 Tap to enlarge.
Tap to enlarge.
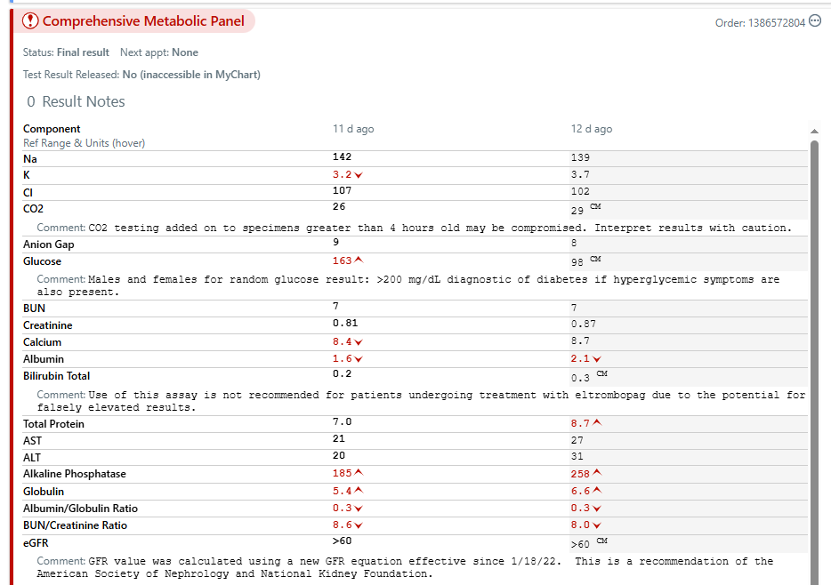
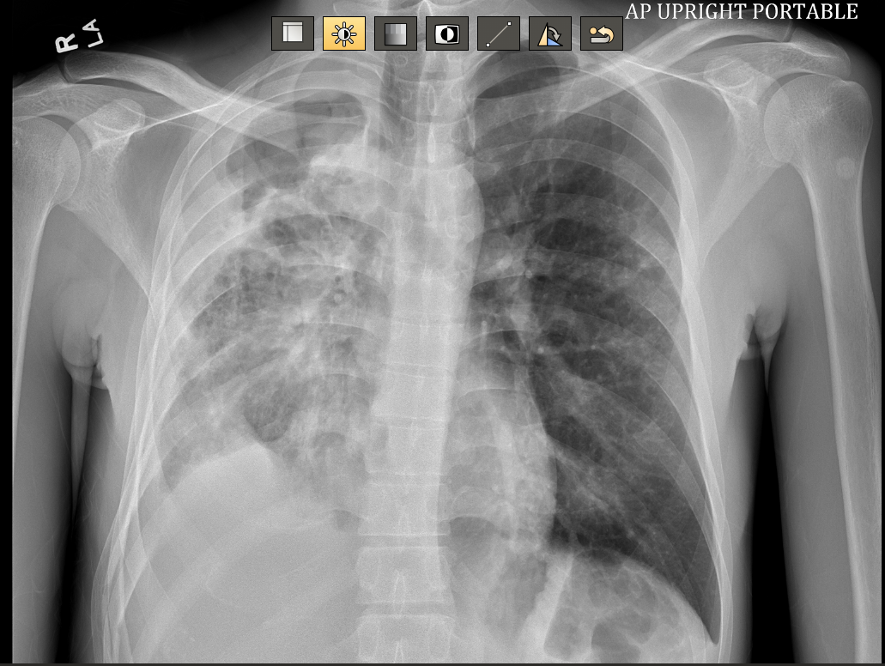
Clinical information
Cough.
Comparison
Previous CXR received from Federally Qualified Health Center (FQHC) urgent care.
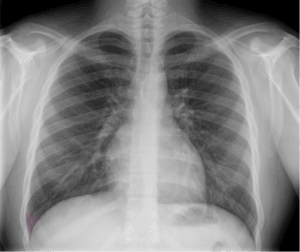
Findings
Right lung consolidation with moderate hydropneumothorax. Normal cardiomediastinal silhouette. No pneumothorax, pleural effusion, or adenopathy. No significant bone abnormality.
Impression
Right lung consolidation with moderate hydropneumothorax could represent pneumonia with parapneumonic effusion versus cavitary pneumonia. Further evaluation with CT is recommended.
Clinical information
Cough and fever for six months. Abnormal chest radiograph.
Comparison
XR chest AP portable (5/23/2025) We try not to have dates. Is this necessary?
Procedure
Axial images through the chest after the administration of 75ml Omnipaque 350 intravenous contrast. Multiplanar reconstructions.
At least one of the following CT dose optimization techniques were used: Automated exposure control; adjustment of mA and/or kV according to patient size; use of iterative reconstruction technique.
Findings
Lungs: Cavitary consolidation of the right-upper lobe as well as of the regions of cavitation within the right-middle and lower lobes. The greatest degree of cavitation is present within the right-upper lobe measuring at least 5.4 × 5.3 × 4.8 cm. Scattered centrilobular airspace opacities involving the right greater than left lung. No cavitation within the left lung.
Multilocular right-sided pleural effusion with complex thin septations. Pleural collection along the anterior inferior right hemithorax measures at least 4.7 × 7.5 cm. Additional loculated posterior pleural component is mild to moderate in severity.
Mediastinum: Normal heart size without pericardial effusion. No pathologically enlarged lymph nodes.
Coronary artery calcification: Minimal or no coronary calcification.
Partial visualization upper abdomen: Negative.
Musculoskeletal: Negative.
Impression
- Multifocal cavitary pneumonia involving the right lung with multilocular right-sided parapneumonic effusion. Findings compatible with necrotizing pneumonia and associated empyema. Significant cavitation involving the right-upper lobe, detailed above. Recommend cardiovascular surgical consult.
- Scattered centrilobular airspace opacities involving the right greater than left lung, likely infectious or inflammatory.