is known as “hitting your funny bone.”
The term “funny bone” is hardly appropriate since the nerve is the problem. The term must have originated because of the nearby bone (humerus = sounds like humorous) or because of the odd sensation elicited when it is struck. Whatever the case, a contusion of the ulnar nerve is no laughing matter!
The cubital tunnel is a site where ulnar nerve entrapment can occur (cubital tunnel syndrome). It is reported to be the second most common peripheral nerve entrapment syndrome (NCBI). It can be temporarily caused by leaning the elbow on a hard surface or bending the elbow for a sustained period, causing the ulnar nerve to be compressed or kinked in the cubital tunnel.
Sometimes abnormal bone growth or fibrotic tissue in the region can narrow the cubital tunnel and trap the nerve. Early symptoms include numbness and tingling in the medial hand. As the condition progresses, muscle weakness may affect the hand and wrist. Which muscles in the forearm could be affected?
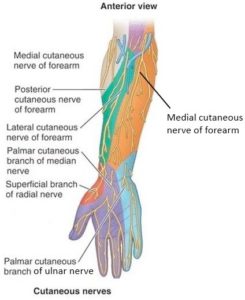
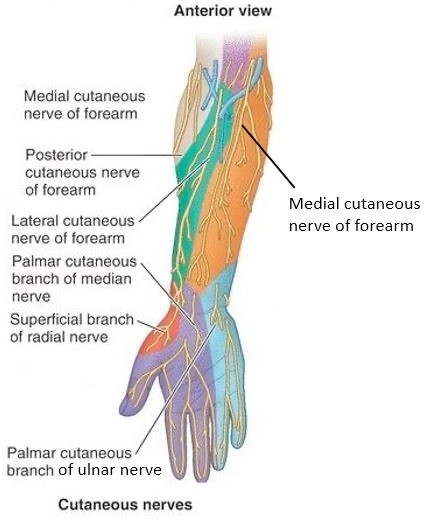
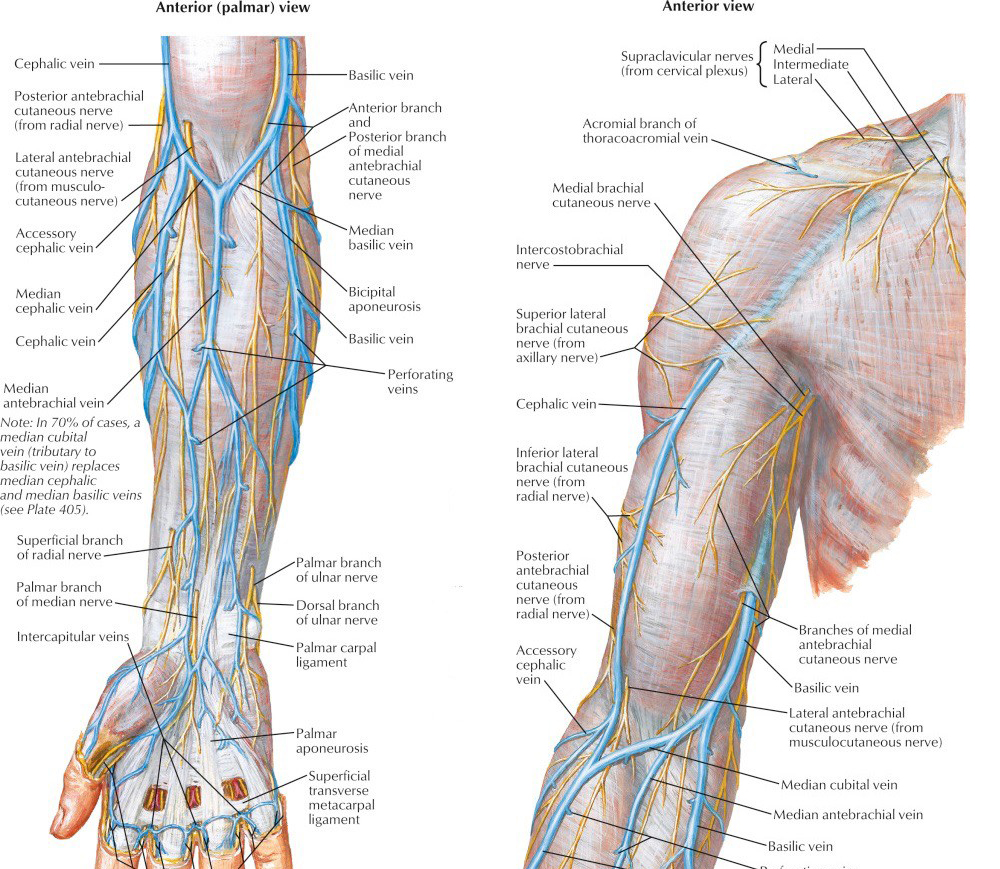
Figure 10.19 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.69 (REVISED).Cutaneous nerves: The skin over the anterior compartment of the forearm is supplied by two nerves. On the medial side is the medial cutaneous nerve of the forearm, extending from the medial cord of the brachial plexus in the axilla all the way to the forearm. On the lateral side is the lateral cutaneous nerve of the forearm, the distal continuation of the musculocutaneous nerve (described with the arm in the previous section).
Vessels
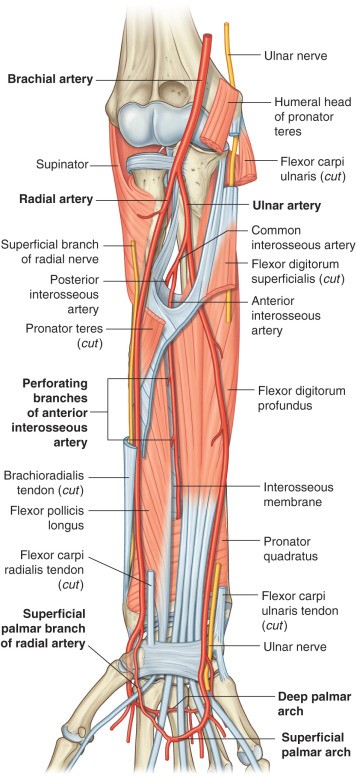
Figure 10.20 Arteries in the anterior forearm. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.88.
The brachial artery enters the cubital fossa in the proximal forearm. Here it divides into radial and ulnar arteries.
Radial artery: Arises deep in the cubital fossa, crosses over the biceps tendon, and heads distally along the shaft of the radius, deep to the brachioradialis muscle. In the distal forearm, medial to the styloid process of the radius, the radial artery becomes superficial between the tendons of the brachioradialis and flexor carpi radialis. Its pulsations can be felt by pressing the artery against the bone (radial artery pulse). From here, the radial artery loops posteriorly and enters the hand.
Ulnar artery: The larger of the two terminal branches of the brachial artery. After leaving the cubital fossa it dives under the fibrous arch formed by the origin of the flexor digitorum superficialis (FDS) and travels distally in the medial forearm on the surface of the flexor digitorum profundus, where it is joined by the ulnar nerve.The ulnar artery pulse can be felt with some effort near the wrist, proximal to the pisiform bone and lateral to the tendon of the flexor carpi ulnaris. The ulnar artery and nerve enter the hand through the ulnar (Guyon’s) canal.
The largest branch of the ulnar artery in the forearm is the common interosseous artery, given off from the lateral side of the ulnar artery just after it passes below the FDS. It immediately divides into anterior and posterior interosseous arteries. The posterior interosseus artery loops around the upper border of the interosseous membrane into the posterior compartment of the forearm. The anterior interosseous artery accompanies the anterior interosseous nerve (from the median nerve) distally, adjacent to the interosseous membrane, supplying the muscles in the deep layer of the anterior forearm.
Radial and ulnar veins: The radial artery is accompanied by two radial veins, and the ulnar artery by two ulnar veins. These are known as the venae comitantes (companion veins) of the arteries. The veins fuse in the cubital fossa to form two brachial veins.
Superficial veins (in the superficial fascia): As mentioned previously (Introduction to the Limbs), two large superficial veins arise at the wrist from the dorsal venous network on the posterior hand.
The cephalic vein runs along the lateral (pre-axial) border of the forearm into the arm.
The basilic vein runs along the medial (postaxial) border of the forearm into the arm.
Additionally, in the anterior forearm there are numerous antebrachial veins in various patterns between the cephalic and basilic veins. Sometimes a large median antebrachial vein runs up the center of the anterior forearm to the cubital fossa.
Superficial veins in the anterior forearm near the elbow seem to follow two patterns:
The median antebrachial vein if present may split over the cubital fossa and join the cephalic and basilic veins. In this case, the veins form an “M” pattern.
A single vein called the median cubital vein may join the cephalic and basilic veins over the cubital fossa. In this case, the veins form an “H” pattern. This is the most common pattern of veins in the cubital fossa (~80% of cases).
Figure 10.21 Superficial veins of the forearm: “M” pattern (left); “H” pattern (right). NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATES 405 AND 406.
The cubital fossa
This clinically important region is anterior to the elbow joint and straddles the anterior arm and forearm. It is worth knowing about since it contains nearly all the nerves and vessels that supply the forearm and hand (the exception being the ulnar nerve). We will consider it here since it is mainly in the anterior compartment of the forearm.
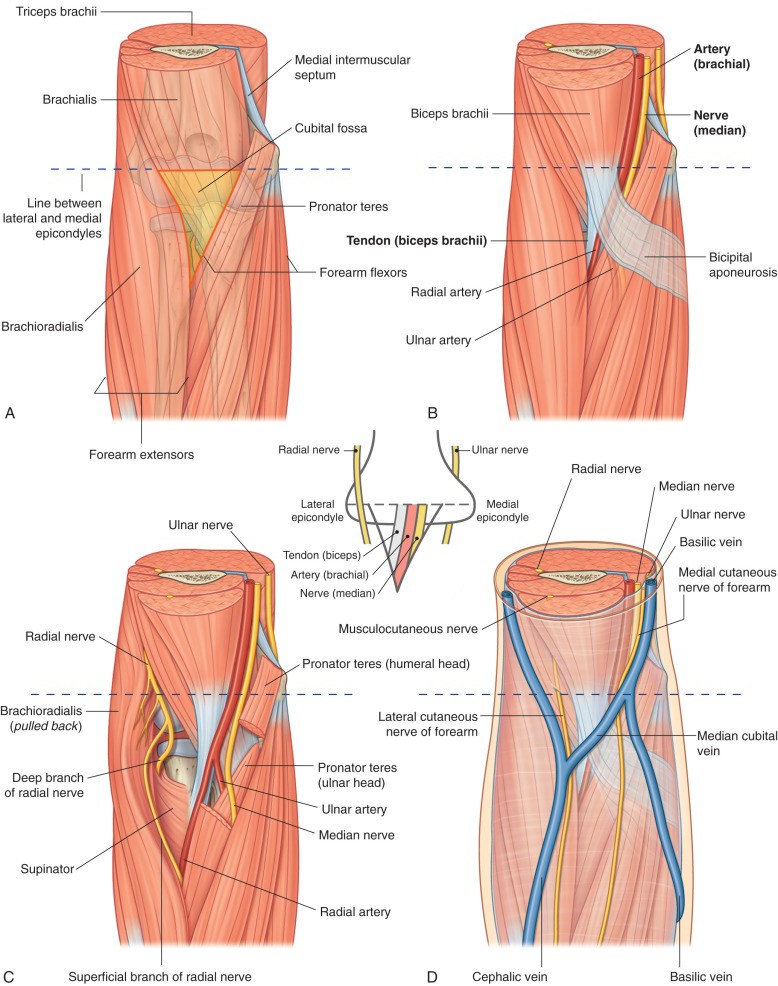
Figure 10.22 The cubital fossa. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.77.
Boundaries
Contents
The cubital fossa is an inverted triangle = wide proximally and tapered to an apex distally.
Base of the triangle: A line drawn between the two humeral epicondyles.
Medial side: Pronator teres muscle
Lateral side: Brachioradialis muscle
The roof of the cubital fossa is formed by the bicipital aponeurosis. Recall that this is a sheet of fibrous tissue arising from the biceps tendon that fuses with the deep fascia of the forearm. The bicipital aponeurosis forms a protective blanket over the contents of the cubital fossa.
The floor is formed by the brachialis and supinator muscles.
Overlying the fossa (not technically in it), in the superficial fascia, are clinically important superficial veins. These are usually arranged in an “M” or “H” pattern (described in the previous section—the “H” pattern is more common). In the case of an “H”, the cross bar is the median cubital vein —it connects the cephalic and basilic veins, which are the vertical posts of the “H.” The veins are separated from the cubital fossa by the bicipital aponeurosis.
The tendon of the biceps brachii is in the center of the fossa. Recall that it attaches to the radial tuberosity.
Medial to the biceps tendon is the brachial artery. Deep in the fossa the brachial artery bifurcates into radial and ulnar arteries.
The median nerve is medial to the brachial artery.
The radial nerve is lateral to the biceps tendon, in the extreme lateral corner of the fossa, under the brachioradialis muscle. As it leaves the fossa, the radial nerve divides into superficial and deep branches.
Summary
The structures related to the cubital fossa can be imagined lined up along the crease of skin in front of the elbow, from lateral to medial:
Venipuncture is a procedure where a needle is used to obtain blood from a vein for laboratory analysis (also known as a “blood draw”) or to enter a vein to administer intravenous therapy.
A vein over the cubital fossa (median cubital vein or equivalent veins in the case of an “M” pattern) is the most common site for a blood draw. Knowledge of anatomy is paramount here—because the pulsating brachial artery and median nerve are deep to the vein, separated only by the bicipital aponeurosis. The median cubital vein is a fine place for a blood draw, but not always preferred by clinicians for intravenous infusion of drugs or placement of an IV cannula because of the danger deep to it.
The biceps reflex, a deep tendon reflex routinely tested during a physical exam, is elicited by tapping the tendon of the biceps within the cubital fossa with a reflex hammer. It tests the C-5 spinal nerve.
The manual method of measuring a patient’s blood pressure involves inflating a cuff around the arm and listening to the flow of blood through the brachial artery in the cubital fossa with a stethoscope. Another application of anatomical knowledge that is taken for granted!
Posterior compartment of forearm
Muscles
The posterior compartment contains muscles that supinate the forearm and extend the wrist and digits. These are all innervated by the radial nerve. In considering the muscles, it is best to organize them into superficial and deep groups.
Superficial layer
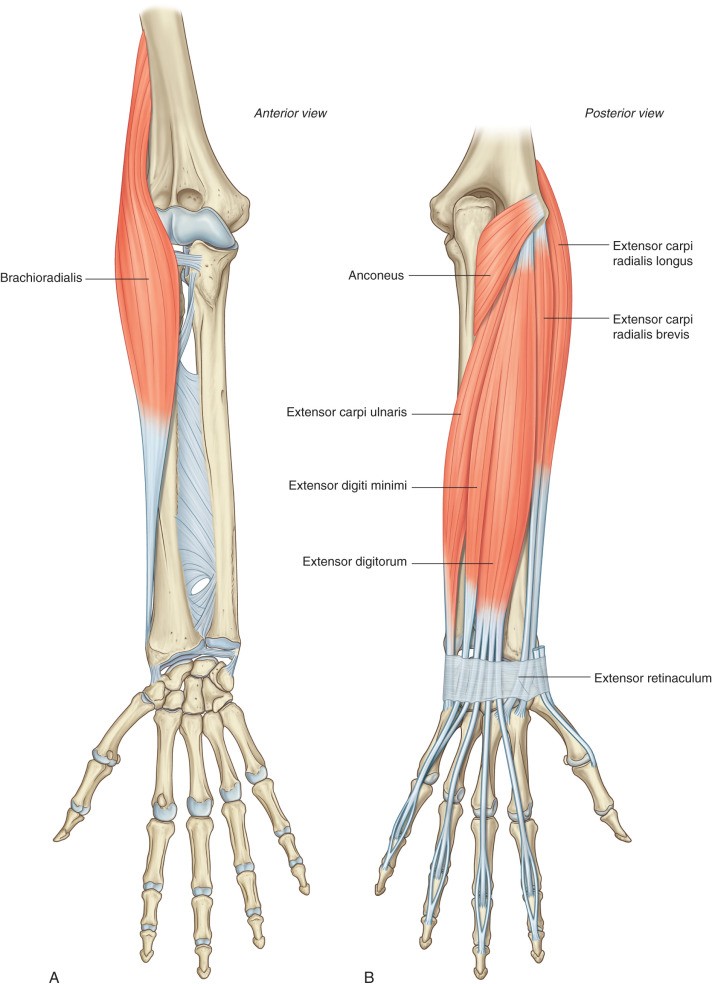
Figure 10.23 Superficial muscles in the posterior compartment of the forearm. Note that the brachioradialis is best seen in the anterior forearm—it flexes the elbow yet is innervated by the radial nerve. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.90.
Brachioradialis: This muscle is an odd one. It is located along the pre-axial border of the limb and straddles the two forearm compartments. It originates higher up the arm than other forearm muscles, from the lateral supracondylar ridge. It inserts distally via a flat tendon on the radius near the styloid process (does not cross the wrist joint). Since it crosses anterior to the elbow, it flexes this joint, and thus functionally belongs in the anterior compartment. It is active when the forearm is semi-pronated and the elbow works against resistance—then you see “B-rad” bulging impressively. This is especially useful when hoisting a mug of beer! Innervation-wise, it belongs in the posterior compartment since it is supplied by the radial nerve before it divides into superficial and deep branches.
Extensor carpi radialis longus: Originates from the lateral supracondylar ridge distal to the brachioradialis. Inserts on the base of the second metacarpal bone. Innervated by the radial nerve before it divides into superficial and deep branches. Extends and abducts the wrist
Extensor carpi radialis brevis: The shorter of the pair, it originates via the common extensor tendon from the lateral epicondyle. Inserts on the base of the third metacarpal bone. Supplied by the deep branch of the radial nerve. Extends and abducts the wrist.
The brachioradialis and the two radial extensors of the wrist (longus and brevis), by virtue of their locations on the lateral side of the forearm and their origins farther up the humerus, together produce a muscular mass that is visible to the naked eye, palpable, and moveable as a unit. Sometimes referred to as the “lateral compartment” of the forearm, it is also called the mobile wad (of Henry), since it is relatively mobile and can be retracted during surgery.
Extensor digitorum (old-timers might call it the extensor digitorum communis = common extensor = since it is a muscle that extends more than one digit). Originates from the common extensor tendon, this muscle runs down the center of the posterior forearm. Distally it divides into three or four tendons that insert into the extensor expansion (extensor hood) on the dorsal side of the medial four digits. Its prime function is to extend the metacarpophalangeal (MCP) joints. It can also assist with extension of the interphalangeal (IP) joints of the medial four digits and wrist extension. Supplied by the posterior interosseous nerve (Note: the posterior interosseous nerve is the continuation of the deep branch of the radial, distal to the supinator muscle).
Extensor digiti minimi: This muscle is sometimes hard to recognize as a separate entity. It arises with the extensor digitorum from the common extensor tendon. Distally it diverges from the extensor digitorum to form a separate tendon that inserts independently into the extensor expansion on the dorsal side of the little finger. Thus, the fifth digit usually receives two tendons on its dorsal side—one from the extensor digitorum and one from the extensor digiti minimi. These tendons extend the little finger at the MCP and IP joints. Innervated by the posterior interosseous nerve.
Extensor carpi ulnaris: Originates from the common extensor tendon and from the proximal ulna. Inserts on the base of the fifth metacarpal bone. Extends and adducts the wrist. Supplied by the posterior interosseous nerve.
Anconeus: This small triangular muscle is an outlier—it is often placed in the posterior compartment of the arm and considered an accessory part of the triceps. It arises from the lateral epicondyle of the humerus and inserts on the olecranon and posterior surface of the ulna. It blends with the medial head of the triceps and assists the triceps in extending the forearm. Innervated by a radial nerve branch that arises in the posterior arm.
Clinical correlation
The tendon of insertion of brachioradialis to the distal radius is subcutaneous and easily accessible. Tapping it with a reflex hammer elicits a deep tendon reflex that tests the C-6 spinal nerve.
Clinical correlation
Lateral epicondylitis (“tennis elbow”) is a tendinopathy of the common extensor tendon caused by overuse. It is common in 30- to 50- year-olds. Pain over the lateral epicondyle that gets worse with activity is the tell-tale sign. Tennis players are singled out because of their repeated backhand shots during matches, but tennis elbow can affect violinists, drummers, carpenters, painters,gardeners, etc.—anyone who extends their forearms repeatably. NSAIDs, orthotics, corticosteroid injections, or physical therapy are some treatments.
Deep layer
“Outcropping muscles” of the deep layer
Anatomical Snuffbox
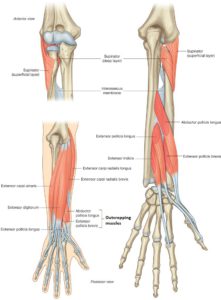
Figure 10.24 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 430.
Muscles in the deep layer include a forearm supinator, three muscles that move the thumb, and a muscle that extends the index finger (extensor indicis). The bellies of these muscles are completely hidden beneath the superficial layer of muscles. The tendons of the thumb muscles and the extensor indicis emerge from beneath the extensor digitorum, seeming to appear from nowhere in the distal forearm. The tendons of the three thumb muscles are especially noticeable, since they diverge at an angle toward the thumb in stark contrast to the muscles in the superficial layer which are all oriented down the long axis of the forearm. Because of this, the three extrinsic muscles of the thumb in the posterior forearm are sometimes called the “outcropping muscles” or “outcroppers.”
Supinator. A thin, curved muscle with complicated attachments. Its origins are from the posterior side of the lateral epicondyle, the radial collateral ligament of the elbow joint, and the lateral surface of the proximal ulna. The muscle has deep and superficial parts. The supinator encircles the proximal radius from behind before inserting on its anterior surface, adjacent to the radial tuberosity and the attachment of the pronator teres. When the forearm is pronated, the radius crosses over the ulna and the supinator is stretched and ready for action—when it contracts it restores the forearm to the supine position, with the radius and ulna parallel to one another. Do you recall the other muscle that can supinate the forearm? The deep branch of the radial nerve innervates the supinator as it passes between its deep and superficial parts.
Extensor indicis: Arises from the posterior surface of the distal ulna where the muscle belly is hidden beneath the extensor digitorum. To pull on the index finger, the tendon of the extensor indicis crosses the wrist obliquely and runs deep to and parallel with the first tendon of the extensor digitorum to the extensor expansion on the dorsum of the index finger. Thus, the index finger has two tendons on it is dorsal surface that can extend its MCP and IP joints (extensor digitorum and extensor indicis). Innervated by the posterior interosseous nerve.
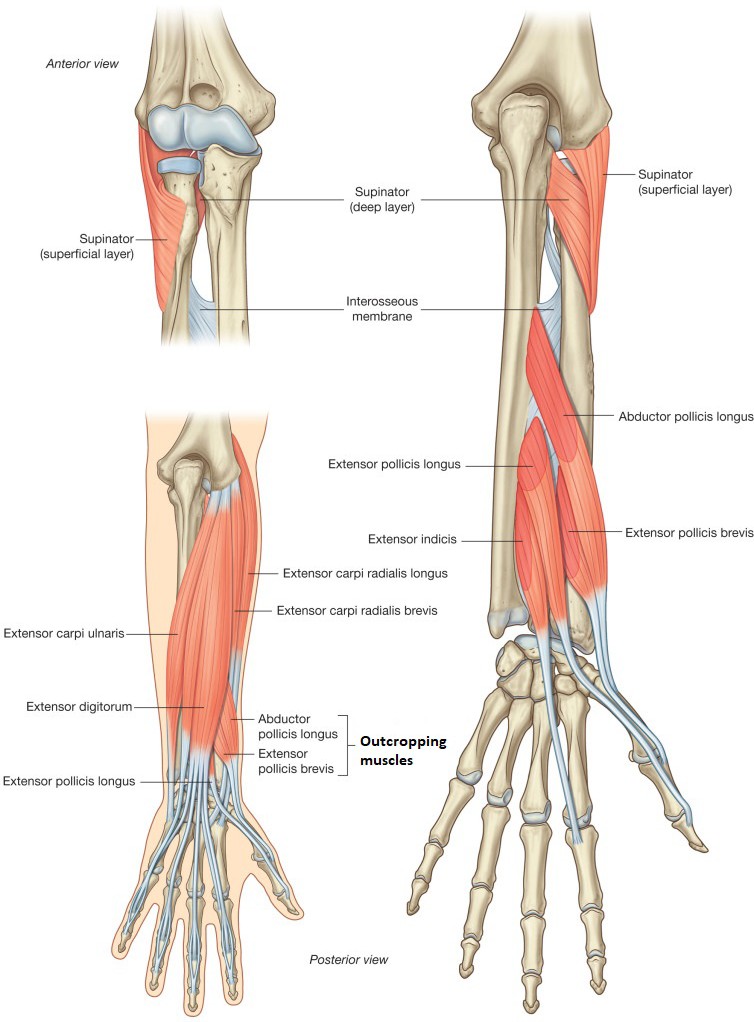
Figure 10.25 Deep muscles in posterior compartment of the forearm. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.90 (REVISED).Extensor pollicis longus: The longest and most medial of the “outcroppers,” it originates from the posterior surface of the ulna and the interosseous membrane. Its tendon hooks around the dorsal tubercle of the radius (Lister’s tubercle), using it as a pulley to get maximum leverage, and inserts on the distal phalanx of the thumb (pollex). Extends the first MCP joint and the IP joint of the thumb. Innervated by the posterior interosseus nerve.
Extensor pollicis brevis: The “baby” thumb extensor is the central “outcropper.” It originates from the posterior radius and interosseous membrane and inserts on the proximal phalanx of the thumb. Extends the MCP joint of the thumb. Innervated by the posterior interosseous nerve.
Abductor pollicis longus: The lateral-most “outcropper” is the extrinsic abductor of the thumb. It arises in the forearm from the posterior surfaces of the ulna, radius, and interosseous membrane. Its tendon runs adjacent to that of the extensor pollicis brevis across the wrist to insert on the lateral (radial) side of the first metacarpal bone. To get there the tendon spirals around the distal radius, using the bone as a pulley to exert force on the thumb. Sometimes the tendon is split into two or three portions to widen its insertion. The abductor pollicis longus abducts and extends the first carpometacarpal joint (the “saddle joint” that allows the thumb to be “opposable”). Abduction and extension returns the thumb to its starting position after it has been placed in opposition to another digit—a movement called “repositioning.” Innervated by the posterior interosseous nerve.
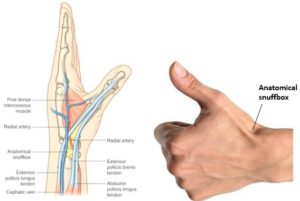
Figure 10.26 DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.100.
When the thumb is extended, a fossa appears at the base of the thumb on the posterior wrist between the tendons of the outcroppers. This depression is known as the anatomical snuffbox. In olden days, those who used “snuff ” (tobacco leaves pulverized into a powder) could place a pinch in the anatomical snuffbox, raise their hand to a nostril, and sniff, delivering a “hit” of nicotine to the mucous membranes in the nasal cavity. The radial boundary is the side-by-side tendons of the extensor pollicis brevis and abductor pollicis longus. The ulnar border is the tendon of the extensor pollicis longus. The scaphoid bone (one of the carpal bones in the wrist) is in the floor of the snuffbox. The radial artery crosses the snuffbox, and its pulse can felt there.
Conley's clues: The supinator
To see this mystery supinator muscle in lab, go to the anterior forearm and trace the pronator teres muscle to its insertion on the shaft of the radius, then retract the “mobile wad” muscles laterally. You will then see the shiny supinator in the depths of the cubital fossa, wrapped around the proximal third of the radius.
Clinical correlation
A fall on an outstretched hand (good old FOOSH injury) can fracture the scaphoid bone. It is the most frequently fractured carpal bone. Pain in the anatomical snuffbox following a fall is a clue. Scaphoid fractures are a problem because of how the bone receives its blood supply. The main artery to the scaphoid enters the bone from the distal side—a fracture through the “waist” (midpoint) of the bone can impede blood flow to the proximal side, resulting in poor healing and the possibility of avascular necrosis.
Table 10.5 Muscles in the Posterior Compartment of the Forearm
Muscle
Proximal attachment (origin)
Distal attachment (insertion)
Innervation
Primary actions
SUPERFICIALLAYER
Brachioradialis (“B-rad”)
Lateral supracondylar ridge of humerus
Distal radius near styloid process
Radial nerve
Flexes forearm at elbow (when semi-pronated)
Extensor carpi radialis longus
Lateral supracondylar ridge of humerus
2nd metacarpal
Extends and abducts hand at wrist
Extensor carpi radialis brevis
Lateral epicondyle via common extensor tendon
3rd metacarpal
Deep branch of radial nerve
Extends and abducts hand at wrist
Extensor digitorum
Lateral epicondyle via common extensor tendon
Extensor expansion on dorsum of medial 4 digits
Posterior interosseous nerve
Extends MCP joints of medial 4 digits; Assists with extension of IP and wrist joints
Extensor digiti minimi
Lateral epicondyle via common extensor tendon
Extensor expansion on dorsum of 5th digit
Extends MCP joint of 5th digit
Extensor carpi ulnaris
Lateral epicondyle via common extensor tendon and posterior ulna
Abducts and extends thumb at 1st carpo- metacarpal joint (saddle joint)
Extensor retinaculum
Retinacula are thickened bands of deep fascia in both upper and lower limbs that function to keep tendons in place when the muscles contract. The extensor retinaculum of the forearm holds down the tendons of the muscles that cross the wrist posteriorly, preventing them from “bowstringing” away from the wrist when the muscles contract. To reduce friction, synovial membranes lubricate the muscle tendons where they pass under the extensor retinaculum.
Nerves
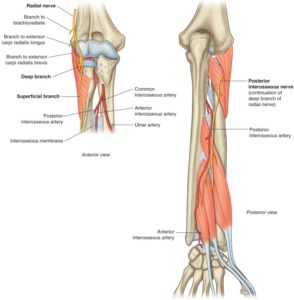
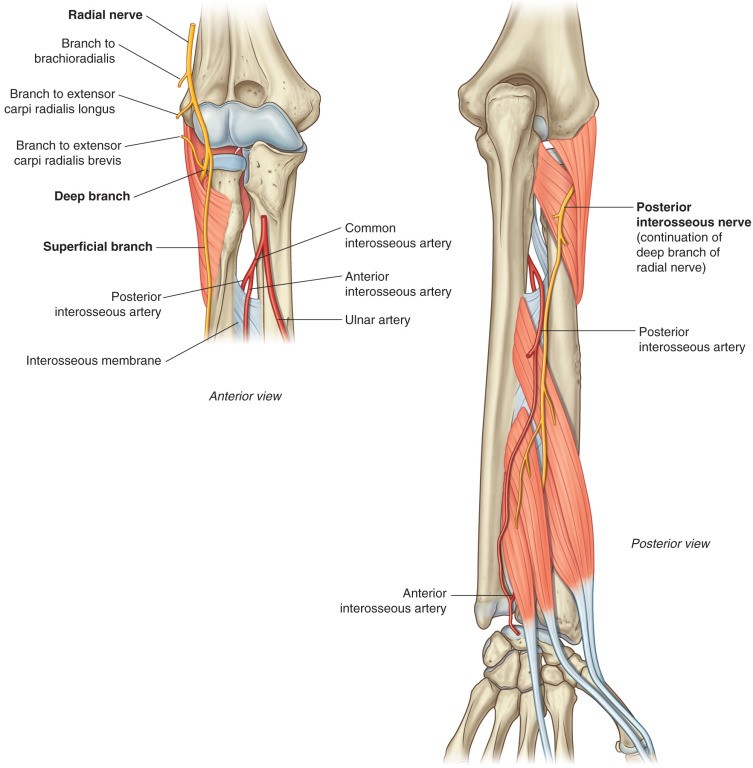
Figure 10.27 Radial nerve in the posterior forearm. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.92.
The radial nerve supplies all the muscles in the posterior compartment of the forearm.
The main trunk of the radial nerve does not enter the posterior compartment of the forearm. Recall that it leaves the posterior compartment of the arm and enters the lateral part of the cubital fossa in the anterior forearm. As it does so, it supplies motor fibers to the brachioradialis and extensor carpi radialis longus. At the lateral edge of the cubital fossa, the radial nerve bifurcates into deep and superficial branches.
Deep branch
Superficial branch
The deep branch of the radial nerve is a motor nerve. It supplies motor fibers to the extensor carpi radialis brevis. It then penetrates the supinator muscle in the floor of the cubital fossa, passing between its superficial and deep parts through what is sometimes called the “radial tunnel.” After innervating the supinator, the nerve emerges from the muscle in the posterior compartment of the forearm. Here the deep radial nerve changes its name to the posterior interosseous nerve. The name is a bit misleading since the nerve runs in the plane between the superficial and deep muscles in the posterior compartment, on the external surfaces of the two lateral “outcropping” muscles, before reaching the wrist. The posterior interosseous nerve is a motor nerve only, supplying most of the muscles in the posterior forearm, except the brachioradialis, the two radial wrist extenders (longus and brevis), and the supinator.
The superficial branch of the radial nerve has no function in the forearm. After leaving the radial nerve near the cubital fossa, it runs down the anterior surface of the radius under cover of the brachioradialis. At the wrist joint it swings around the radius to the dorsal side of the hand where it innervates skin, mainly over the dorsal “web space” between the thumb and index finger. The superficial branch of the radial is a cutaneous nerve.
Clinical correlation
The area of the forearm around the supinator muscle is a potential site for radial nerve entrapment. It’s a fairly rare condition with different names (posterior interosseus syndrome, supinator syndrome, radial tunnel syndrome). There can be many causes: fibrous bands from the elbow joint capsule, compression from a nearby artery (radial recurrent artery), or thickening of the supinator muscle where it forms an arch (arcade of Frohse) over the deep radial nerve at the entrance to the radial tunnel. Depending on location, the deep branch of the radial nerve, posterior interosseus nerve, or both can be affected.
The clinical presentation is typically motor since the nerves are motor only. If the posterior interosseous nerve were completely compressed, there would be no extension of the thumb or digits at the MCP joints (extensor digitorum, extensor indicis, and “outcropping” muscles affected). Extension of the wrist could still occur, but would be weak—why? If wrist drop occurred, could a lesion of the radial nerve at the level of the supinator be the cause? If the deep branch of the radial nerve were damaged, could forearm supination still occur?
Figure 10.28 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.69 (REVISED).Cutaneous nerves of the posterior forearm include the medial cutaneous nerve of the forearm (discussed earlier—also supplies the medial side of the anterior forearm), from the medial cord of the brachial plexus, and the posterior cutaneous nerve of the forearm, a branch of the radial nerve in the posterior arm that descends into the posterior forearm all the way to wrist.
Vessels
The posterior interosseous artery supplies the posterior compartment. It branches from the common interosseous artery (from the ulnar artery) in the anterior forearmand reaches the posterior compartment by passing around the upper border of the interosseous membrane. Emerging below the supinator, it accompanies the posterior interosseous nerve.