Test your knowledge!
Which muscles produce the facial expressions shown here? (Tap for answers.)
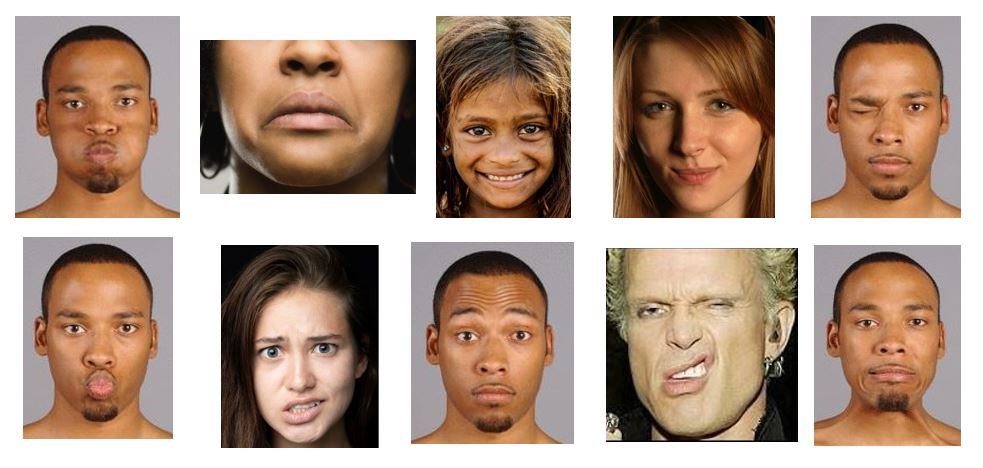
Test your knowledge!
Which muscles produce the facial expressions shown here?
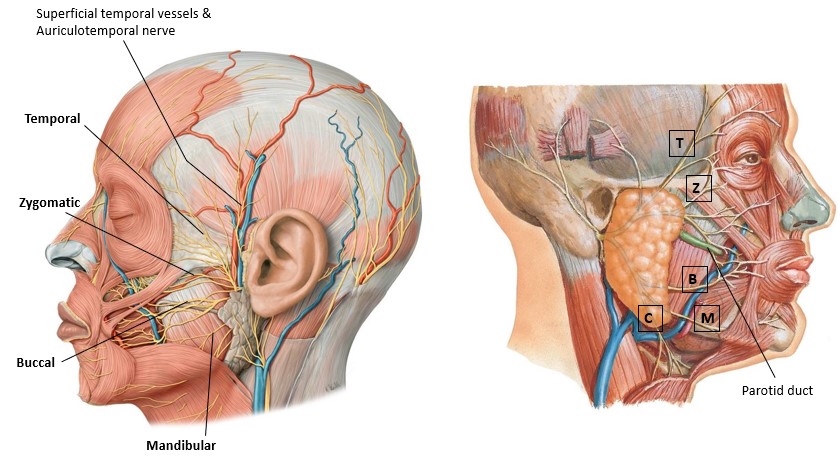
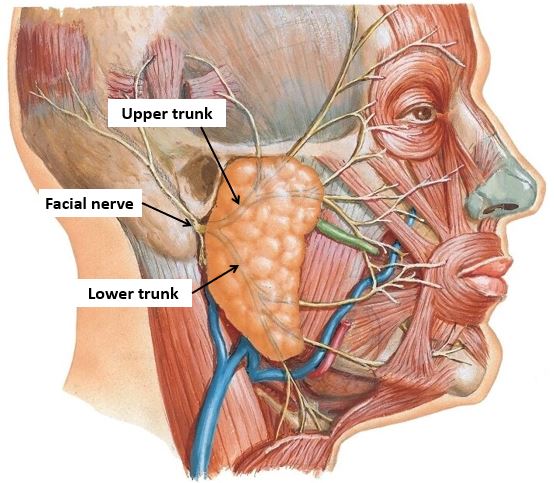
■The facial nerve emerges from the skull through the stylomastoid foramen, then enters the parotid gland. It typically divides into two trunks within the gland.
■From the upper trunk arise temporal and zygomatic branches
■From the lower trunk arise buccal, mandibular, and cervical branches.
Let’s find the facial nerve within the parotid gland using this method:
■First, locate the zygomatic and buccal branches above and below the parotid duct, anterior to the gland. Dissect them back to the gland, then remove pieces of the gland with forceps and scissors and follow the branches into the gland until you reach the trunks of the nerve. Follow the upper and lower trunks posteriorly to where they merge: this is the facial nerve, entering the parotid gland from the stylomastoid foramen.
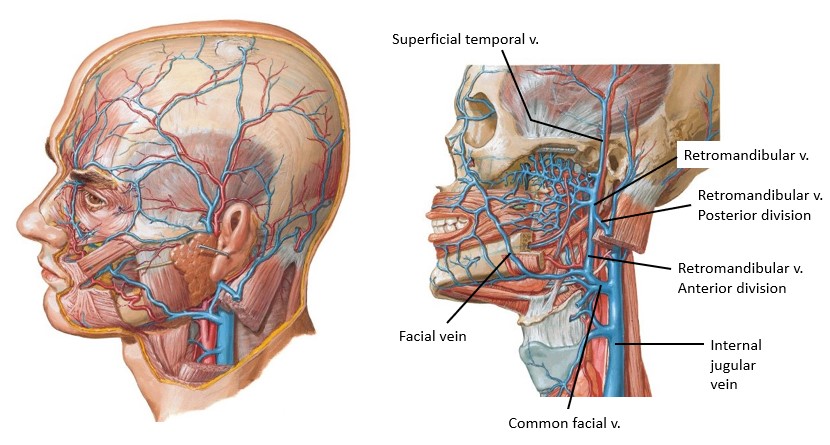
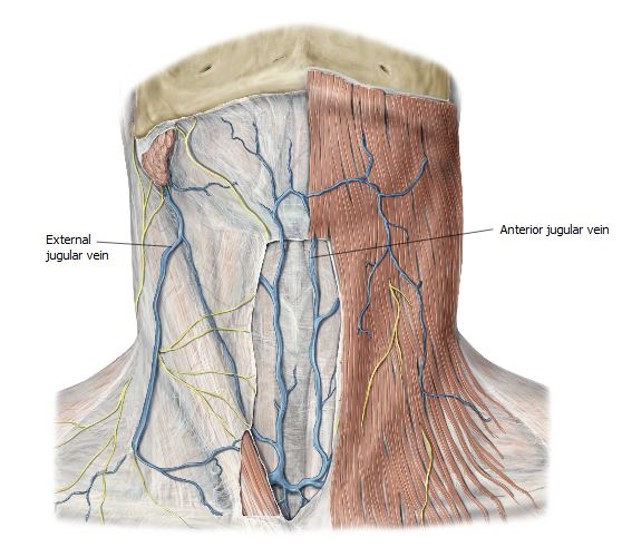
■This vein is formed by the union of the superficial temporal vein (from the scalp) and maxillary vein (from the infratemporal fossa—deep to the mandible). The veins merge within the parotid gland.
Best bet: Locate the superficial temporal vein in the lower scalp and trace it down into the parotid. Remove parotid tissue as you clean the vein from superior to inferior.