Workup depends on whether the presentation is typical or if there are atypical features such as young age, rapid onset, other neurologic signs (like Parkinsonism).
- If the presentation is relatively typical (older adult [>65 years old], gradual short-term memory loss as the initial symptomatology, then the basic workup is usually:
- Screening neurologic exam and MoCA.
- Basic metabolic, B12, TSH, vit D.
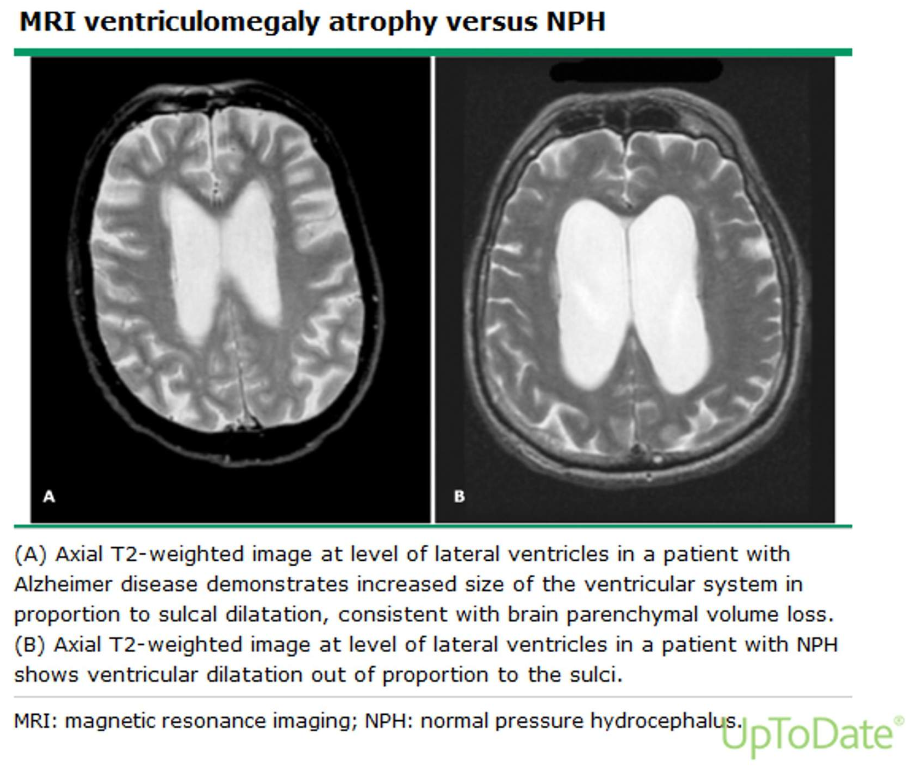
- MRI (with contrast if early/rapid onset), CT first test acceptable.
- RPR, Viral PCR.
- Consider sleep studies.
- If younger, atypical or rapid onset, consider other diagnoses:
- Toxin exposure (ETOH, other), Infectious dz w/u (HIV, RPR, Lyme).
- Rheumatology eval.
- Paraneoplastic?
- For early onset or unusual presentations, consider the following with neurologic consultation:
- CSF amyloid β42; Tau/P-tau levels.
- Consider PET if CSF not available.
- Dementia vs. delirium: They can co-occur!
- Dementia = progressive cognitive decline.
- Mainly affects memory.
- Typically caused by changes in neuroanatomy.
- Delirium = reversible decline in cognition.
- Mainly affects attention.
- Typically caused by acute illness, drug adverse effect, or substance use (including ETOH).
- Dementia = progressive cognitive decline.
- Mild cognitive impairment (MCI): relatively mild, objective cognitive deficits that do not meet the criteria for dementia, but are more than those expected with normal aging.
- Patients are still typically able to function independently.
- Stroke.
- Mass.
- Tumor.
- Abscess.
- Co-existing mood disorders (e.g., depression).
- Conditions that can be chronic: E.g., undiagnosed hypothyroidism, vitamin deficiencies, neurosarcoidosis, etc.