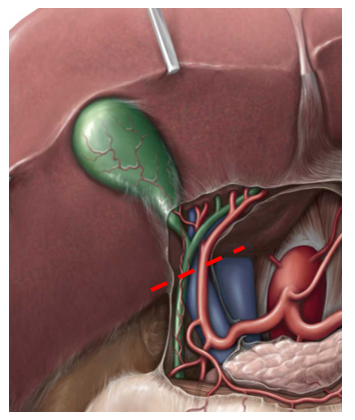
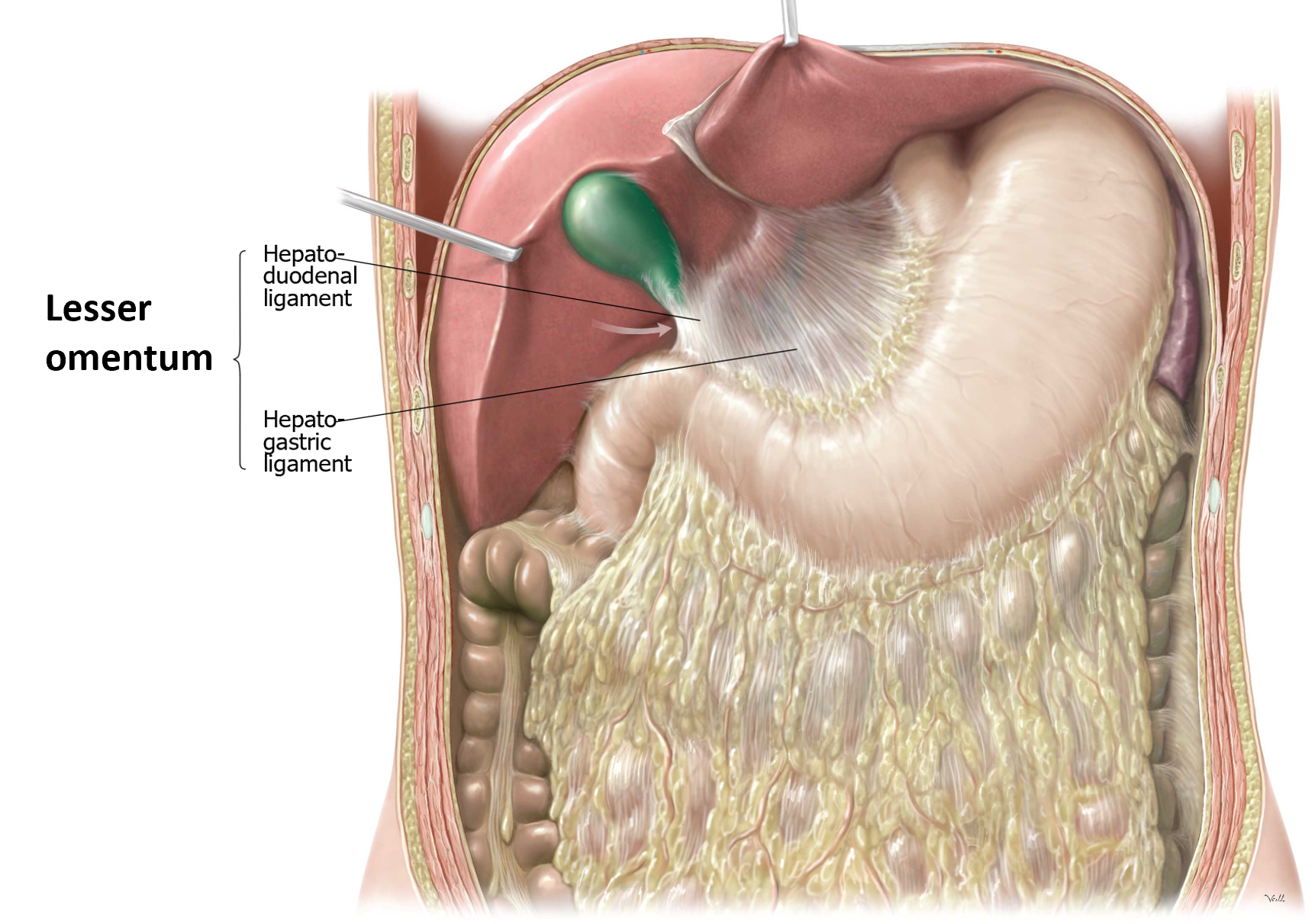
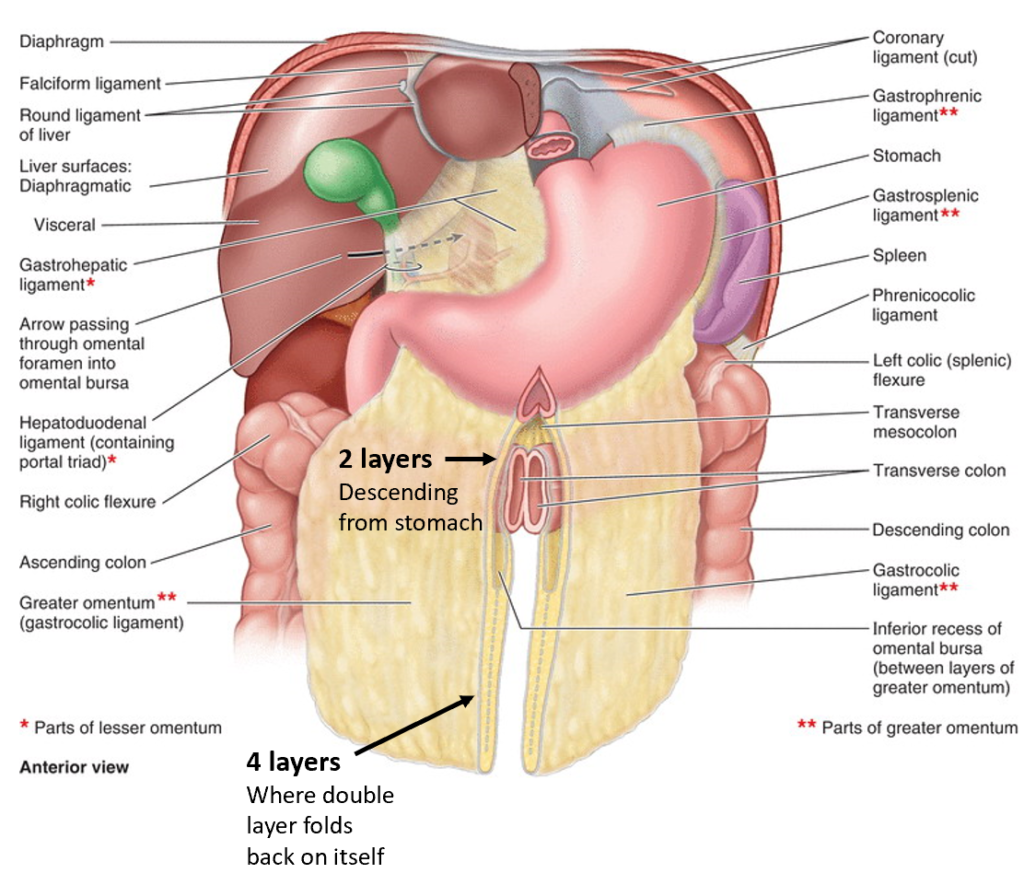
The lesser omentum has two parts:
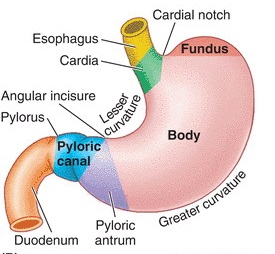
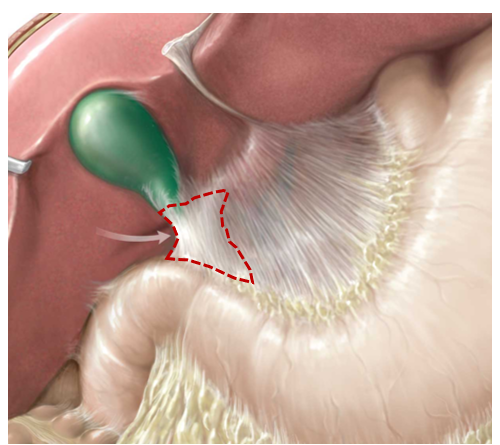
1Hepatogastric ligament = very thin, almost transparent. Connects liver to lesser curvature of stomach.
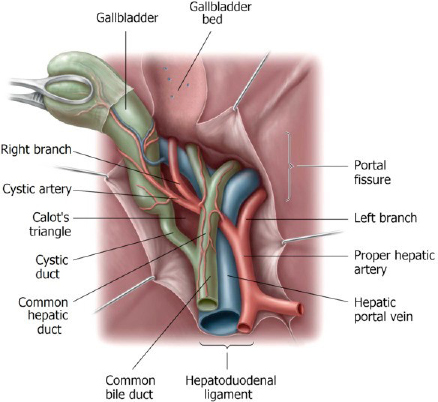
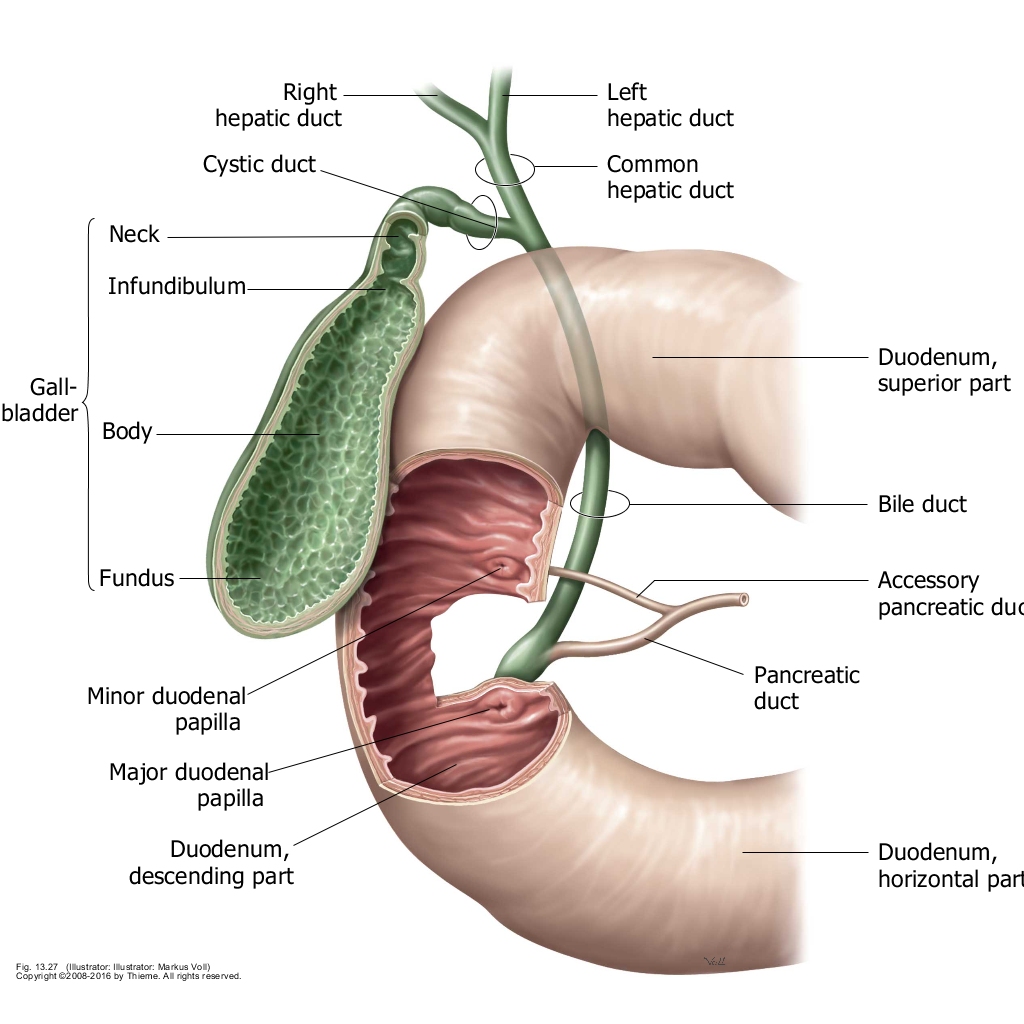
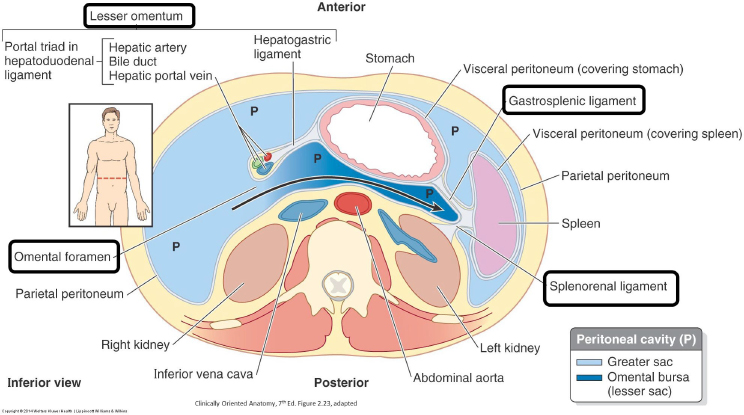
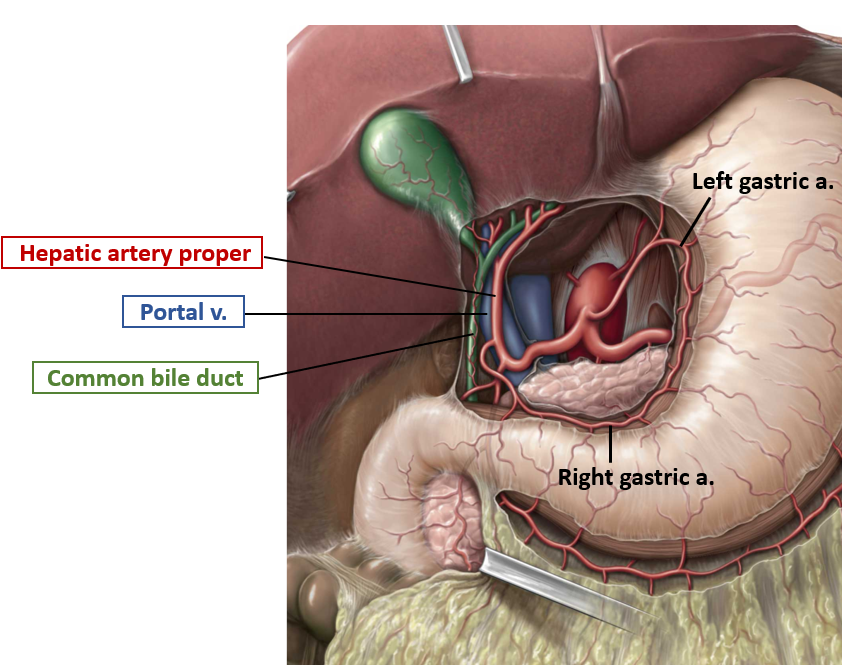
2Hepatoduodenal ligament = connects liver to first part of duodenum (the other parts of the duodenum are retroperitoneal). It is thick, because it contains the portal triad: the hepatic artery proper, the bile duct, and the portal vein. Feel the structures within the hepatoduodenal ligament between your thumb and finger.
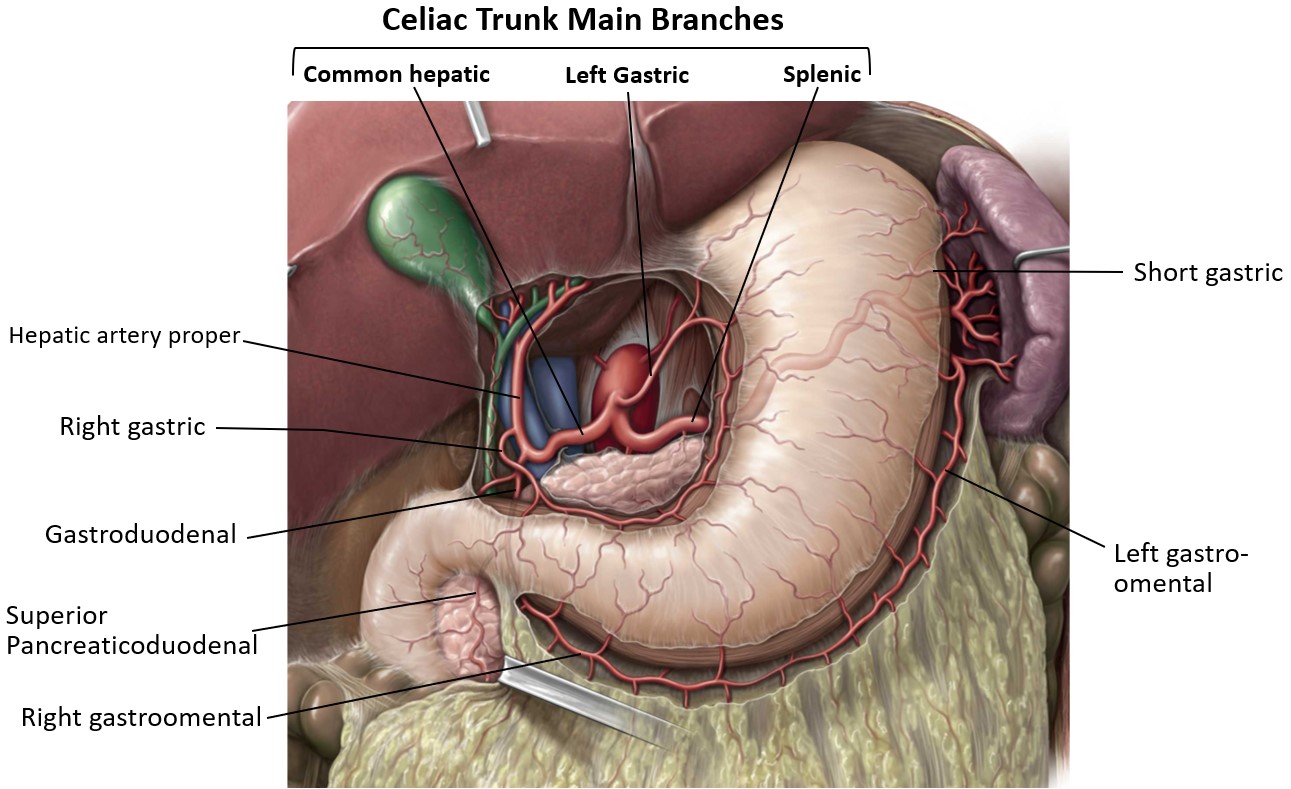
Splenic Artery
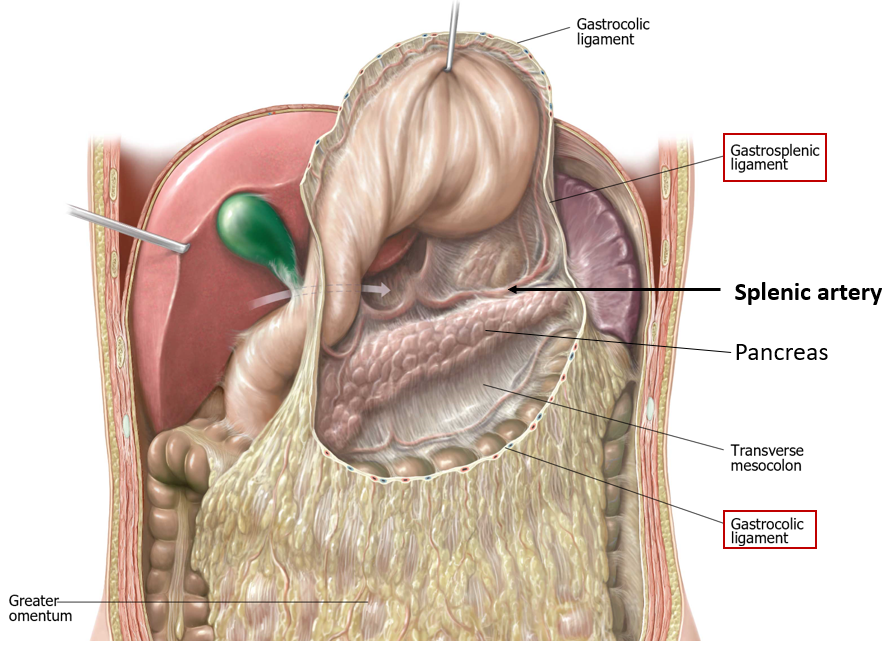
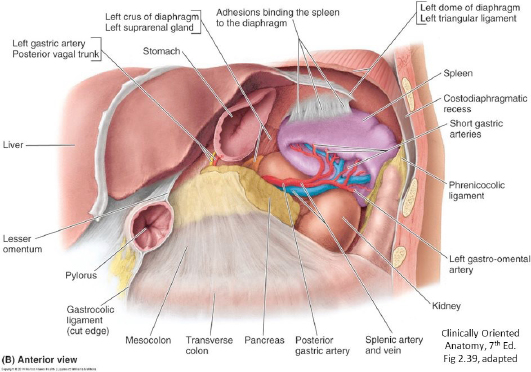
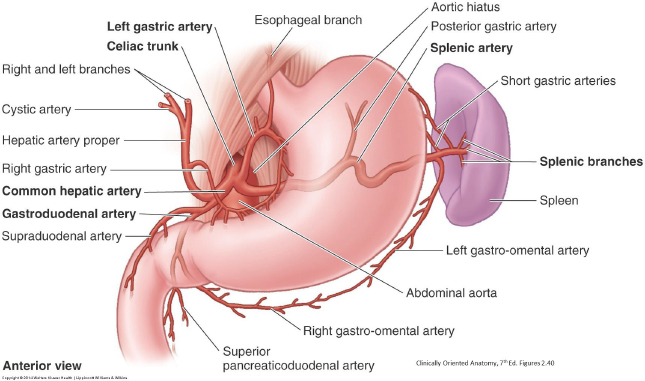
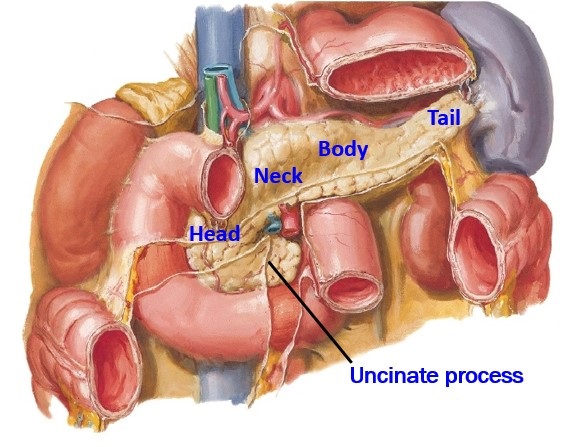
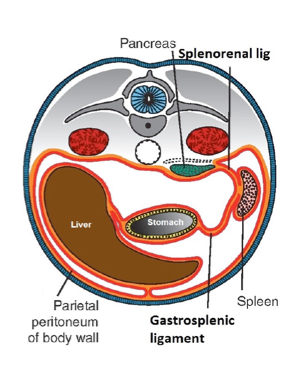
Follow the splenic artery: with scissors, open a hole in the gastrosplenic ligament to the left of the greater curvature of the stomach. Widen the opening with your hands by tearing into the gastrocolic ligament, from left to right, below the greater curvature of the stomach (be careful not to damage the gastro-omental arteries running along the greater curvature!) Elevate the stomach to reach the hilum of the spleen. You should see the pancreas just deep to the peritoneum on the floor of the lesser sac. Clean the hilum of the spleen to find the splenic artery. Trace the tortuous (twisty) splenic artery to the right until you reach the celiac trunk. It runs along the upper border of the pancreas and may be embedded in pancreatic tissue. See Figure 23.17.
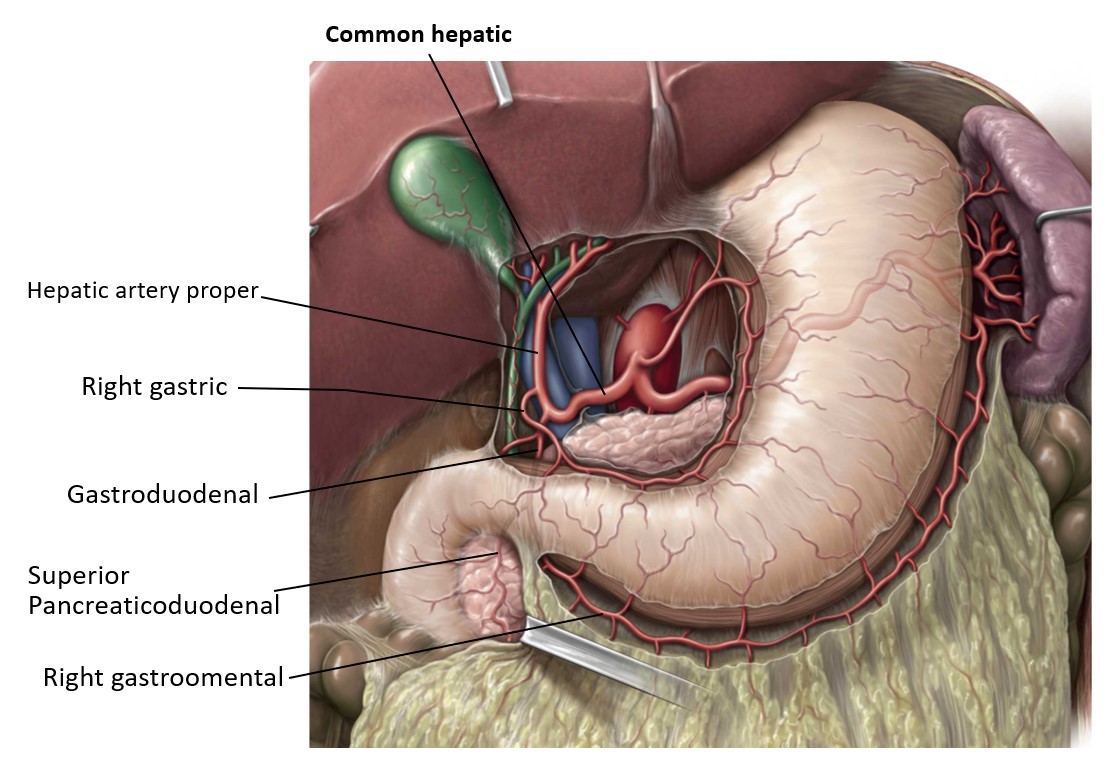
Find the left gastro-omental artery passing from the splenic artery onto the greater curvature of the stomach (within the gastrocolic ligament). Keep following it, and it will merge with the right gastro-omental artery, which comes from the gastroduodenal artery.