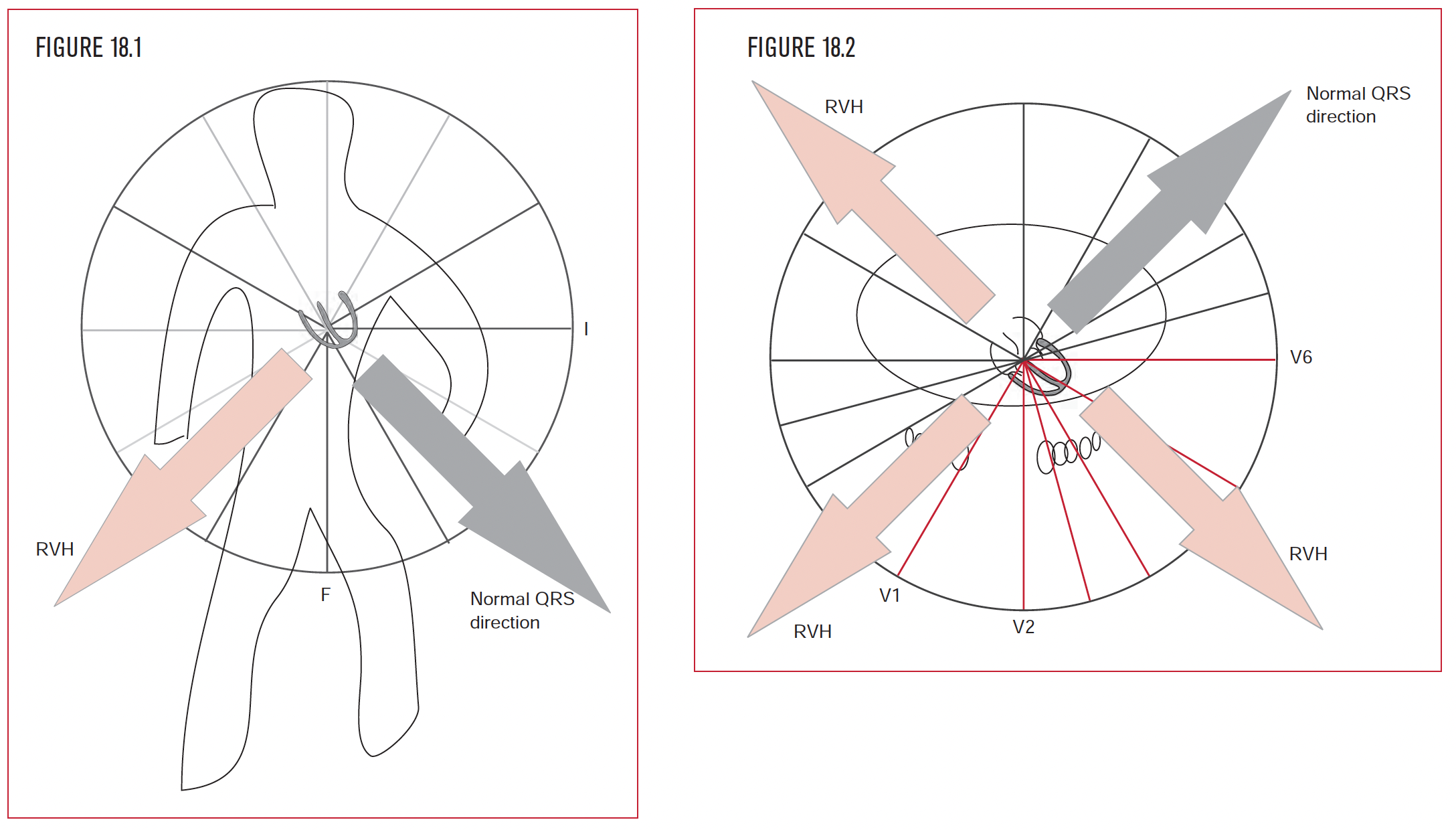
In the frontal plane, the normal QRS direction is to the patient’s left (Figure 18.1). In the horizontal plane, the normal overall QRS direction also points to the left ventricle, which is to the patient’s left and posterior (Figure 18.2).
The diagnostic hallmark of right ventricular hypertrophy is an overall QRS direction that points either to the patient’s right, anterior, or both (Figures 18.1 and 18.2).
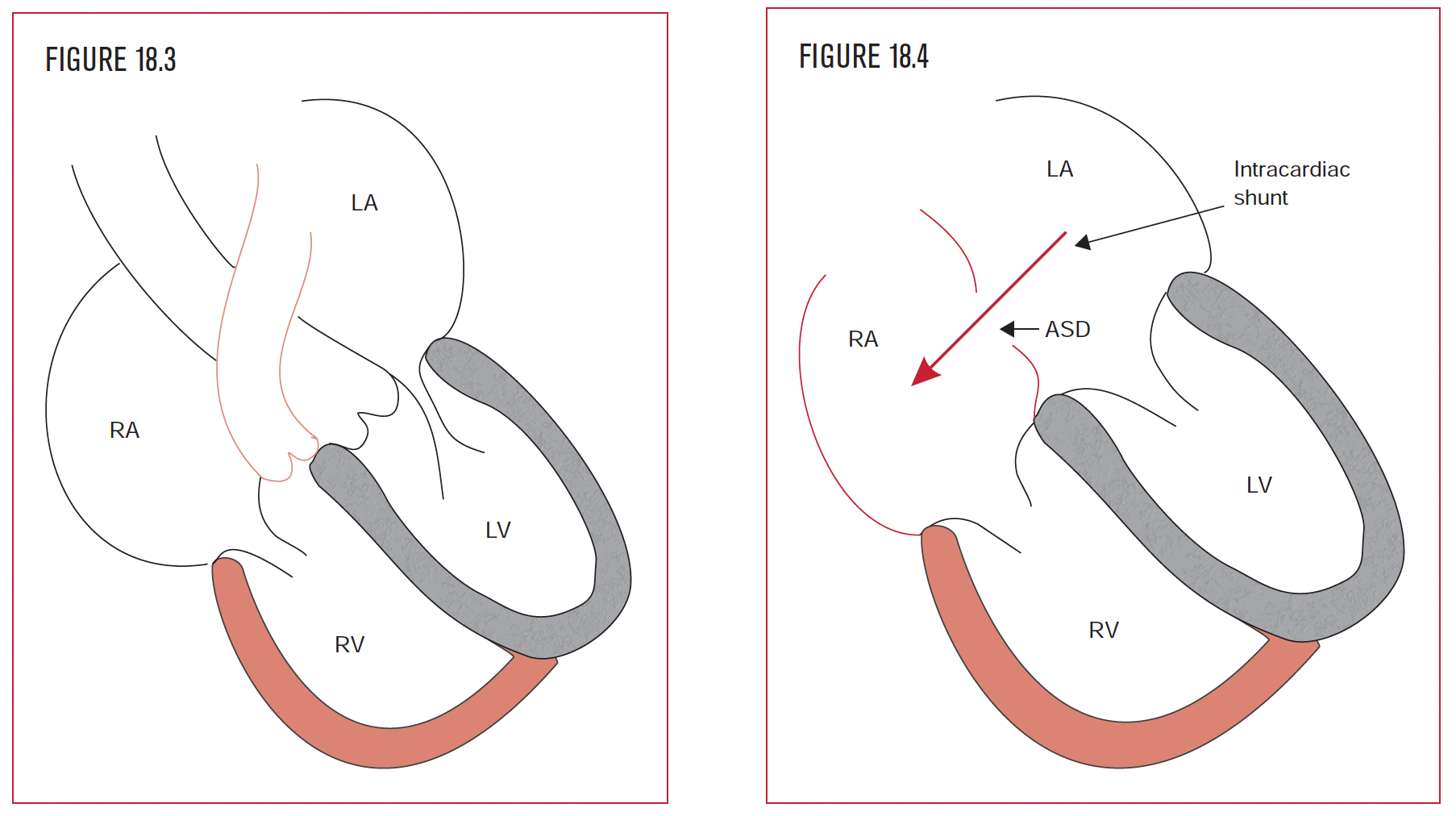
As the right ventricle is subjected to the stress of pressure or volume, its mass increases as a compensatory mechanism to handle the increased work. Increased pressure (Figure 18.3) in the right ventricle can be present from pulmonary hypertension. In adults, this is commonly due to obstructive lung disease or pulmonary emboli. The right ventricular adaptation is to increase its mass.
Increased volume in the right ventricle (Figure 18.4) can result from tricuspid regurgitation or an intracardiac shunt, such as an atrial septal defect (ASD). To handle the volume overload, the right ventricle has to “make space,” and so it dilates.
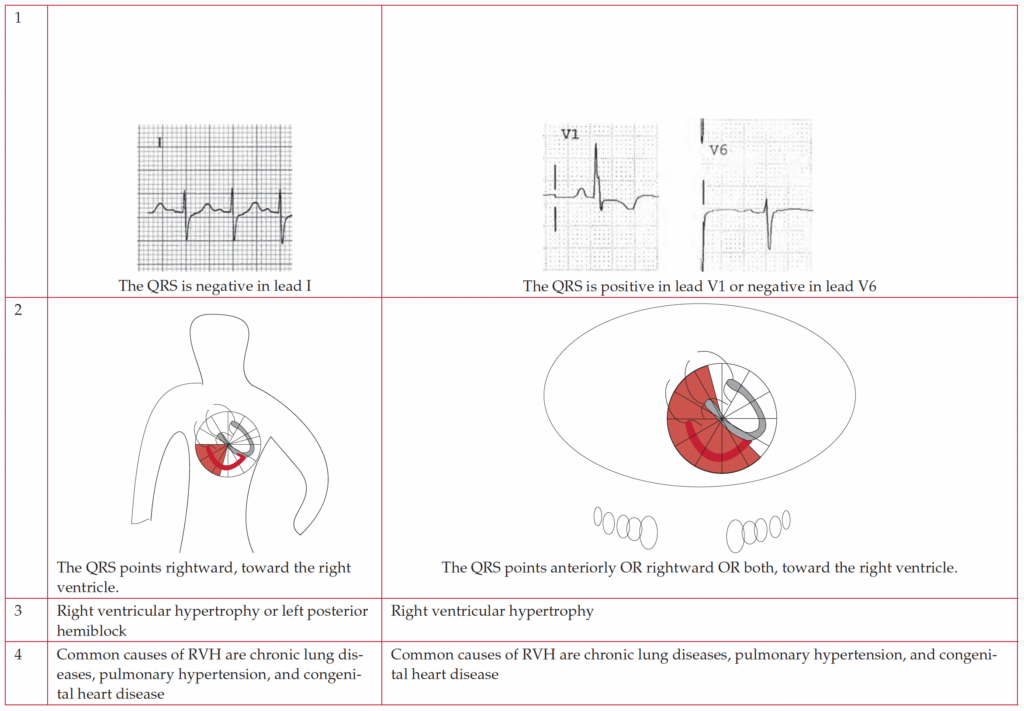
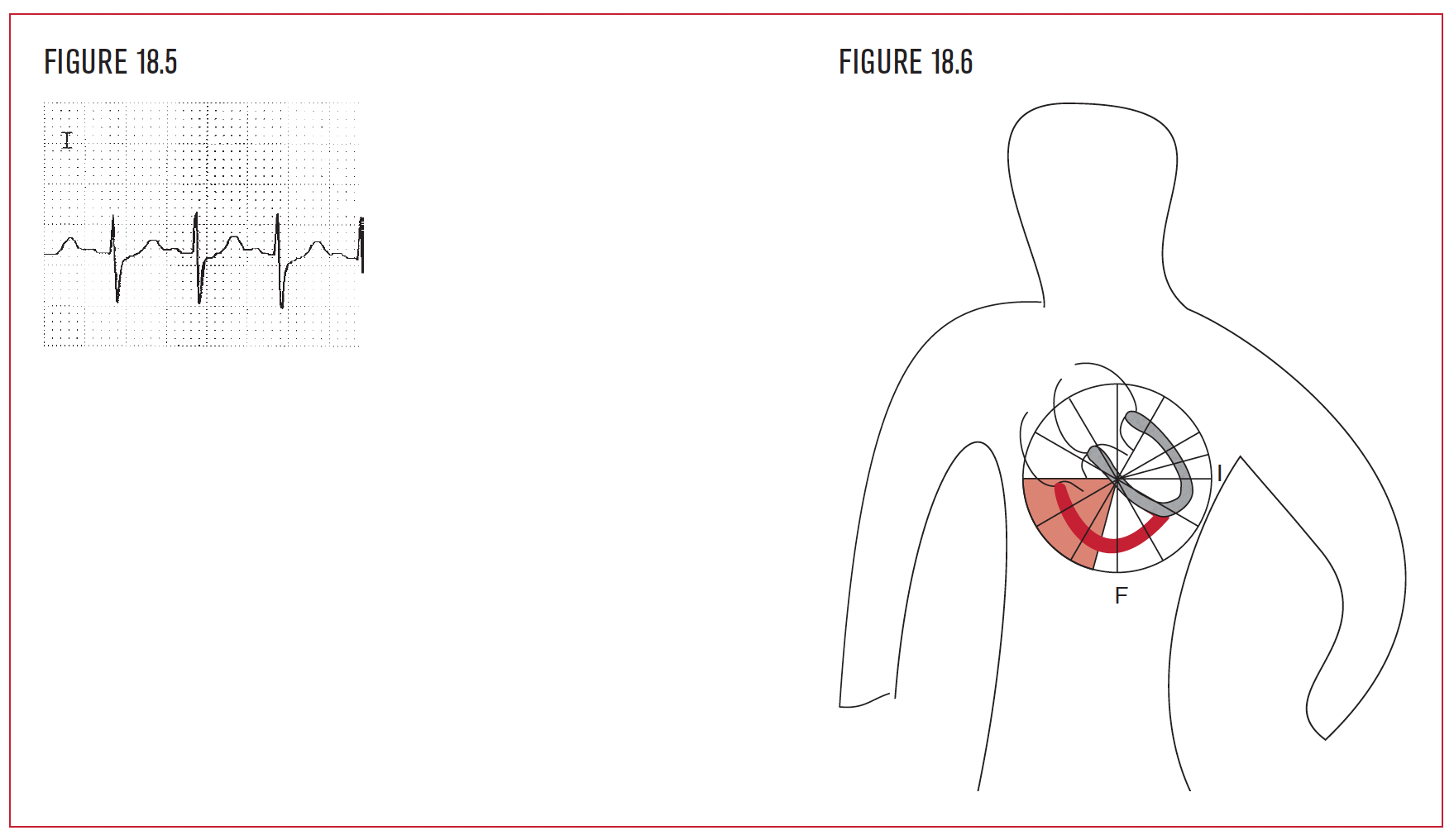
The left ventricle is leftward and posterior. As it depolarizes simultaneously with the right ventricle, its more massive forces predominate. As a result, the mean QRS axis normally points toward the left ventricle. If the right ventricle can achieve enough mass to pull the mean QRS rightward in the frontal plane, then this indicates right ventricular hypertrophy. If the QRS in lead I is negative (Figure 18.5), it indicates that the mean QRS axis in the frontal plane is rightward this by itself indicates RVH (Figure 18.6). Chapter 8 demonstrated LPHB as an otherwise unexplained right axis. Now there is a differential diagnosis when an EKG has a mean QRS that points rightward: LPHB, RVH, or a large lateral wall infarction. Other clues must be examined to help narrow down the diagnosis.
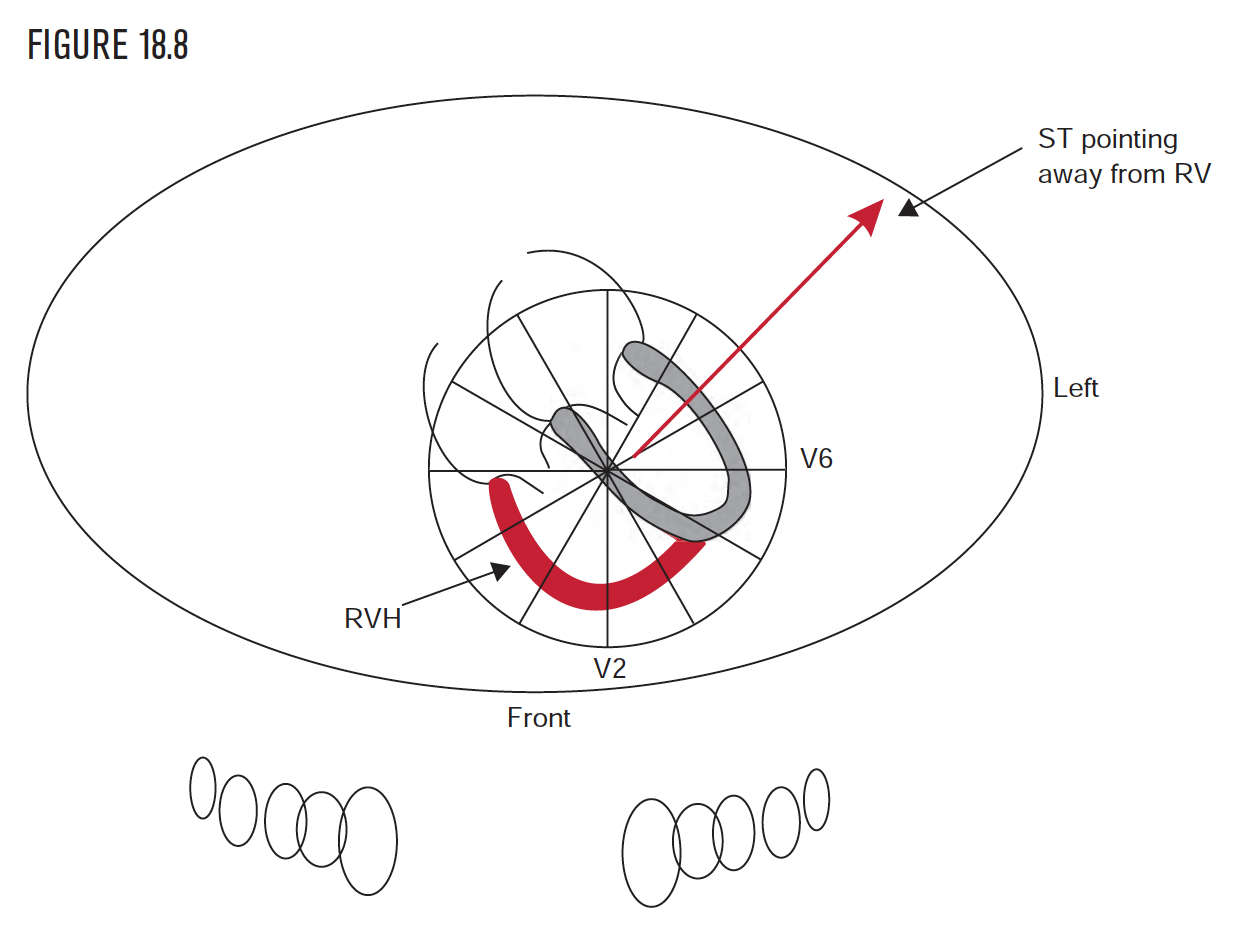
The left ventricle is leftward and posterior. As it depolarizes simultaneously with the right ventricle, its more massive forces predominate. As a result, the mean QRS axis normally points toward the left ventricle. If the right ventricle can achieve enough mass to pull the mean QRS either rightward or anterior, in either the frontal plane or the horizontal plane, then this indicates right ventricular hypertrophy.
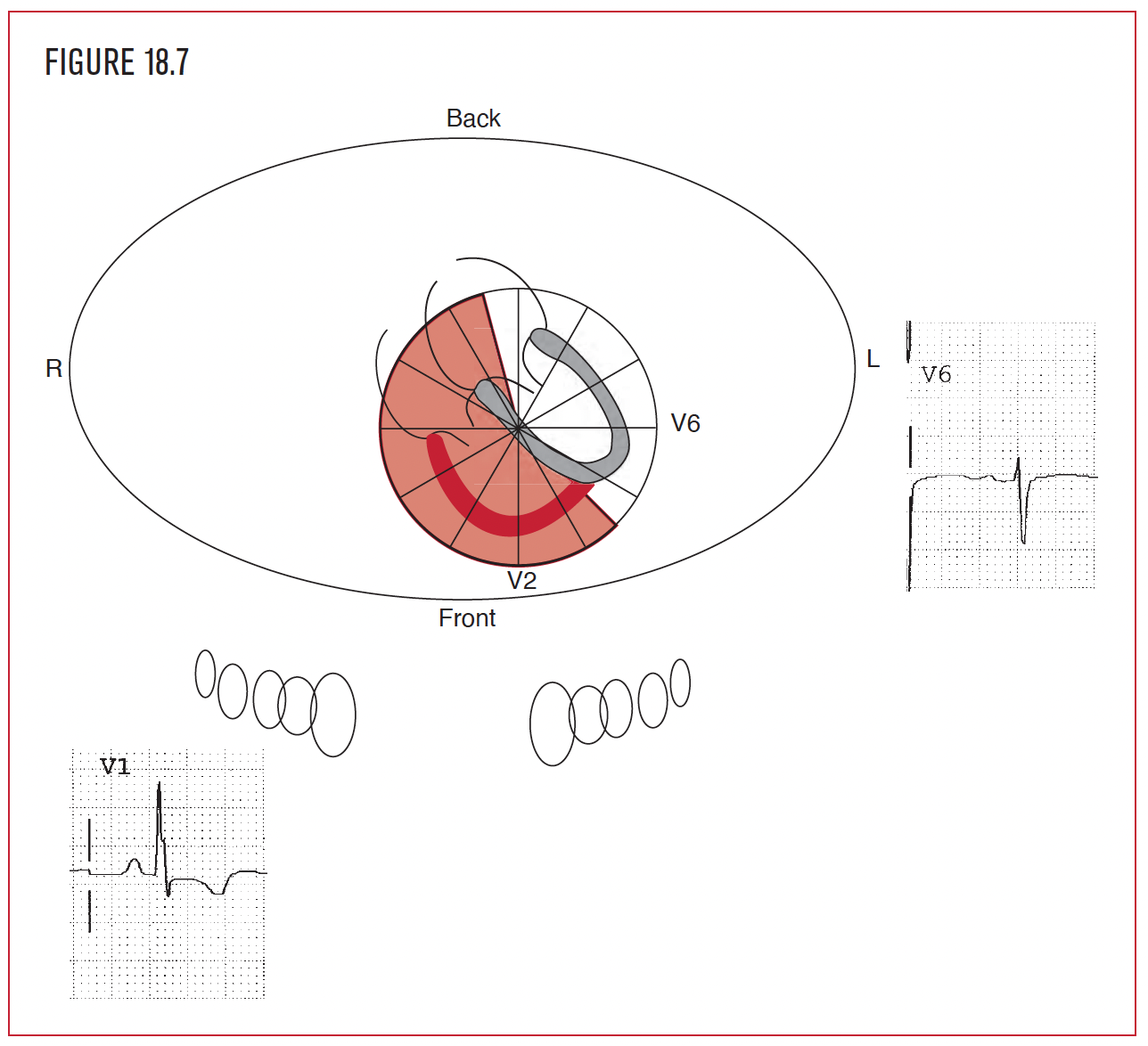
If lead I is negative, it indicates that the mean QRS axis in the frontal plane is rightward, which by itself indicates RVH. Notice that the mean QRS (in this example Figure 18.7) in the horizontal plane is rightward (V6 is negative) and also anterior (V1 is positive). Cut the right ventricle some slack. It is up against the left ventricle. If the right ventricle can pull the QRS either anterior or rightward, then this indicates RVH. (See Figure 6.63 for review.)