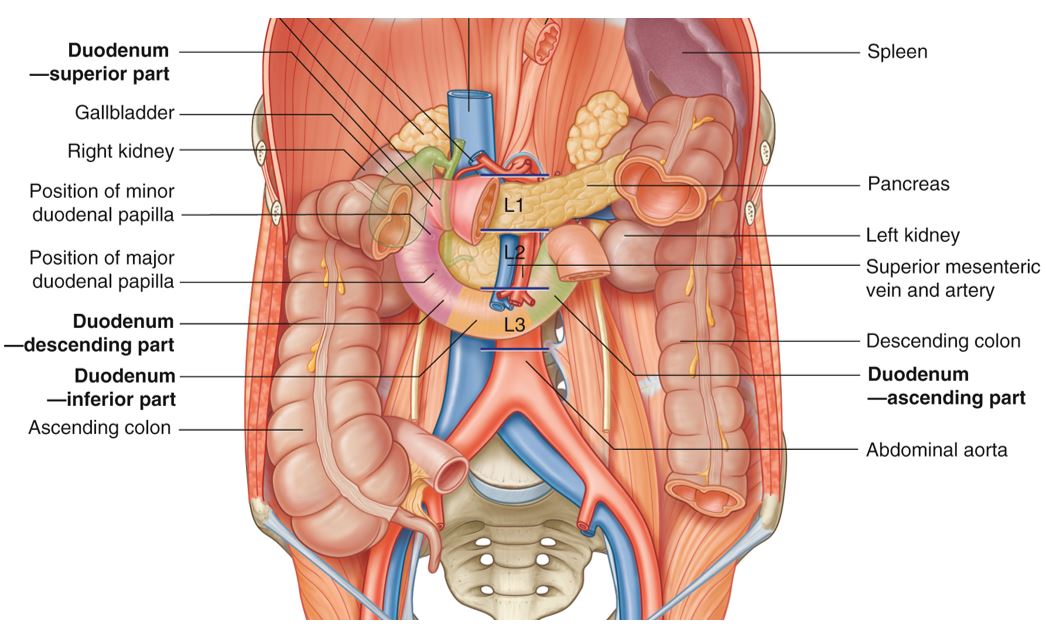
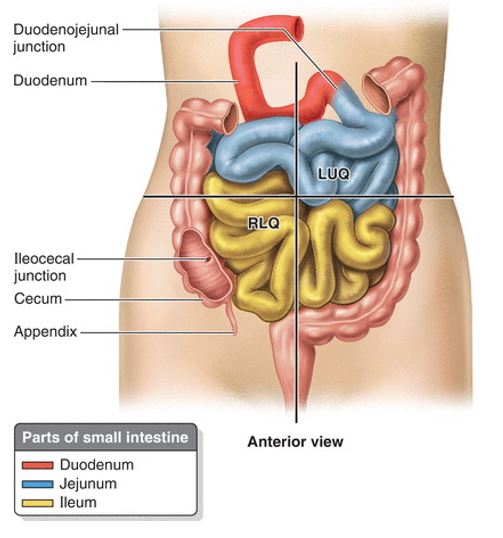
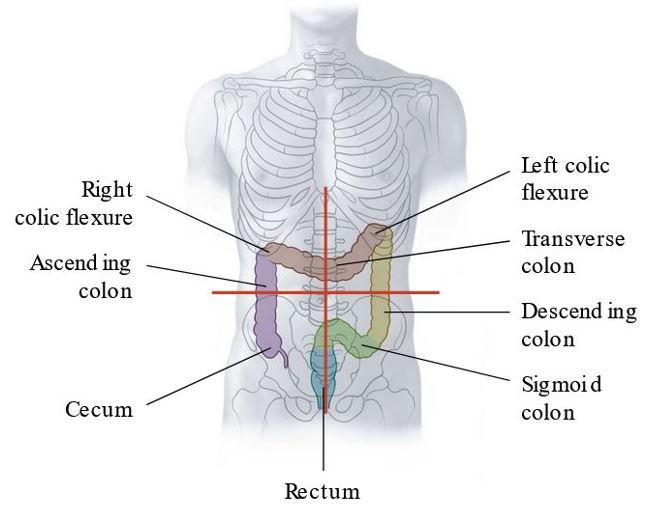
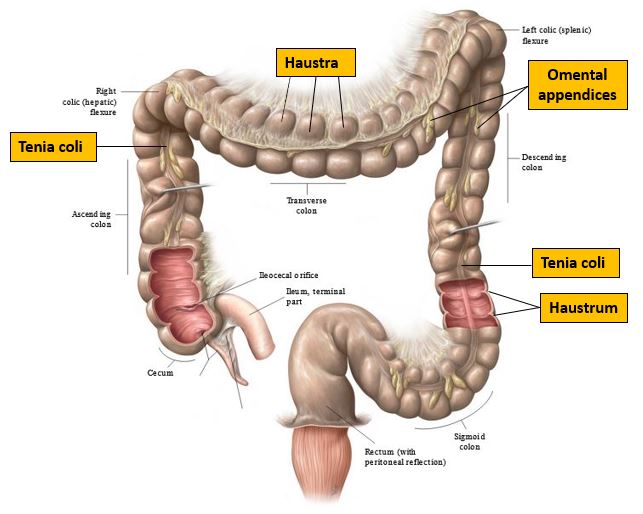
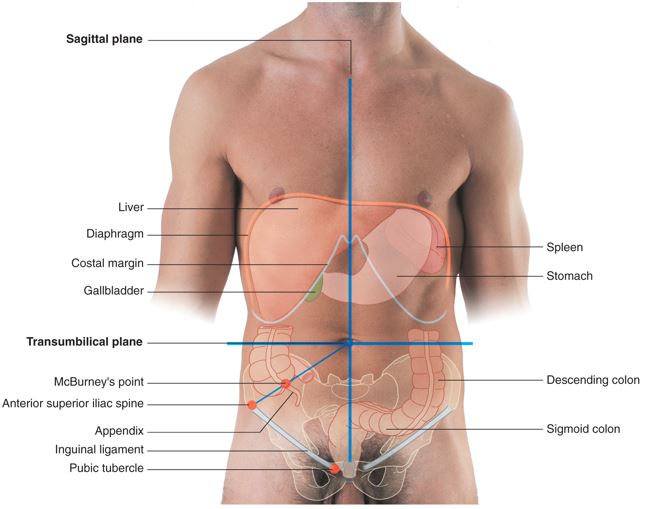
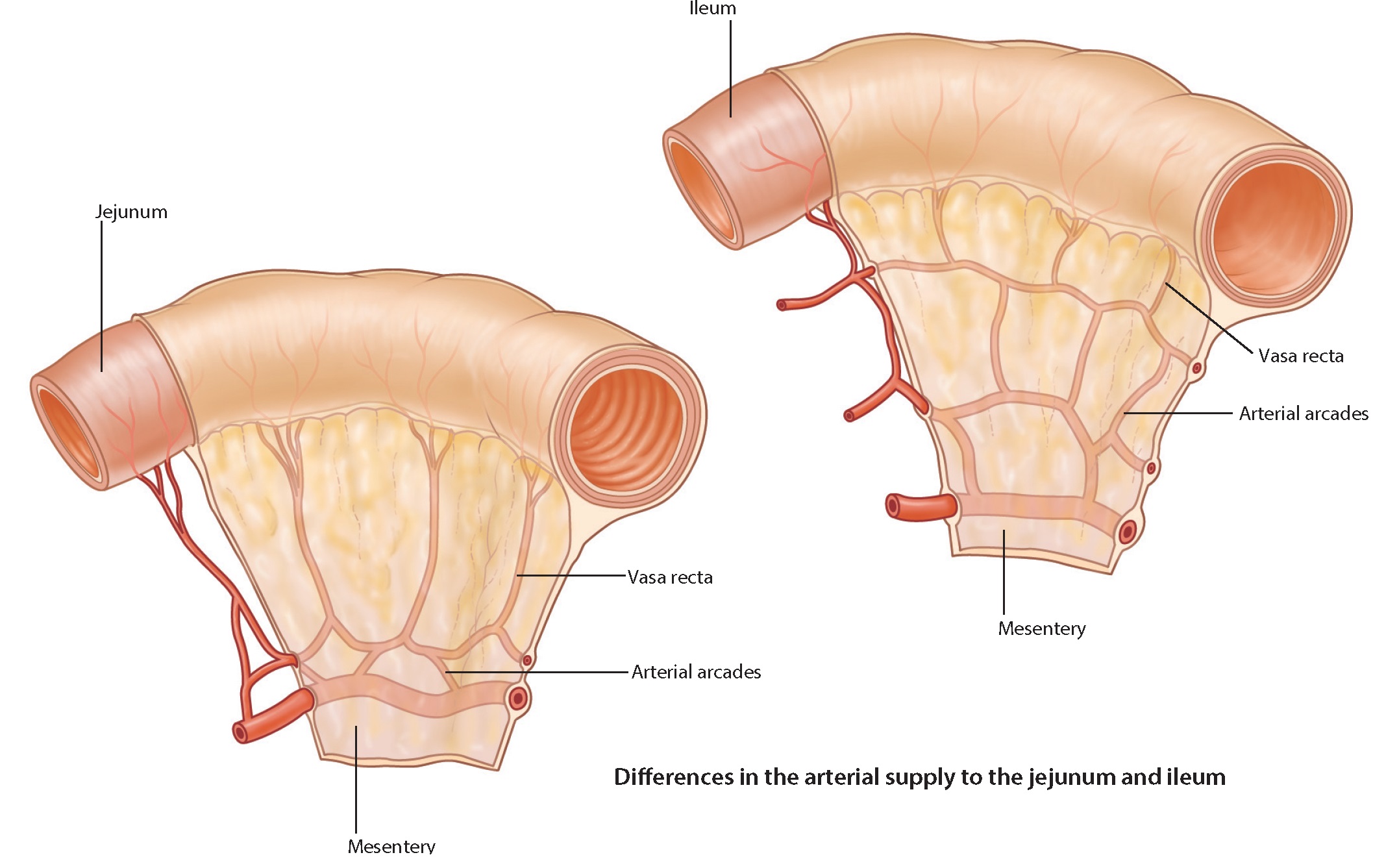
1Identify the parts of the small and large intestines.
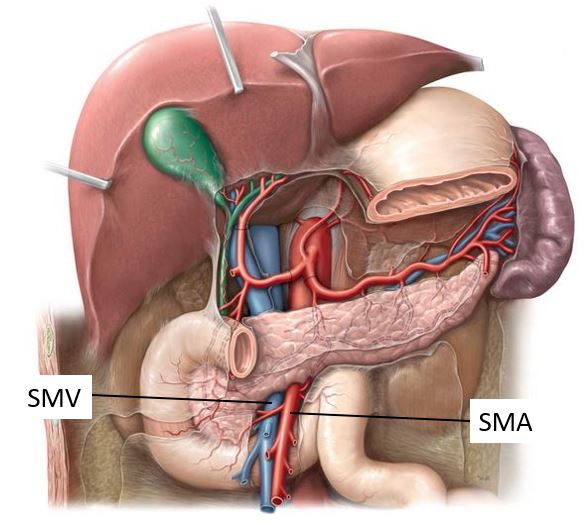
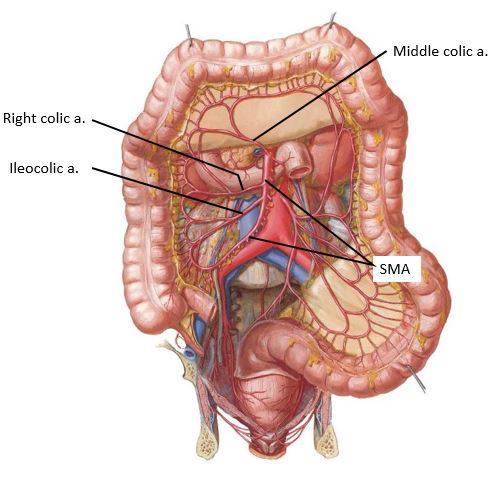
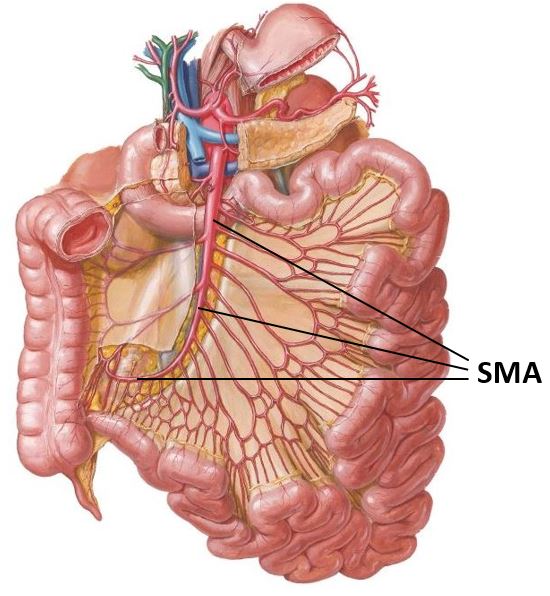
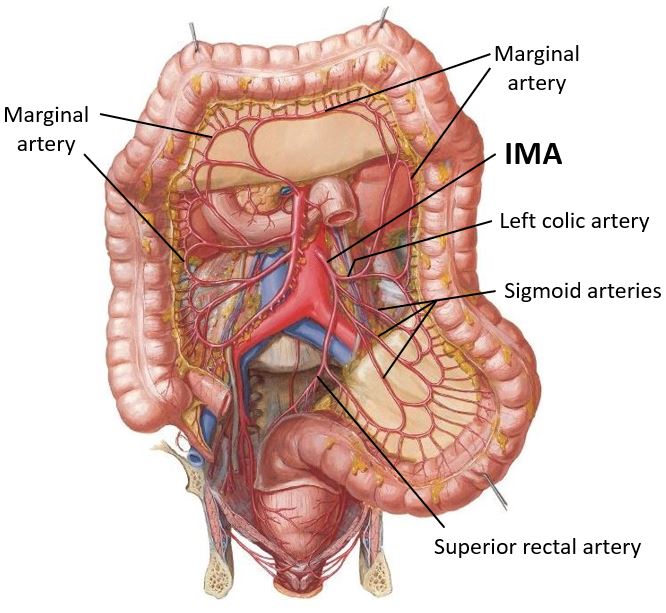
2Dissect the superior and inferior mesenteric arteries and their branches.
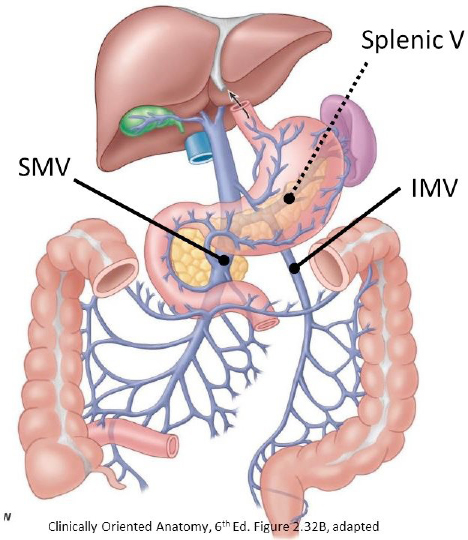
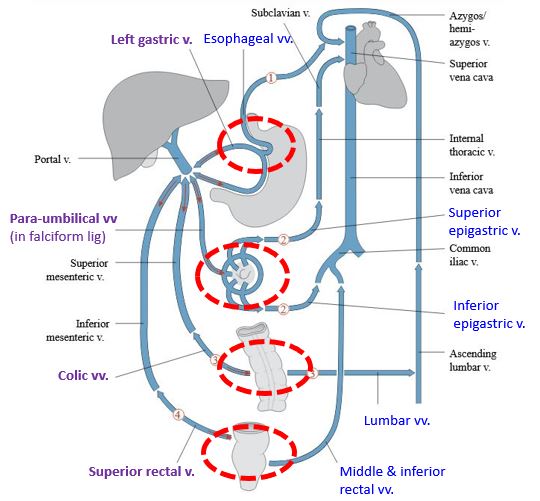
3Identify the hepatic portal vein and its major tributaries.
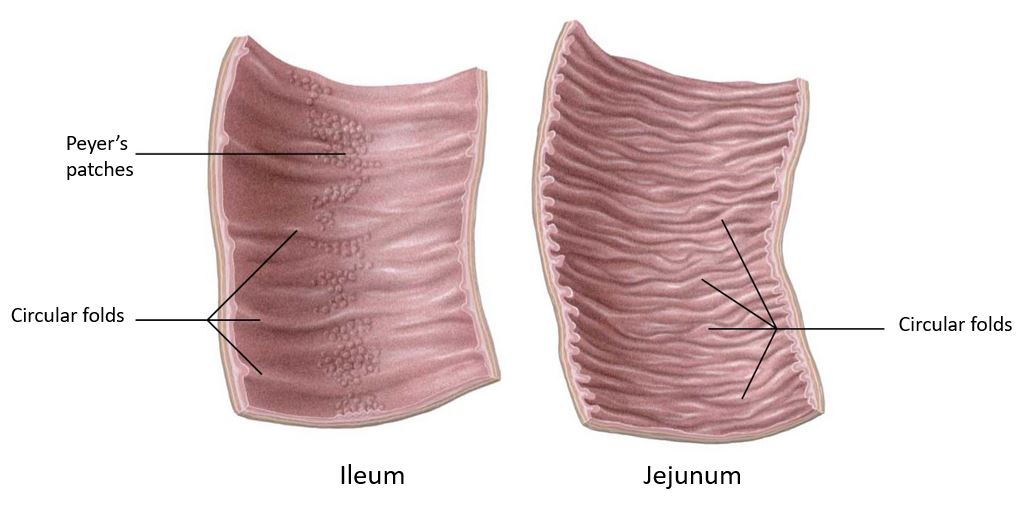
4Open the jejunum, ileum, and cecum to view their internal features.