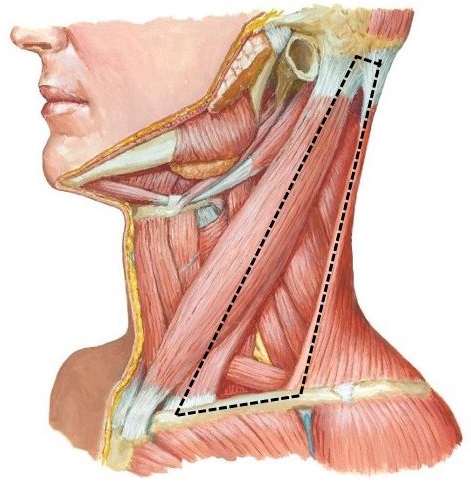
Let’s begin with a geometry lesson. Identify the boundaries of the posterior triangle of the neck (Figure 29.1).
After you get the “lay of the land” in terms of landmarks, clean and identify the external jugular vein on the outer surface of the sternocleidomastoid (SCM). See Figure 29.2.
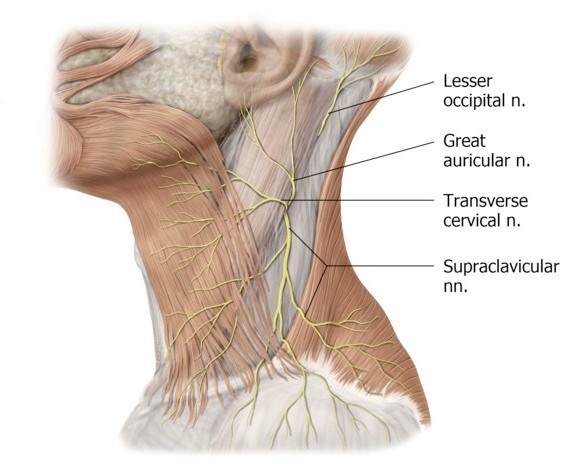
The cutaneous nerves of the neck emerge along the posterior border of the sternocleidomastoid at a common location = the midpoint between the mastoid process of the temporal bone (superiorly) and the sternum and clavicle (inferiorly). This spot is known as Erb’s point (Nerve point of the neck). See Figure 29.3. The nerves that emerge at Erb’s point pierce the investing fascia and enter the superficial fascia. These are all cutaneous nerves.
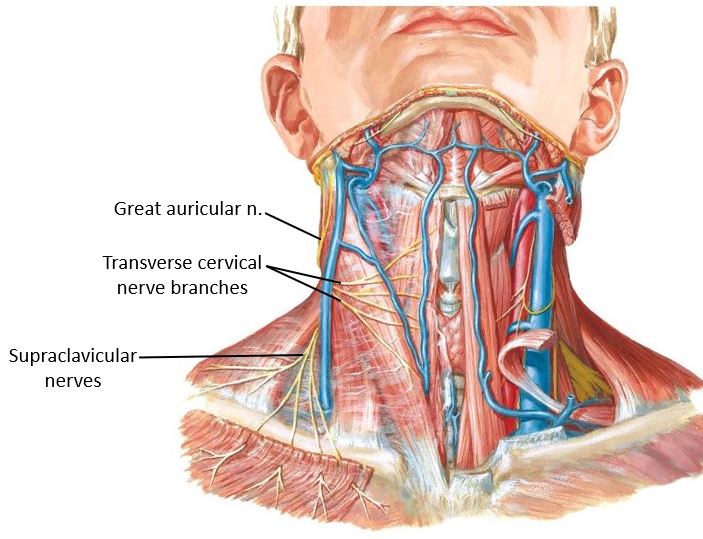
The sensory nerves of the neck are the lesser occipital, great auricular, transverse cervical, and supraclavicular nerves.
These sensory nerves, along with the ansa cervicalis (motor only) and phrenic nerve (mixed—motor and sensory), are derived from the cervical plexus (ventral rami of spinal nerves C-1 to C-4).
The boundaries of the posterior triangle are now visible.
The tough investing fascia is the “roof” over the posterior triangle. Use the open/close scissors technique with patience to do your best to remove it.
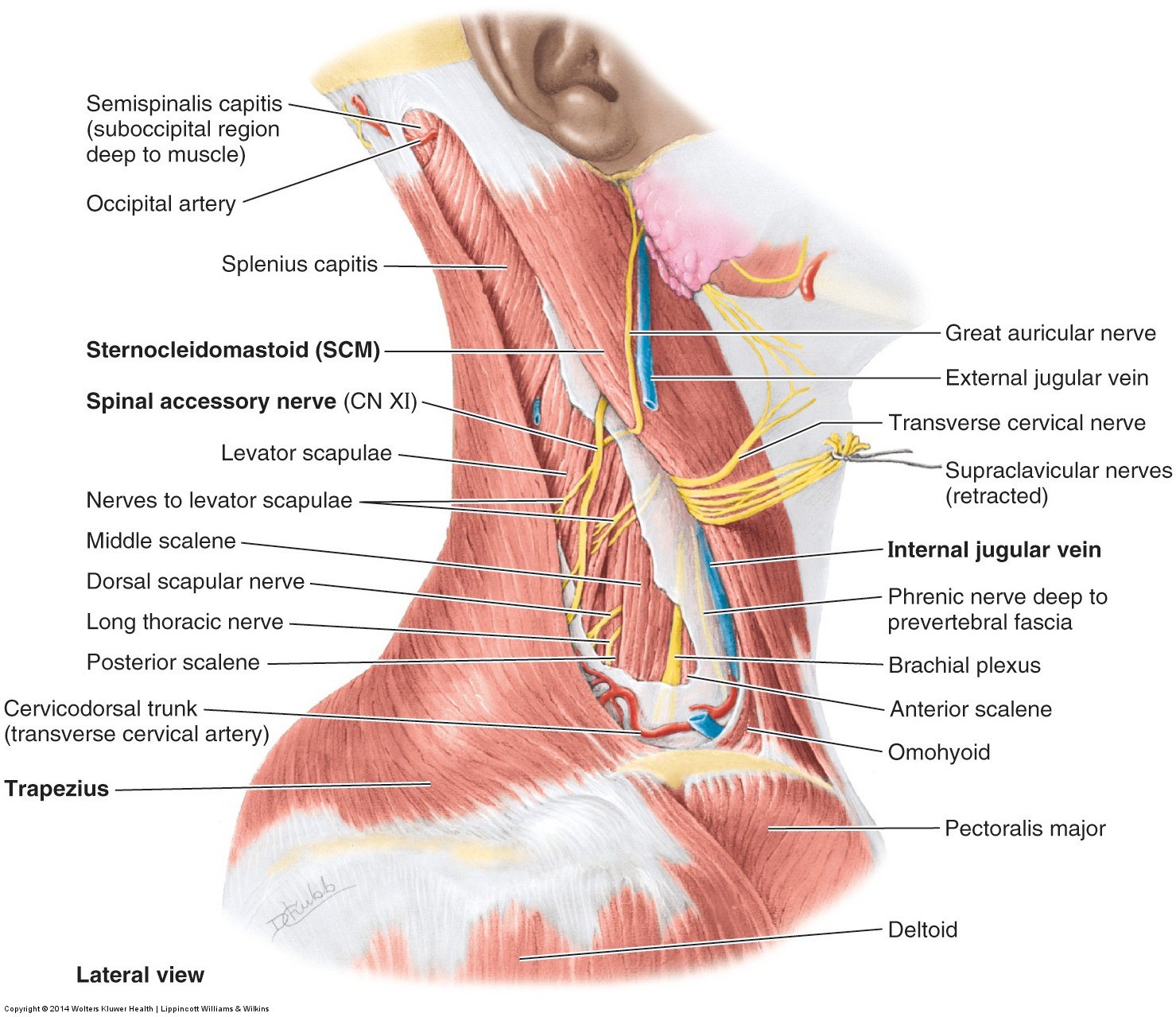
■The spinal accessory nerve enters the deep surface of sternocleidomastoid up high, just below the skull. After innervating the SCM, the spinal accessory leaves the posterior border of the muscle and crosses the posterior triangle.
■Find the spinal accessory nerve (CN XI) entering the deep surface of the reflected SCM (last lab)—trace it as it leaves the SCM and heads across the posterior triangle to the anterior border of the trapezius. It is tortuous as it crosses the neck. It travels through the posterior triangle along an imaginary line drawn between the ear lobe and acromion (summit of shoulder). See Figure 29.4.
Identify, from anterior to posterior:
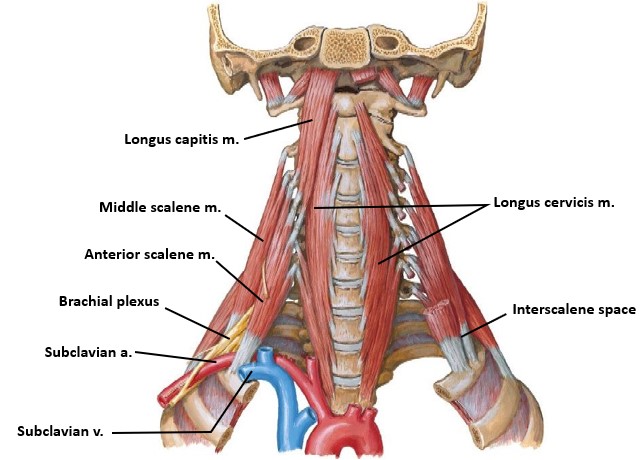
■Anterior and middle scalene muscles
■Phrenic nerve on the surface of the anterior scalene muscle
Identify the “interscalene space” between the anterior and middle scalene muscles, and the first rib. The brachial plexus and subclavian artery squeeze through this space. See Figure 29.5.
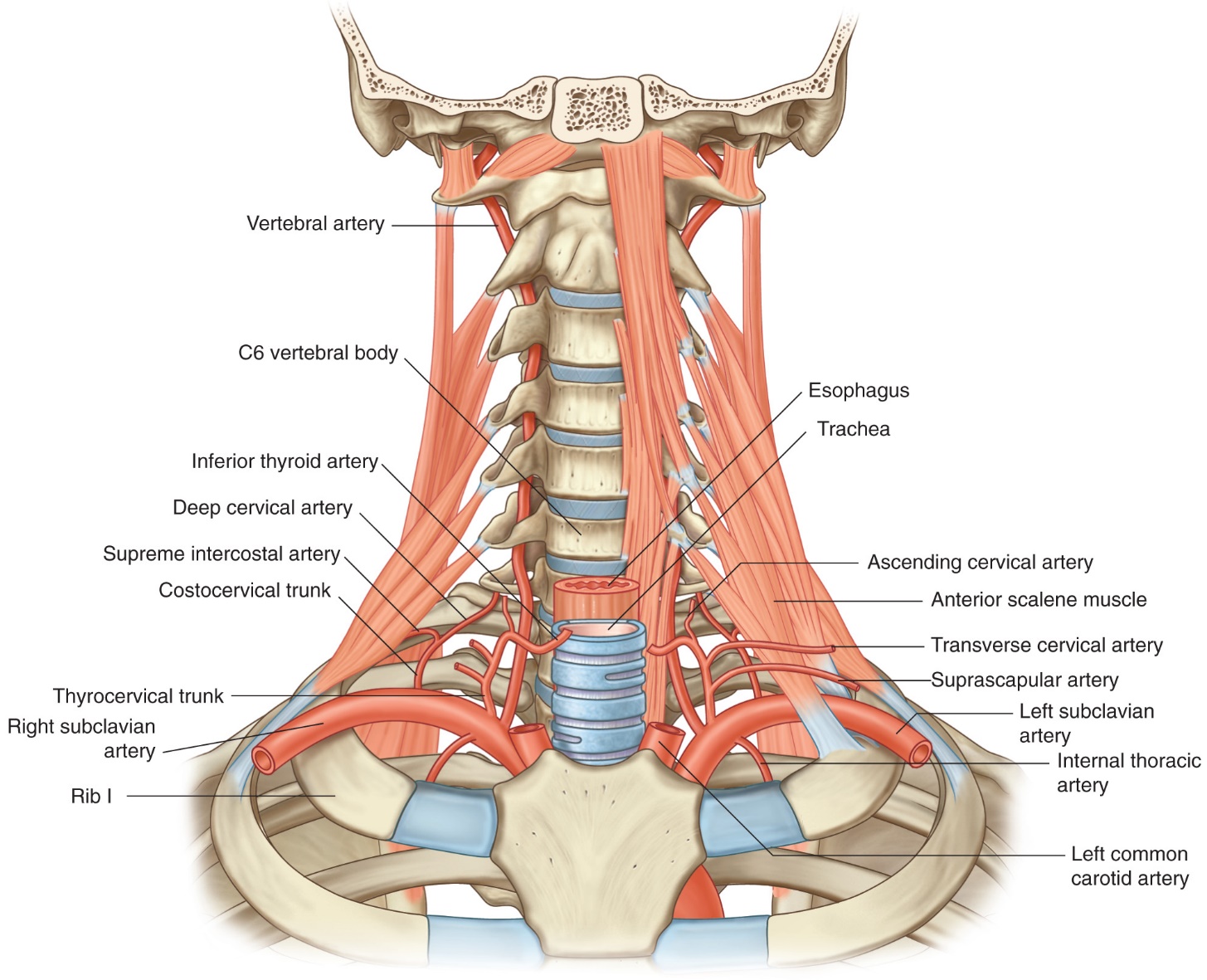
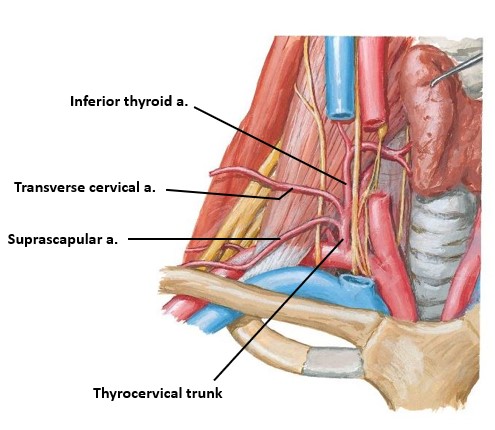
The subclavian artery has 3 parts (based on its relationship to the anterior scalene muscle). The major branches of the subclavian artery are all from Part 1. See Figure 29.7.
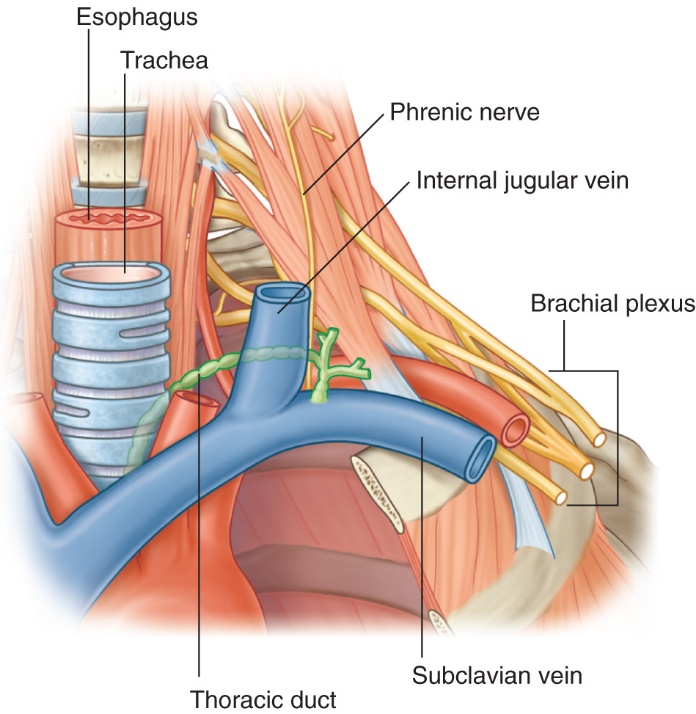
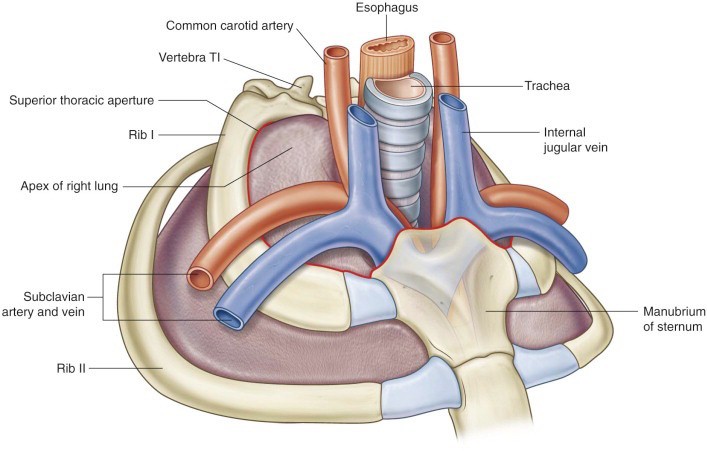
Identify the esophagus as it passes through the superior thoracic aperture. Remember that the thoracic duct is posterior to the esophagus in the mediastinum. The thoracic duct inclines to the left as it passes through the superior thoracic aperture. Clean along the left edge of the esophagus at the root of the neck to find the thoracic duct and follow it to the left venous angle. See Figure 29.10.
It is easy to be fooled here because the thoracic duct may be filled with blood and resemble a vein. It often has a “beaded” appearance and may be quite delicate, so clean it with care! The vertebral vein is also in the area (= a tributary of the brachiocephalic vein) and can be confused with the thoracic duct. It descends from the neck.
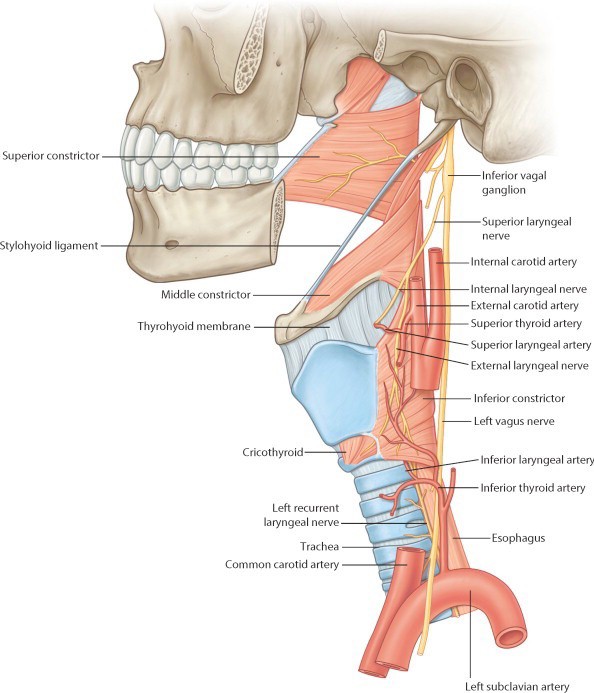
Trace the internal laryngeal nerve backwards from the thyrohyoid membrane—if you are super skilled you may find the thin external laryngeal nerve descending to the cricothyroid muscle. The external laryngeal is the other branch of the superior laryngeal nerve. It accompanies the superior thyroid artery. See Figure 29.12.
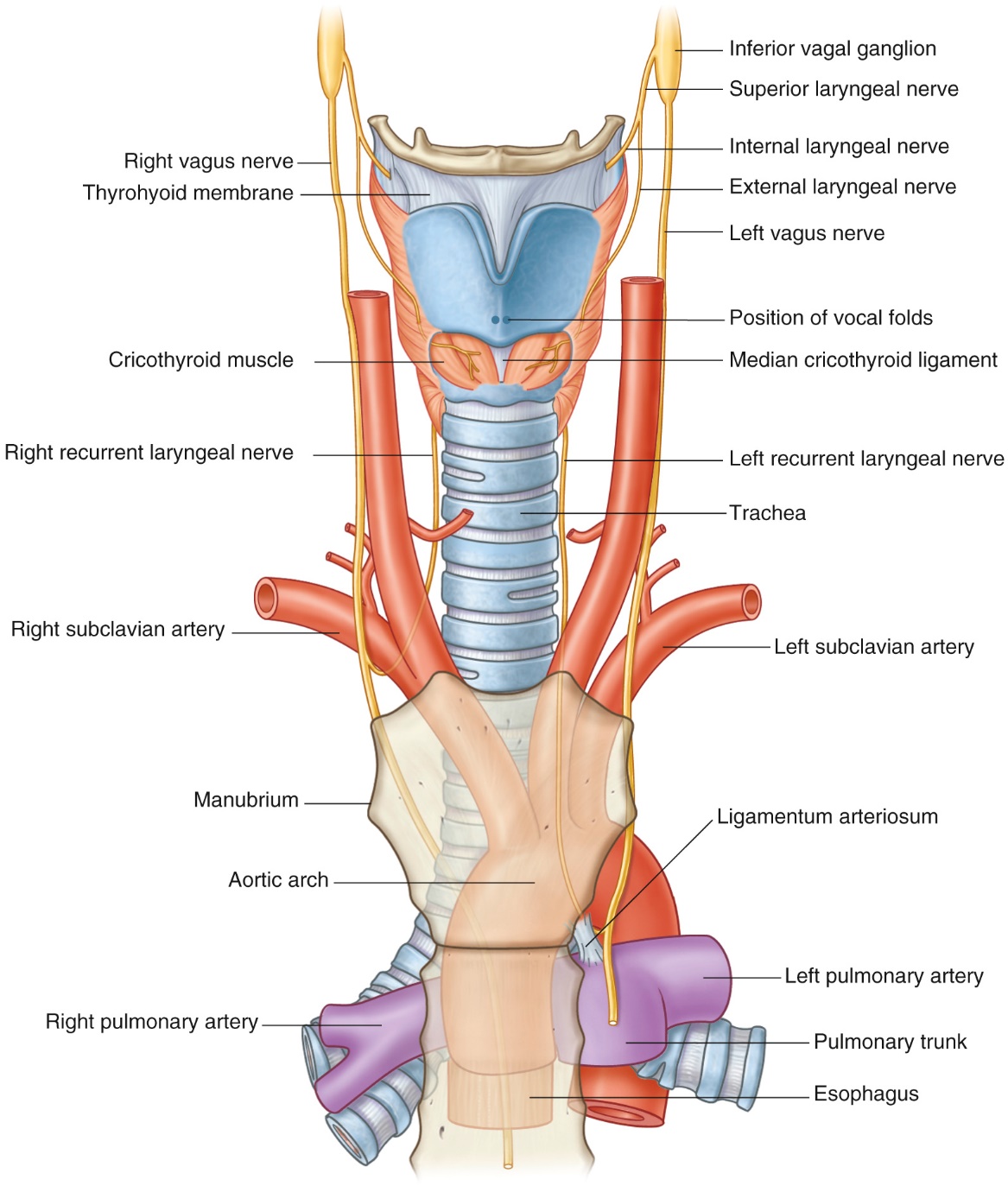
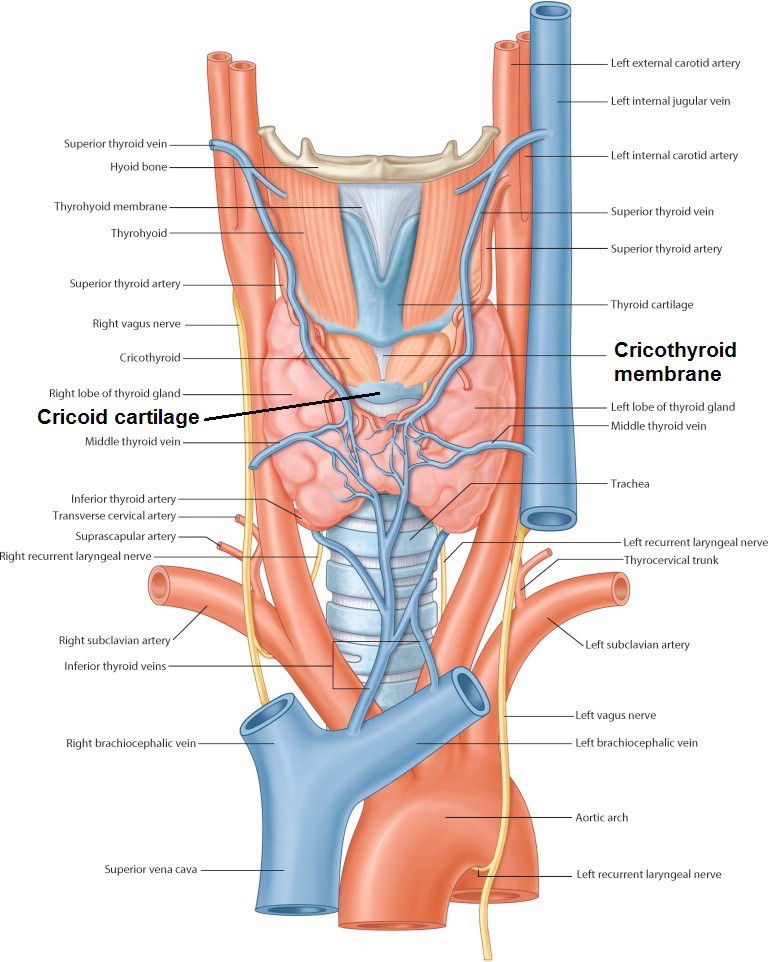
Find the recurrent laryngeal nerves ascending in the tracheo-esophageal grooves (left one loops under the arch of the aorta and the right one recurs around the right subclavian artery). The recurrent laryngeal nerves supply the mucosa of the lower half of the larynx and all intrinsic muscles of the larynx (except the cricothyroid). See Figure 29.13.
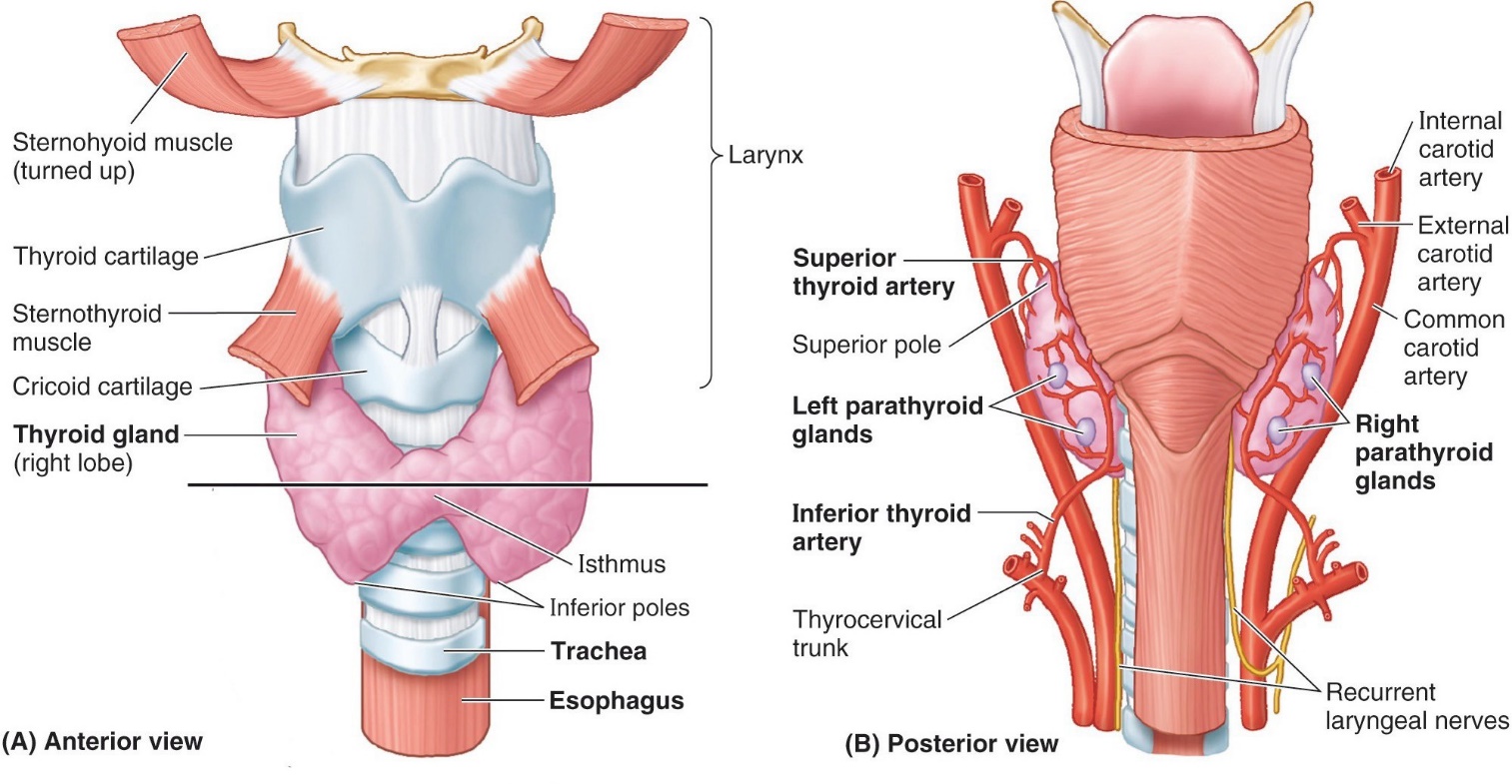
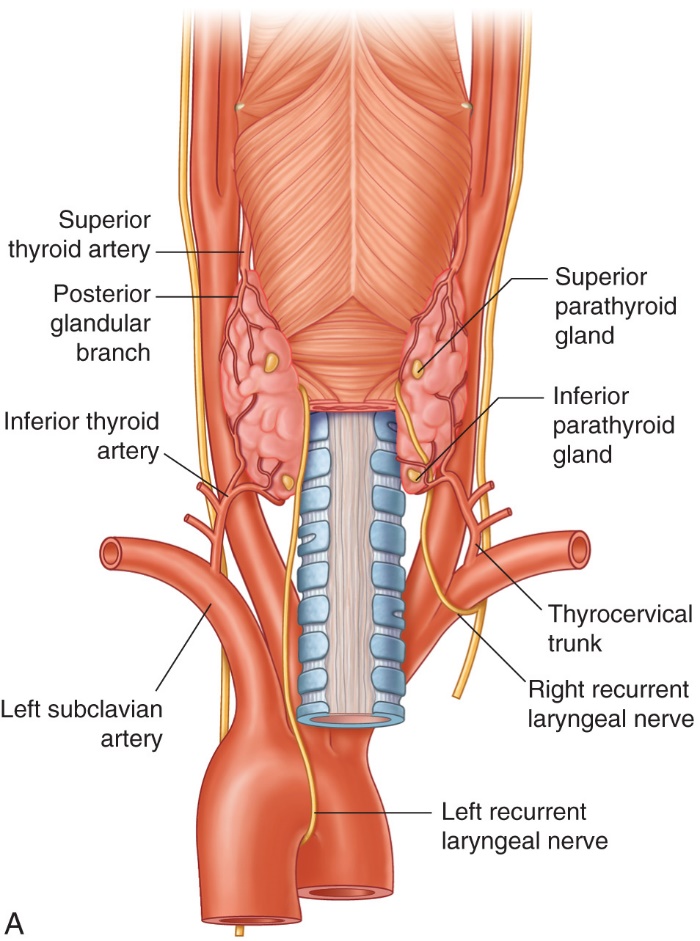
Parathyroid glands are said to relate to the posterior surfaces of the thyroid lobes, but their locations can be variable. These are tough to find in cadavers because of their size, color. and variability (due to embryology!).
The best bet is to look for the superior parathyroid glands behind the superior poles of the thyroid lobes, embedded in the capsule of the thyroid. See Figure 29.15. The superior parathyroid glands are less variable in their locations.