■Clean the surface of the masseter muscle.
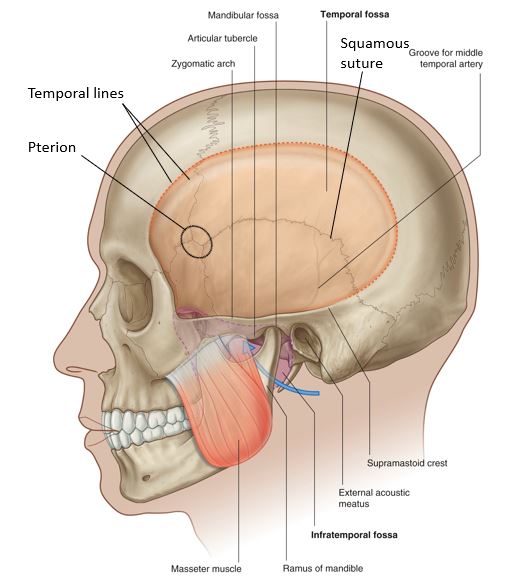
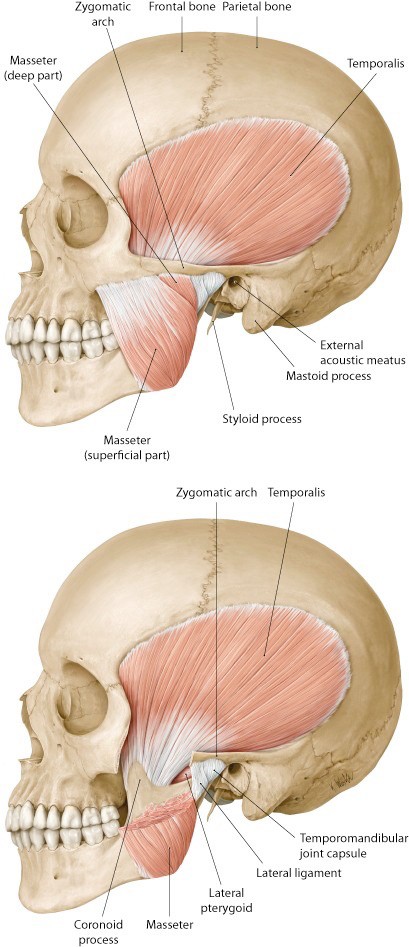
■The masseter is a muscle of mastication. It arises above from the zygomatic bone and zygomatic arch. It inserts below into the external surface of the mandibular ramus and angle of the mandible. What is the function of the masseter?
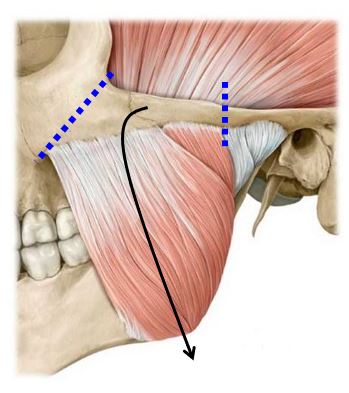
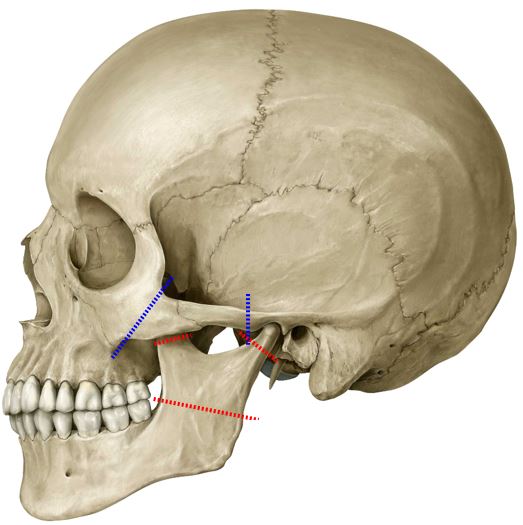
■Use an autopsy saw to make cuts through the zygomatic bone and zygomatic arch, as shown in Figure 30.4. Loosen up the detached segment of zygomatic bone and reflect it downward, along with the attached masseter muscle (Figure 30.4). As you pull down, use a chisel or scissors to scrape/cut away the masseter from its attachment to the external surface of the mandibular ramus. Leave the reflected masseter muscle and zygomatic bone fragment hanging from the mandible or remove it entirely by cutting it at its distal attachment to the angle of the mandible. The external surface of the mandible is now visible.

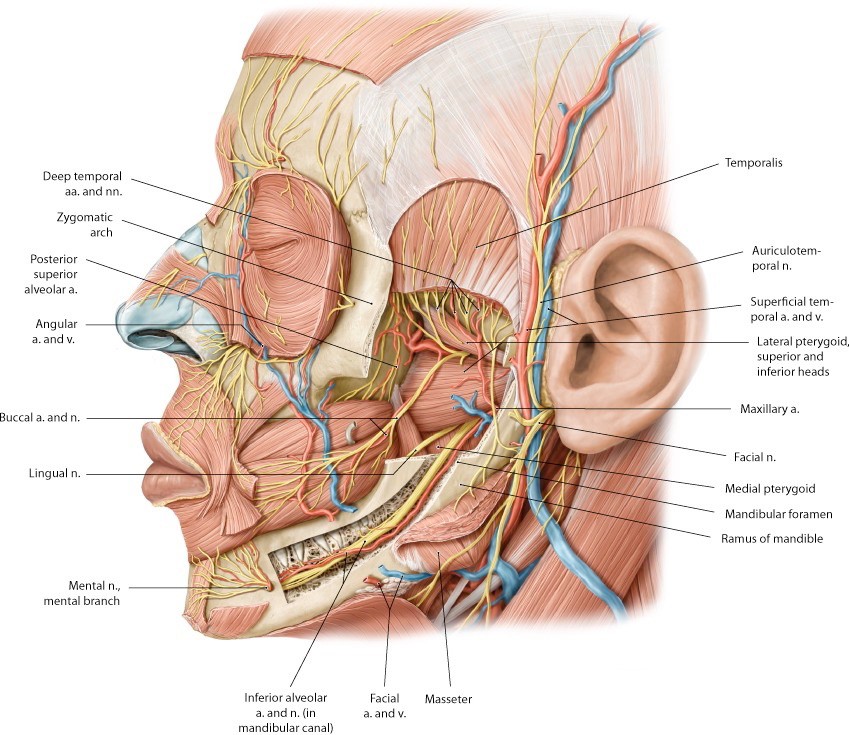
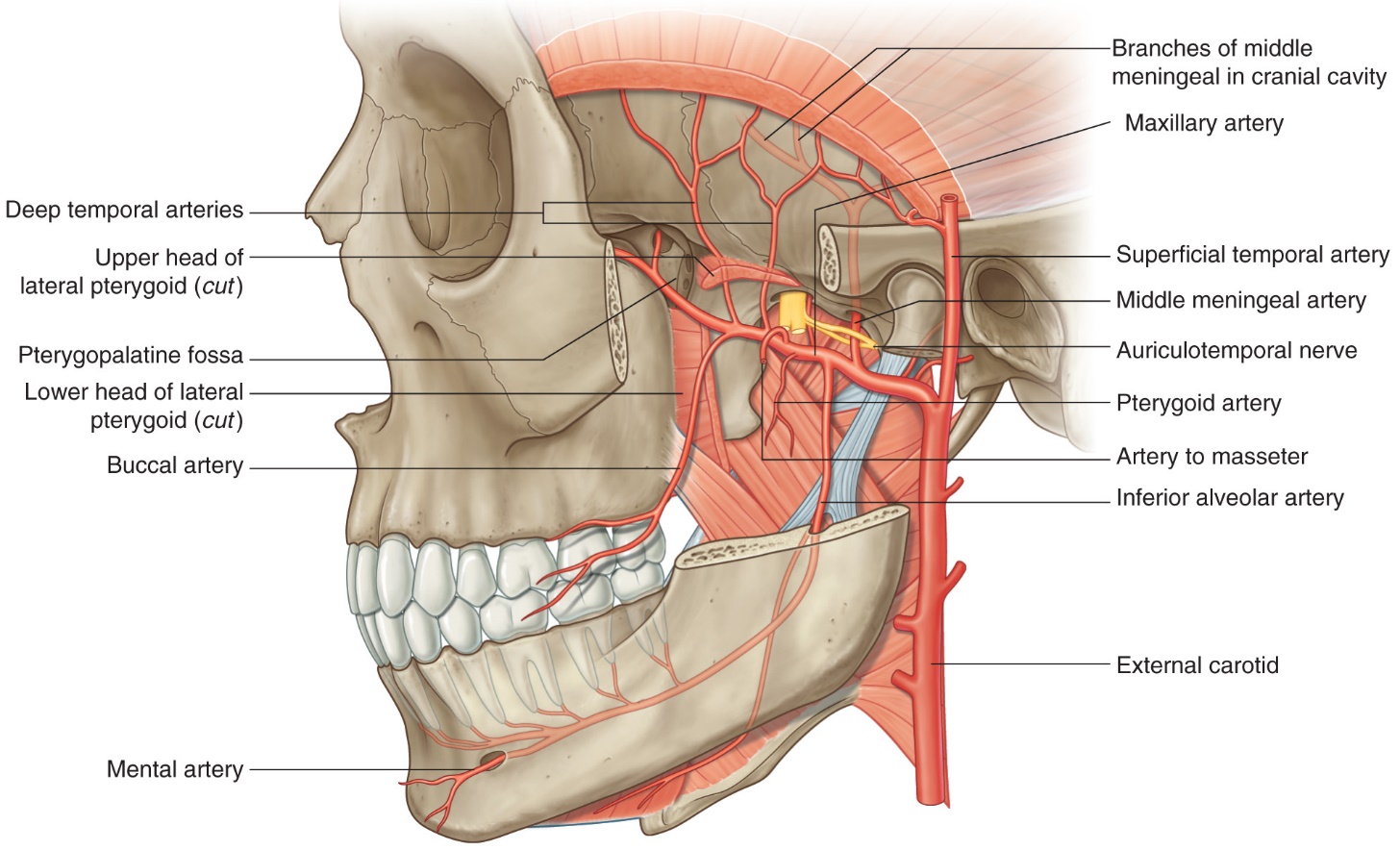
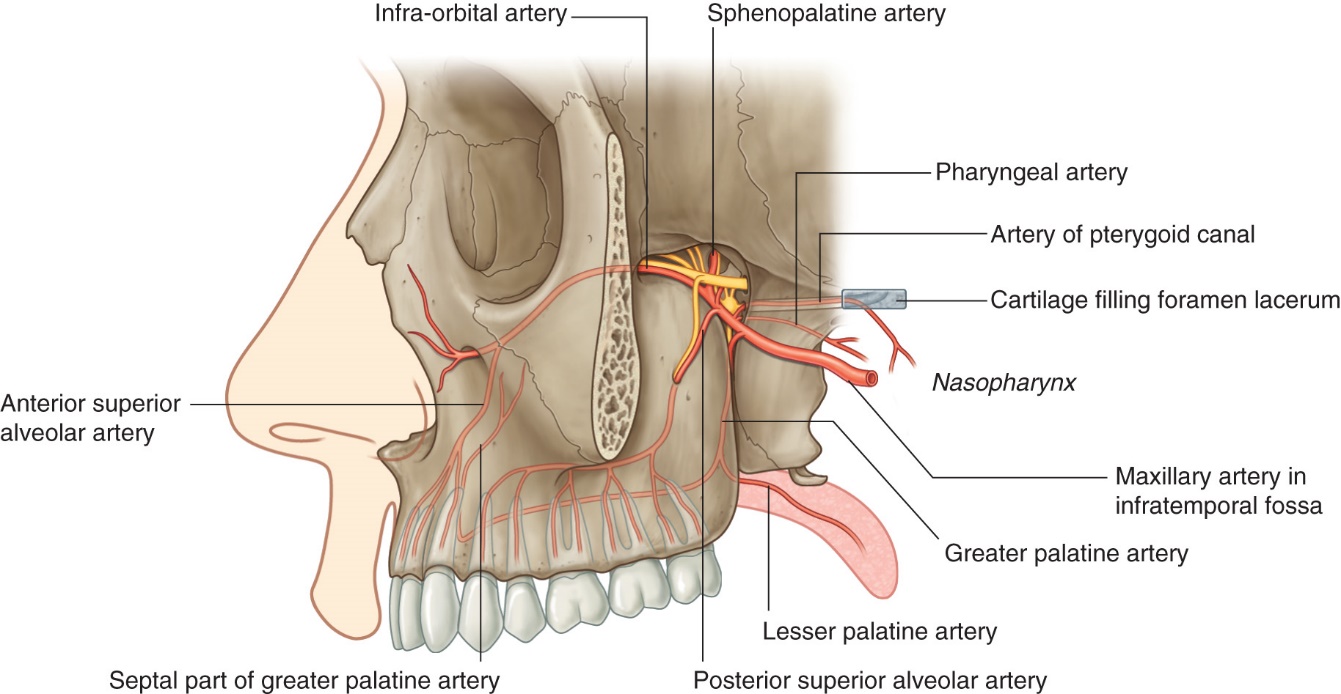
The maxillary artery (Figure 30.9) enters the ITF deep to the condylar process of the mandible. Once in the ITF, it passes either superficial or deep to the lateral pterygoid muscle. You will need to do some cleaning to determine which is the case in your donor. If it passes deep, you won’t see much of the artery until you remove the lateral pterygoid (instructions on this are given later).
The distal part of the maxillary artery leaves the infratemporal fossa via the pterygomaxillary fissure and enters the pterygopalatine fossa (Figure 30.9).
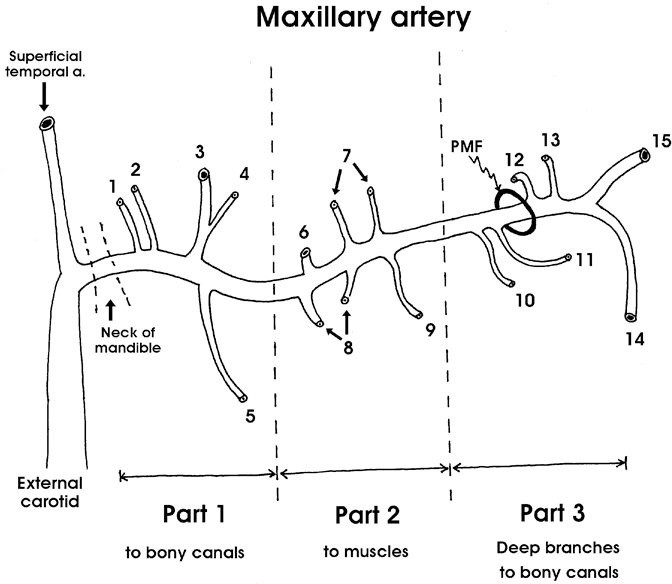
Dissection of the branches of the maxillary artery is difficult! Our goal is to trace it through the ITF to the pterygomaxillary fissure and try to identify several of its major branches. Figure 30.10 is a sketch that lists ALL the branches of the maxillary artery. We will seek out only a few of these today. Don’t sweat the small branches.
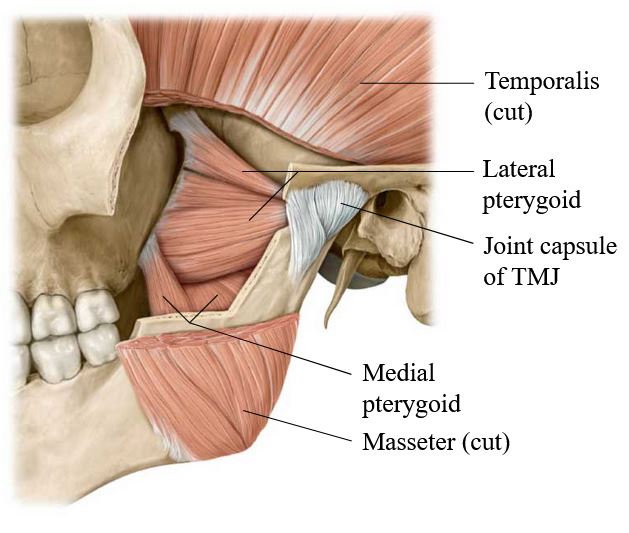
To better see the nerves and vessels in the infratemporal fossa, the lateral pterygoid muscle will be removed. Carefully remove the lateral pterygoid muscle in pieces with scissors and forceps.
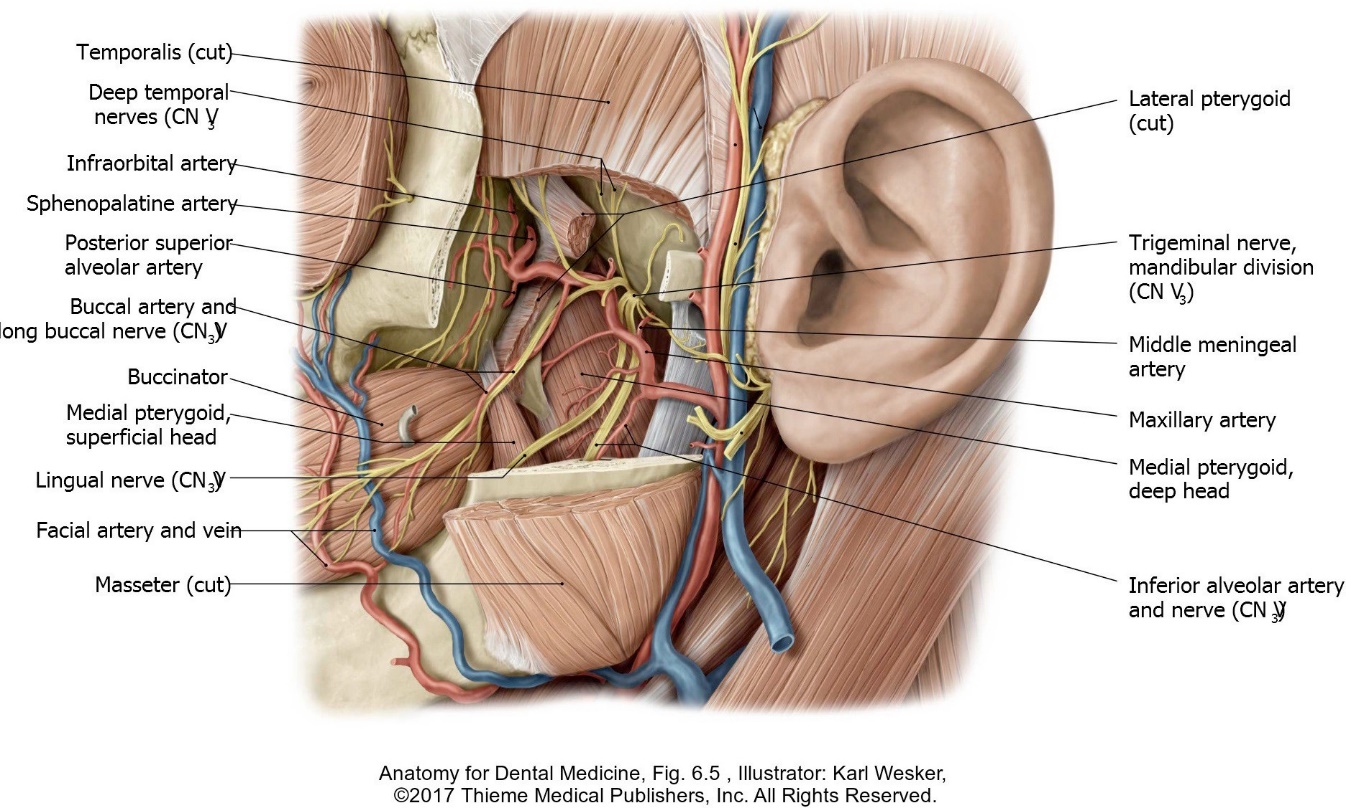
■Identify the buccal nerve passing between the two heads of the lateral pterygoid. Preserve this nerve as the muscle is removed.
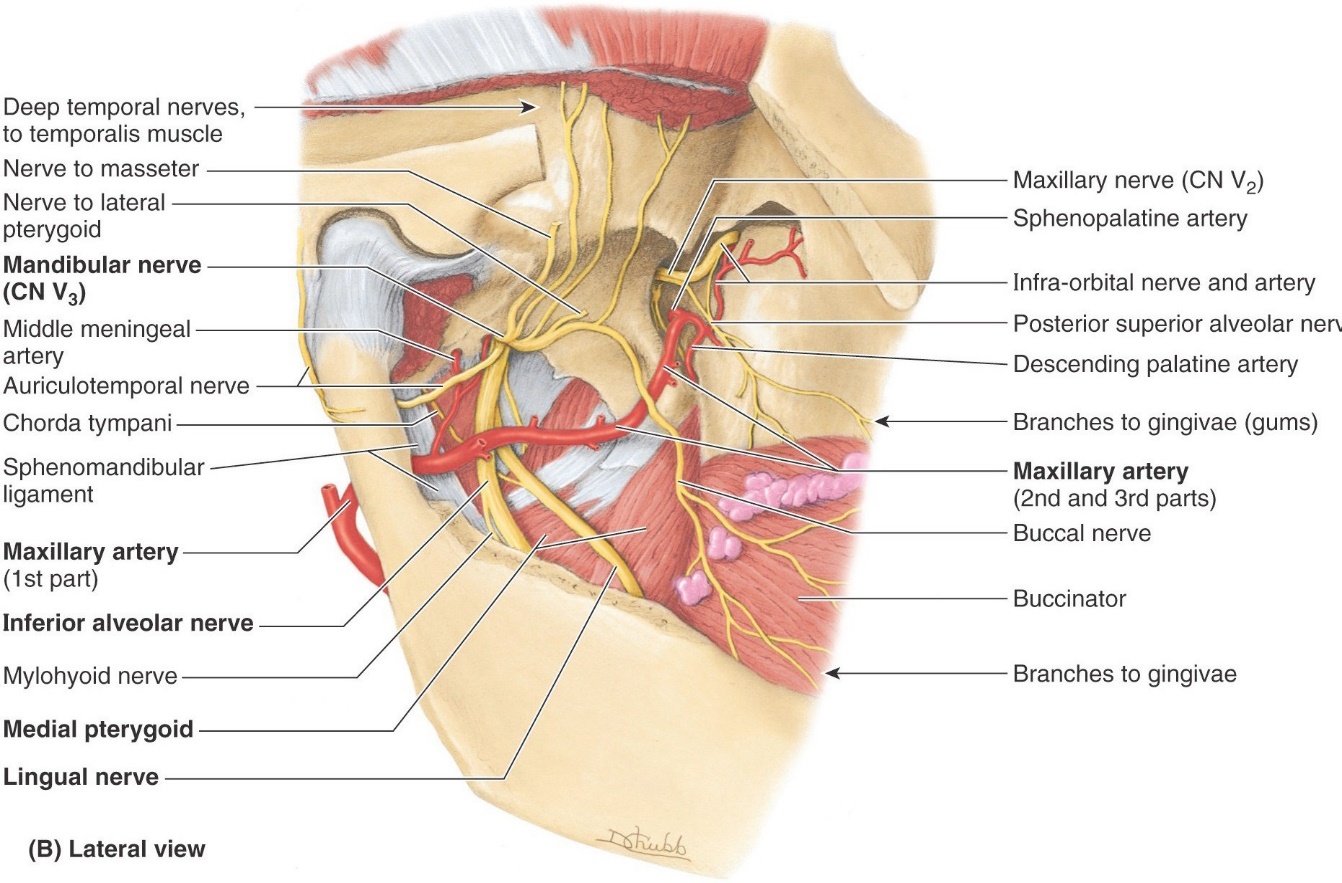
■Locate and clean the maxillary artery as you remove the lateral pterygoid. Look for these branches of the artery as you dissect (Figures 30.9 and 30.11):
■Middle meningeal artery. It exits through the roof of the ITF through which foramen? What is the function of the middle meningeal artery? What is its clinical importance in the case of skull fracture?
■Inferior alveolar artery: Accompanies the nerve of the same name.
■Deep temporal arteries: Ascend to the deep surface of the temporalis


■Make a vertical midline incision in the lip from the oral fissure to the tip of the chin. Cut away the lower lip from the mandible externally. Clean tissue from the body of the mandible.
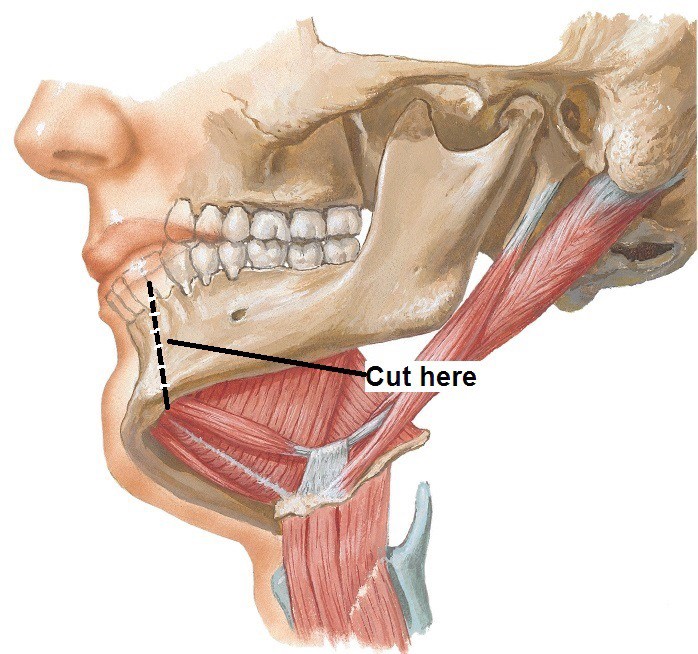
■Transect the mandible with an autopsy saw or hacksaw, off the midline a bit (Figure 30.15). Cut downward vertically between the incisor teeth. This will keep the geniohyoid and genioglossus muscles intact.
■With scissors detach the anterior belly of the digastric and mylohyoid muscles from the inferior surface of the mandible and reflect them down.
■Pull the mandible away from the head to apply traction, then reach into the oral cavity and use a scalpel or scissors to cut away the oral mucosa where it is attached to the lingual aspect of the lower gums.
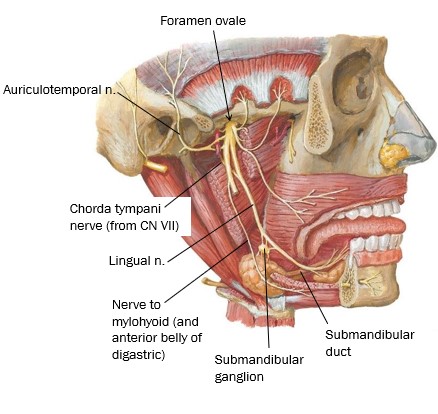
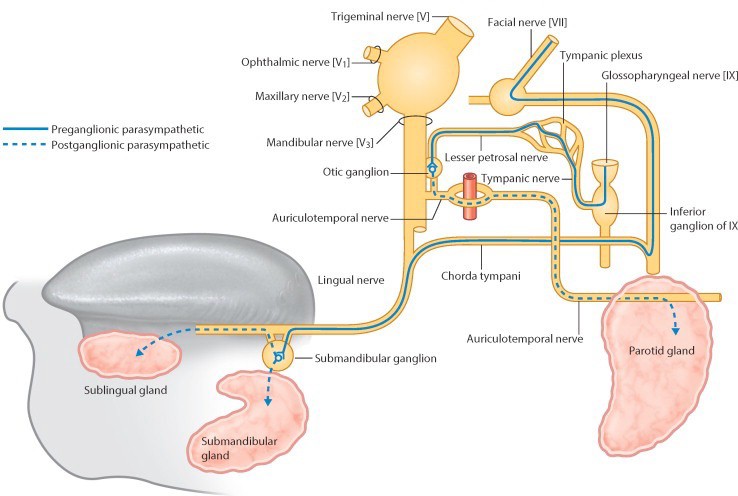
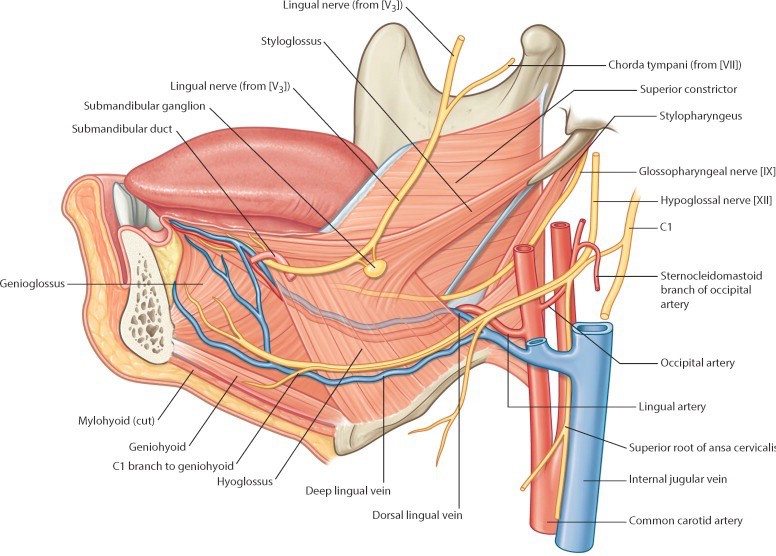
■Trace the lingual nerve forward from the ITF. Look for a wide spot as it curves below the tongue—this is the location of the submandibular ganglion (a parasympathetic ganglion). Cell bodies of post-ganglionic parasympathetic fibers that innervate the submandibular and sublingual glands are located here. Consult Figure 30.16.
■Trace the hypoglossal nerve forward from the neck to below the tongue.
Remember it can be found just inferior to the posterior belly of the digastric and styloyhyoid muscles.
■Identify the inferior alveolar nerve and trace it distally (it has likely been cut, so only a stump may remain). Just before it enters the mandibular foramen it gives off a thin motor branch to the neck called the nerve to mylohyoid and anterior belly of digastric, which runs inferiorly on the medial side of the mandible. See Figure 30.16.
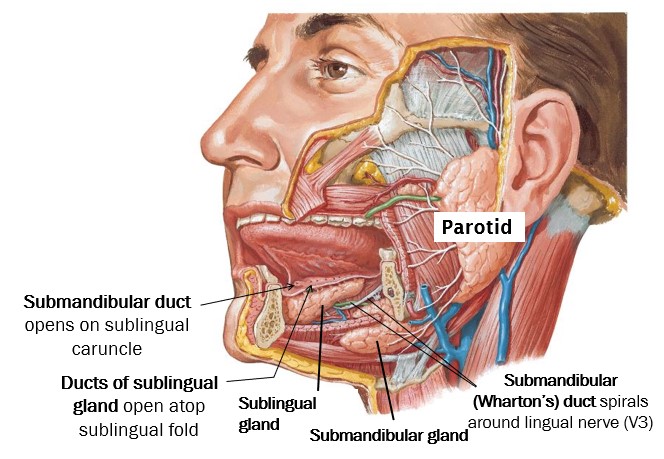
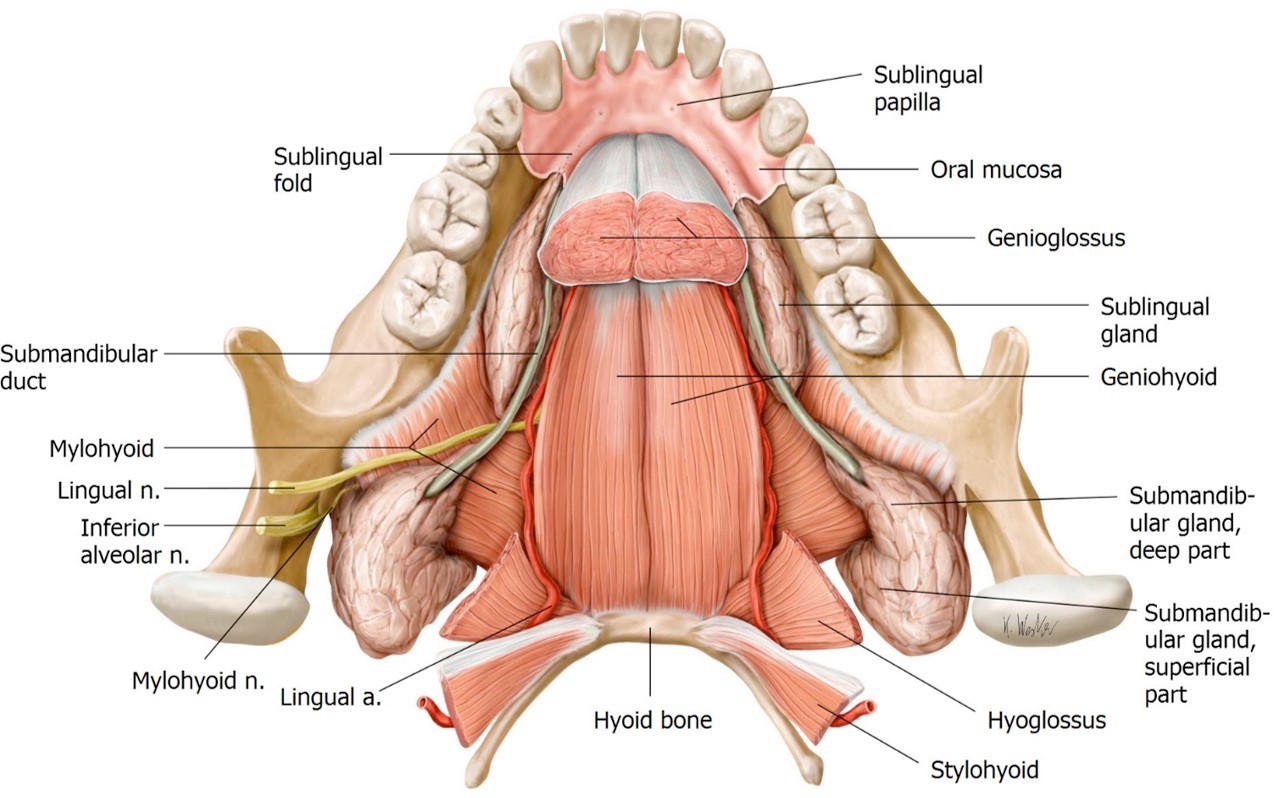
■Clean the submandibular gland and the facial artery twisting around it. Note that the submandibular gland has a large superficial part (external to mylohyoid in the submandibular triangle) & a small deep part (above the mylohyoid muscle in the floor of the mouth). The 2 parts of the gland connect by curling around the posterior “free edge” of the mylohyoid, like the letter “U”. See Figure 30.17.
■Clean the sublingual gland, located just behind the chin (Figure 30.17). It is a small thin gland. At first, you may not recognize it since it may not appear very glandular and can be pale in appearance.
■Starting at the deep part of the submandibular gland and using the lingual nerve as a landmark, search for the flat, thin, white duct of the submandibular gland (Wharton’s duct). It can be tricky to find. See Figures 30.17 and 30.18.
Stylo-muscles
With a finger, palpate the styloid process by probing deeply, posterior to the infratemporal fossa and anterior to the ear.
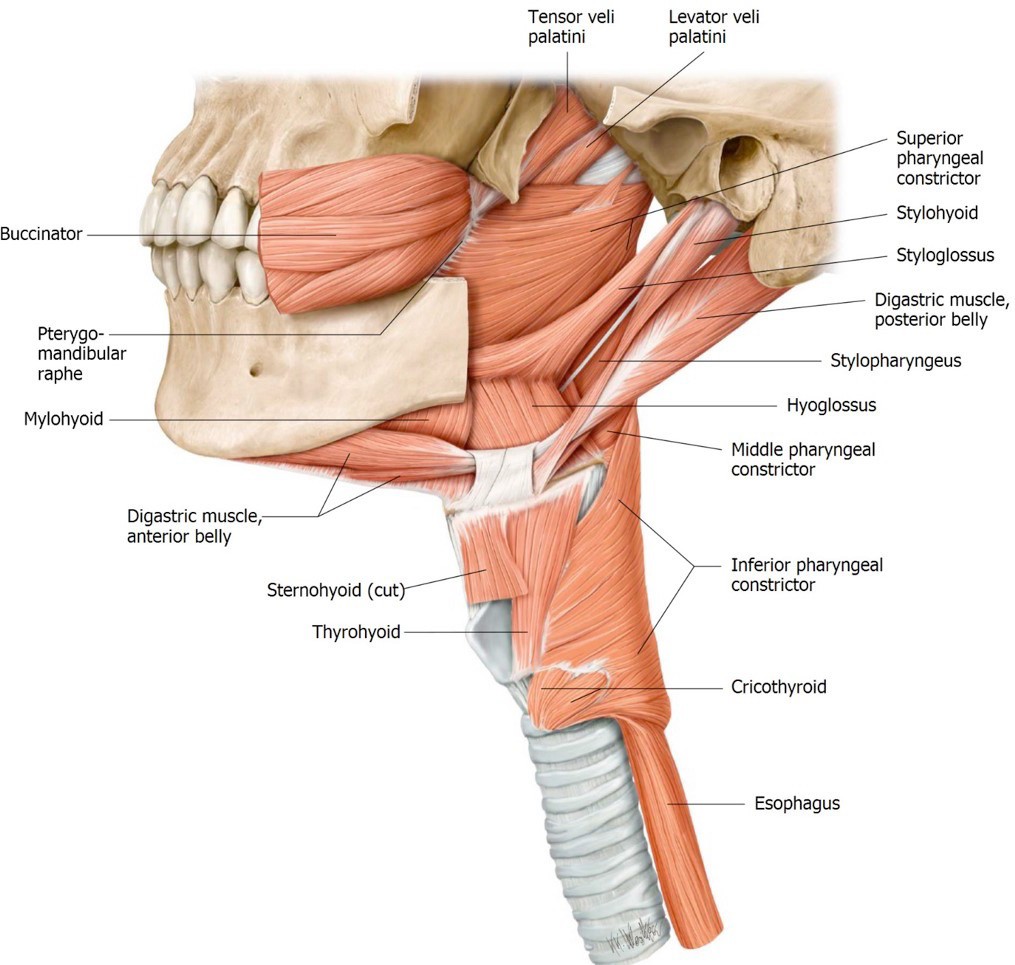
Starting at the styloid process, clean and trace the stylohyoid, styloglossus, and stylopharyngeus muscles. They can be identified by their orientations and destinations. See Figure 30.20.
■The stylohyoid is intimately associated with the posterior belly of the digastric.
■The styloglossus blends with the hyoglossus in the root of the tongue.
■The stylopharyngeus is the deepest since it descends to the pharynx.
■The glossopharyngeal nerve is located on the posterior border of the stylopharyngeus (the only muscle that CN IX supplies!). It is not very large and a bit difficult to identify.