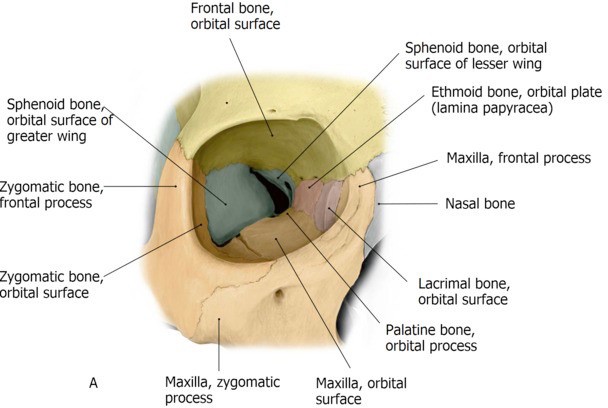
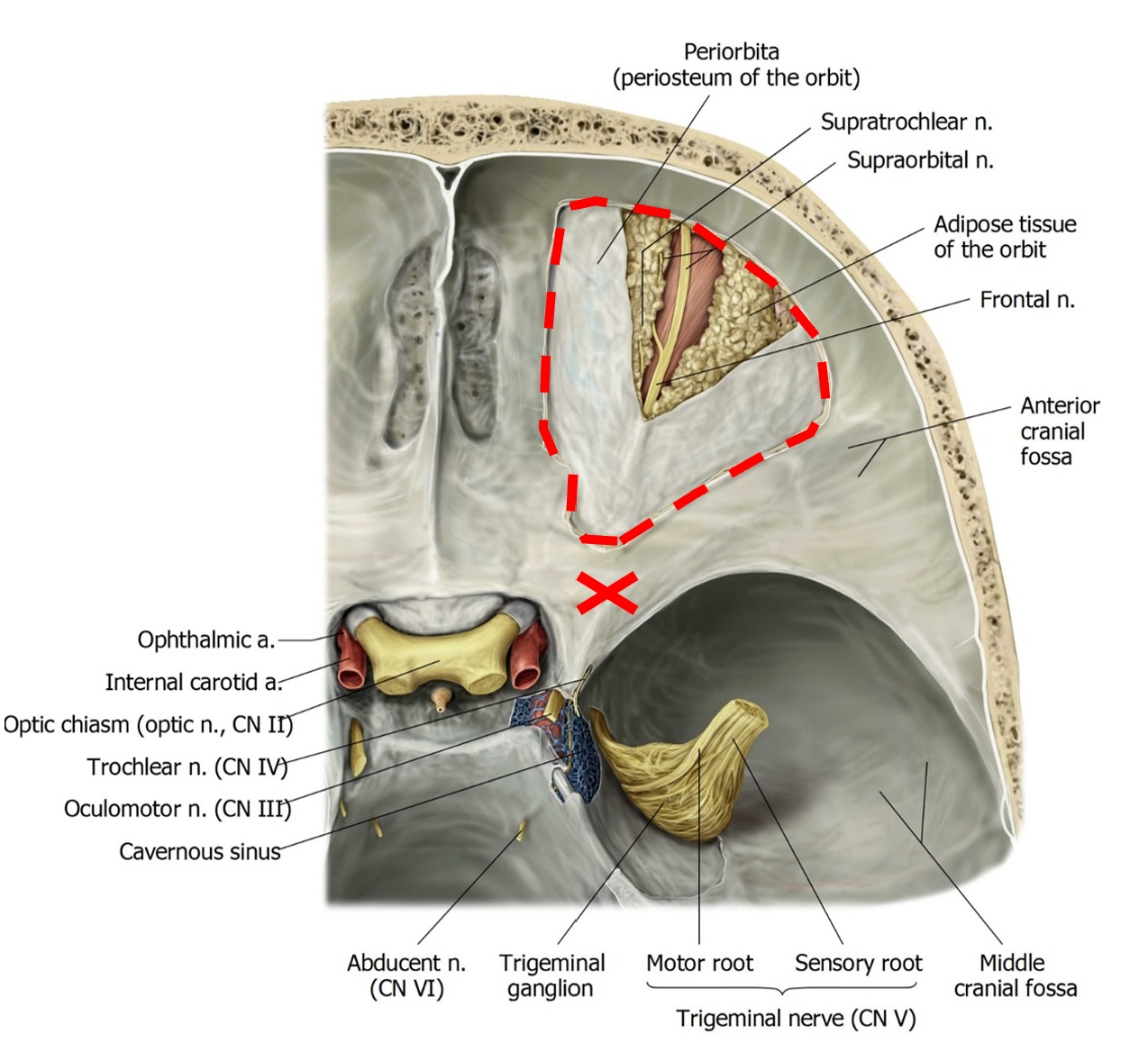
Now chip away the apex of the orbit by removing the lesser wing of the sphenoid bone.
The cone-shaped orbit is now open from above, but it is covered by the periorbita (a layer of periosteum).
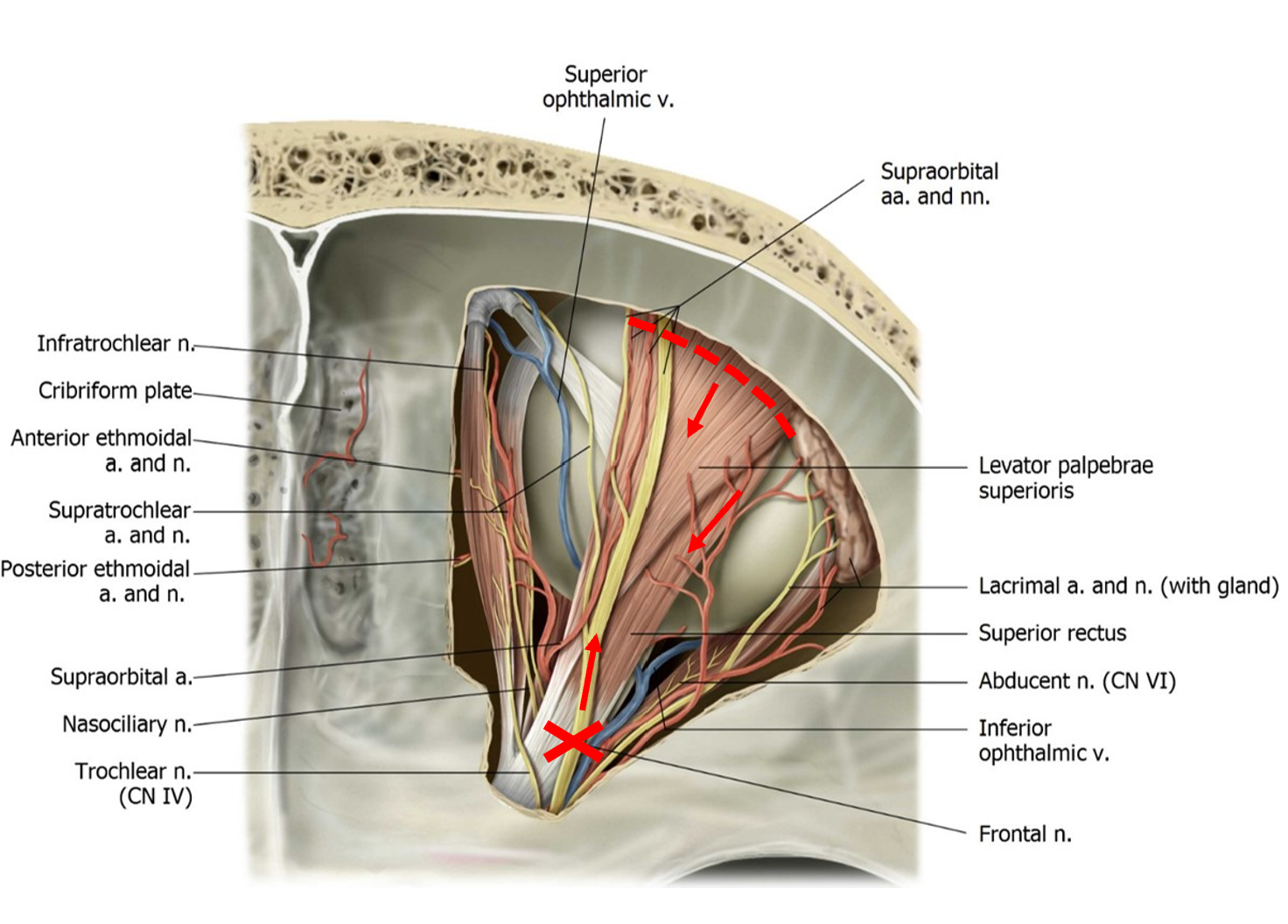
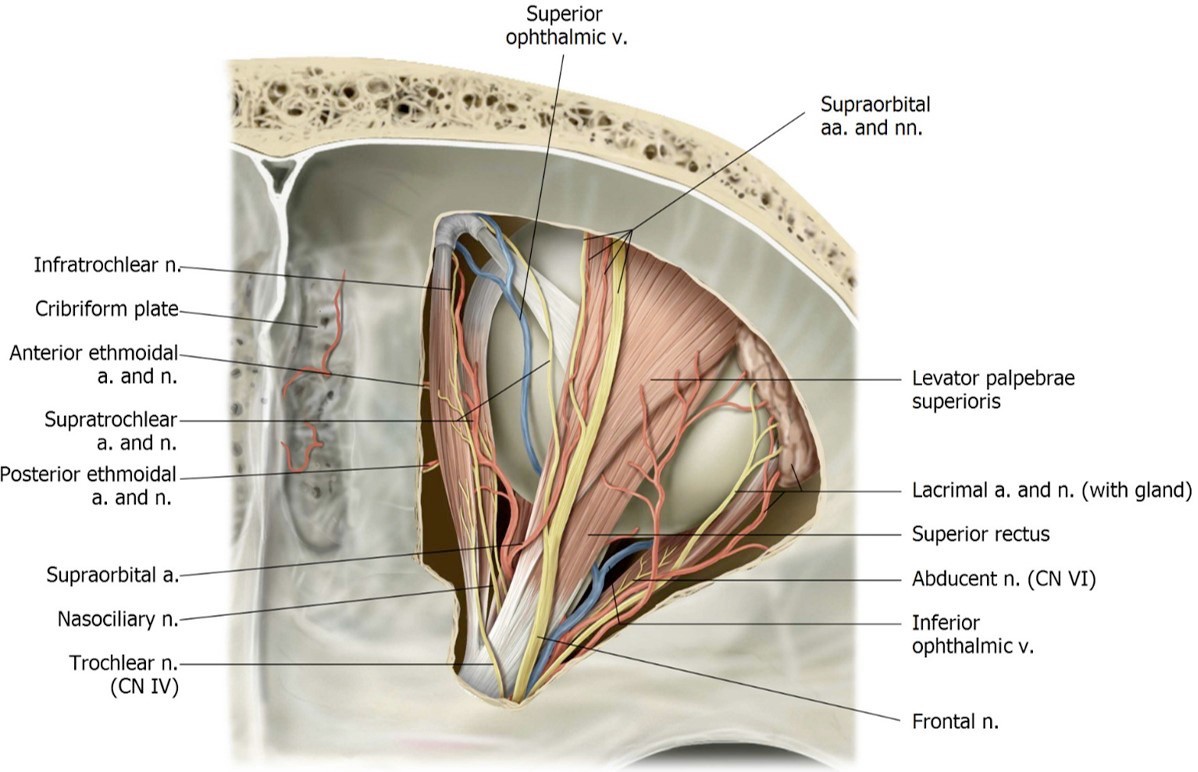
You should see the large flat frontal nerve just deep to the periorbita. Use scissors to carefully cut away the periorbita.
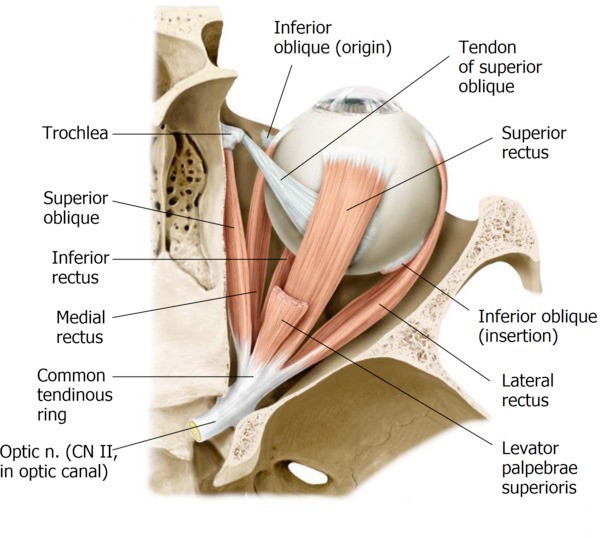
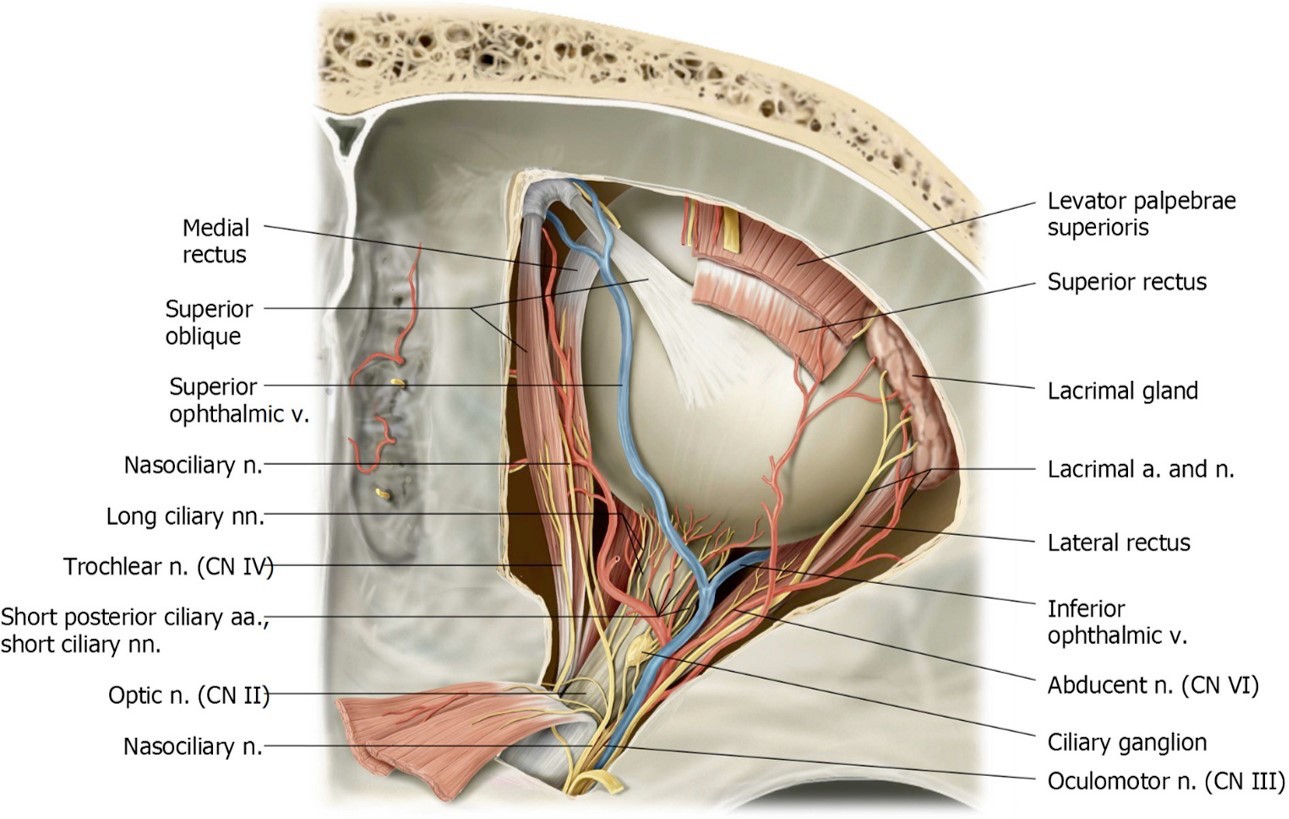
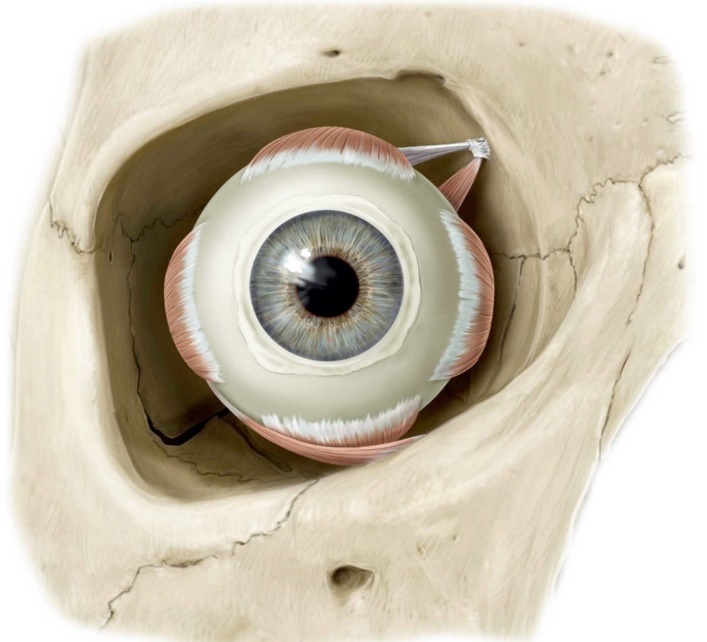
Below and parallel to the superior oblique, locate the medial rectus muscle. Traveling along the lateral wall of the orbit, locate the lateral rectus muscle.
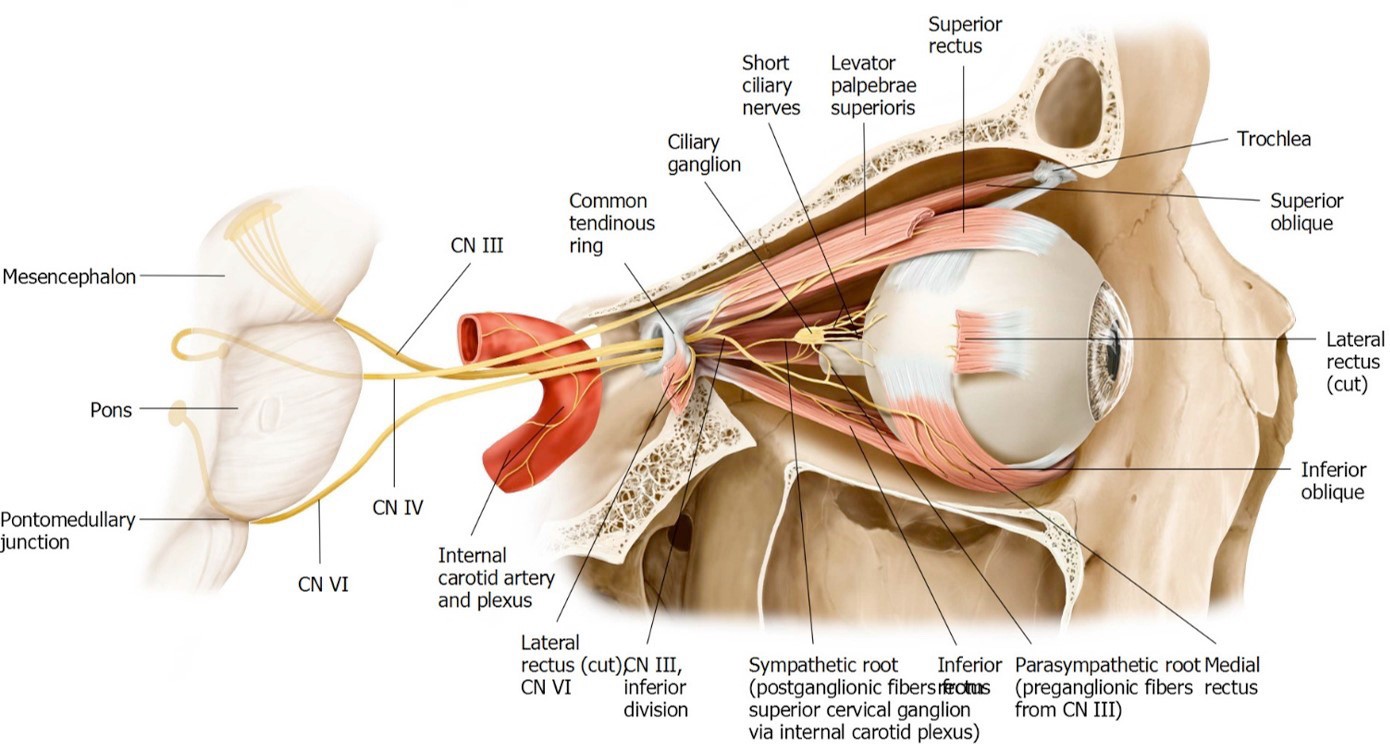
The other two extra-ocular muscles, the inferior rectus and inferior oblique, are on the floor of the orbit and can’t be seen from this view.