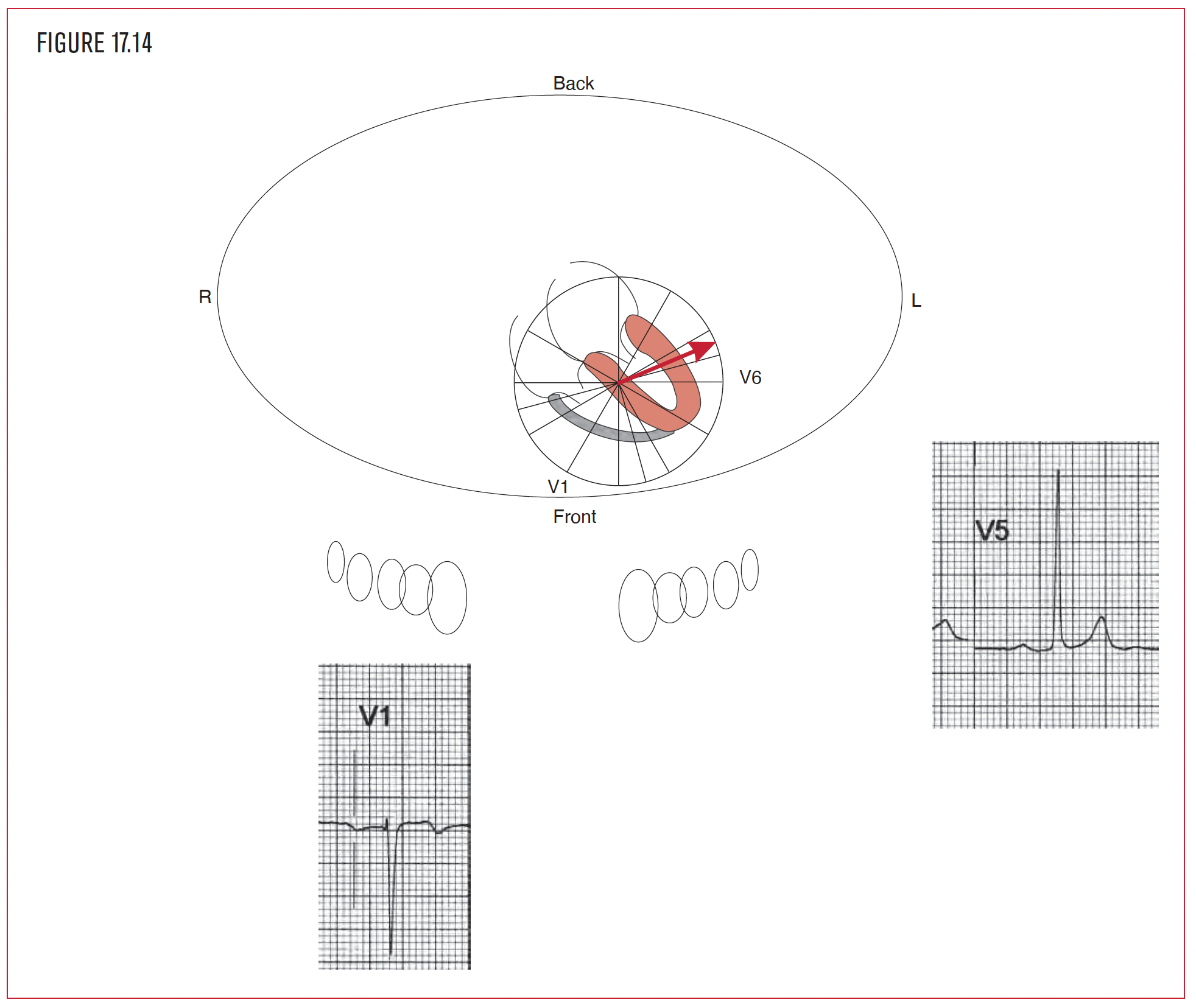
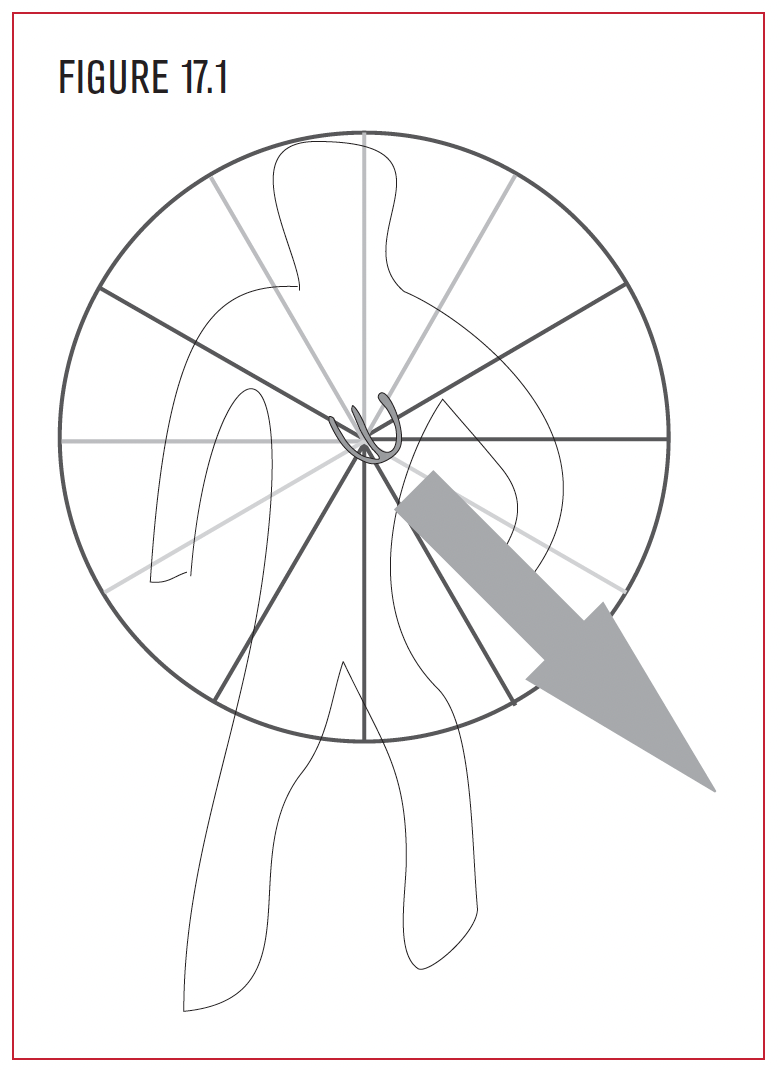
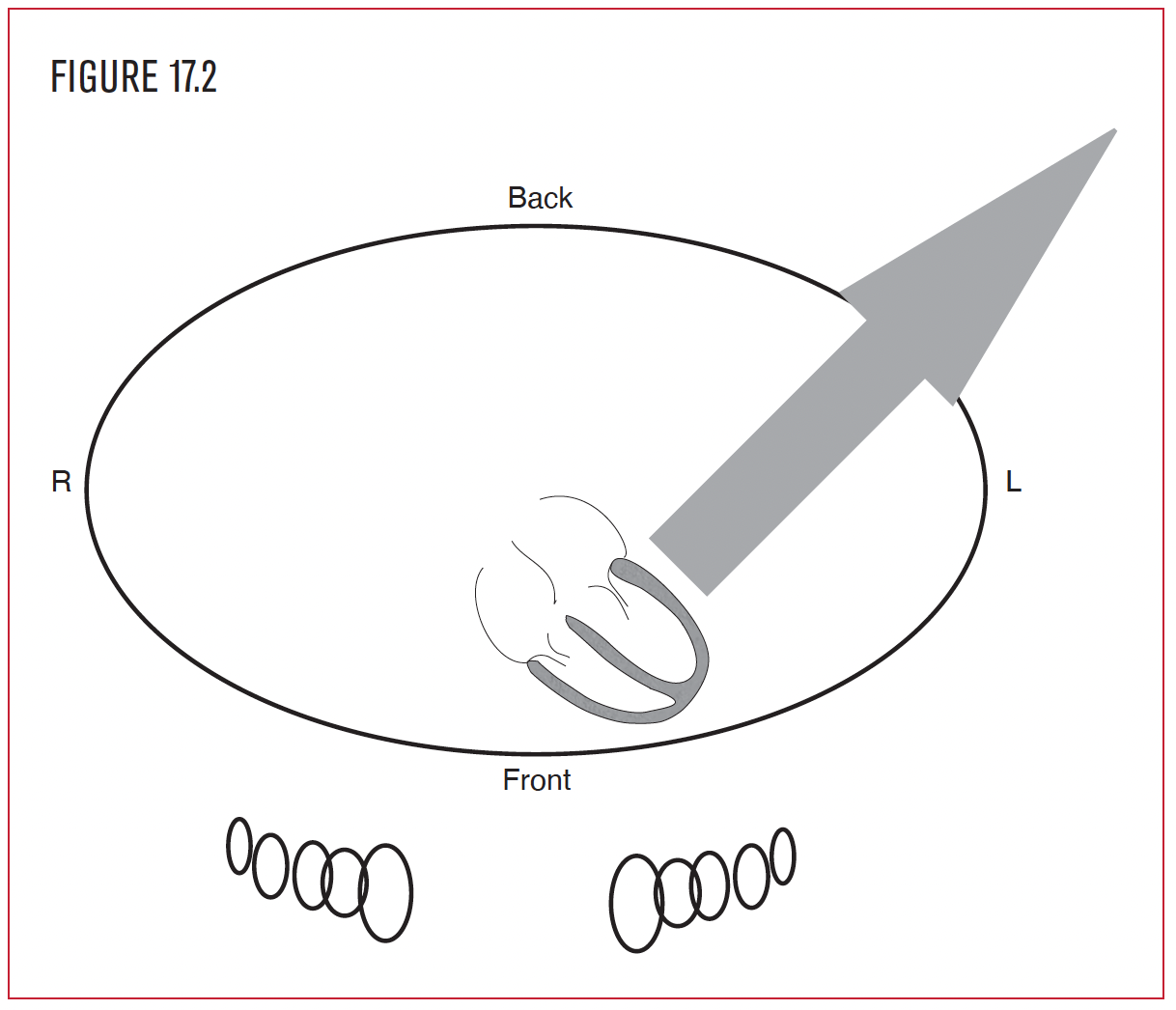
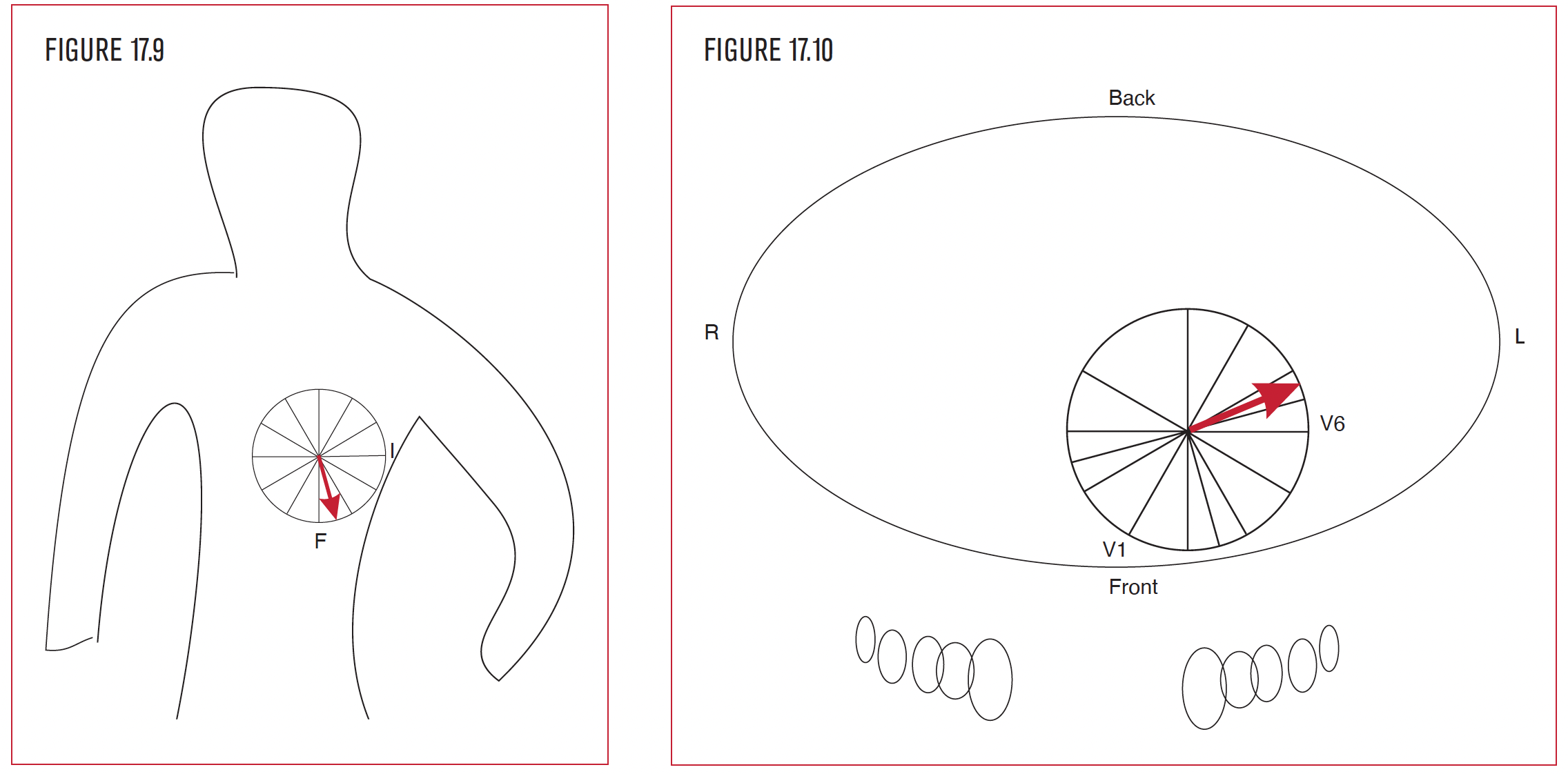
The left ventricle is located to the left and in back of the right ventricle. It is the systemic chamber of the heart and therefore is much larger in size than the right ventricle. Because the left ventricle is larger than the right ventricle, the overall QRS direction normally points posterior and leftward toward the left ventricle (Figure 17.2).
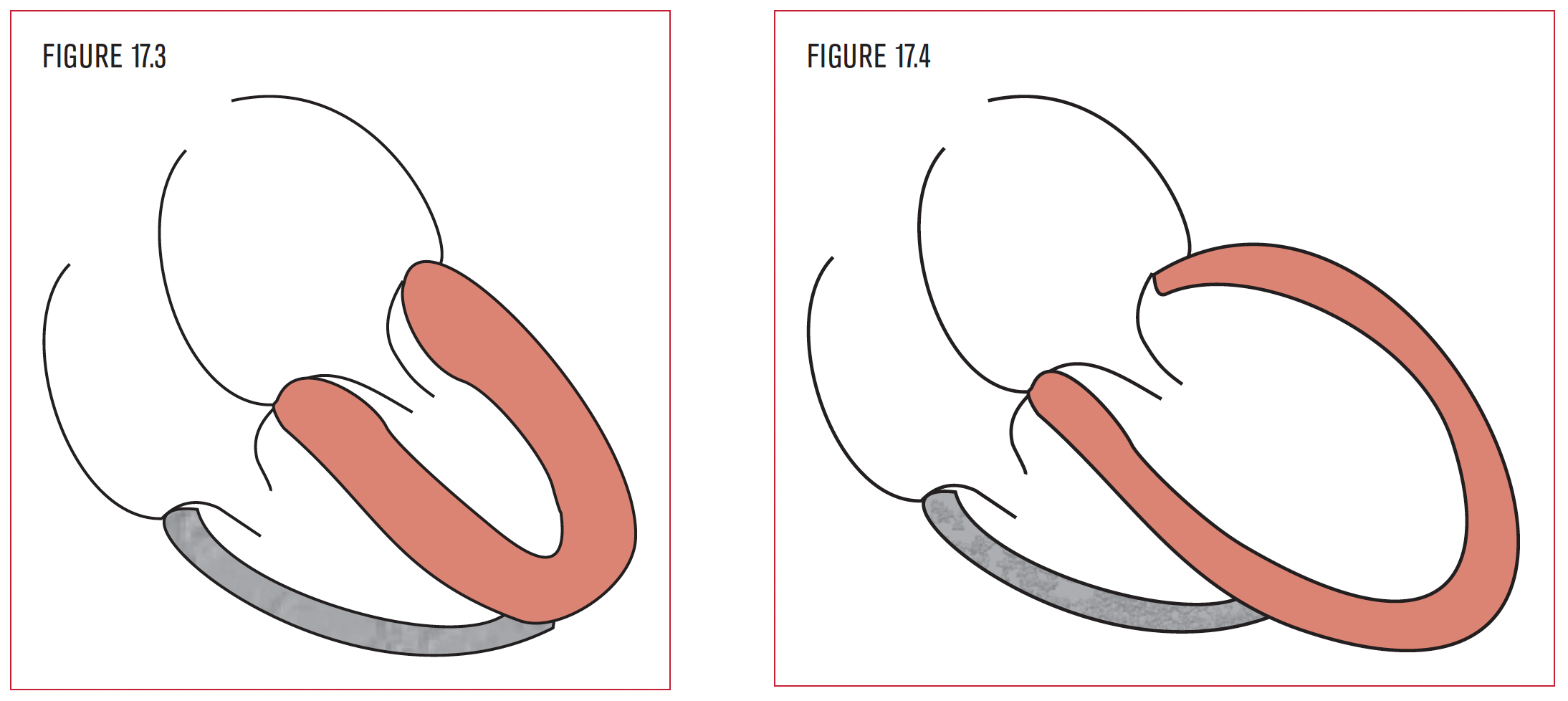
LVH is often the result of an increase in pressure or volume within the left ventricle. When the pressure in the left ventricle increases, it adapts by developing a concentrically thicker wall (Figure 17.3). However, as the ventricular wall thickness increases, the actual cavity size becomes smaller. Increased pressure in the left ventricle is seen in systemic hypertension (HTN), aortic stenosis (AS), and hypertrophic obstructive cardiomyopathy (HOCM or IHSS).
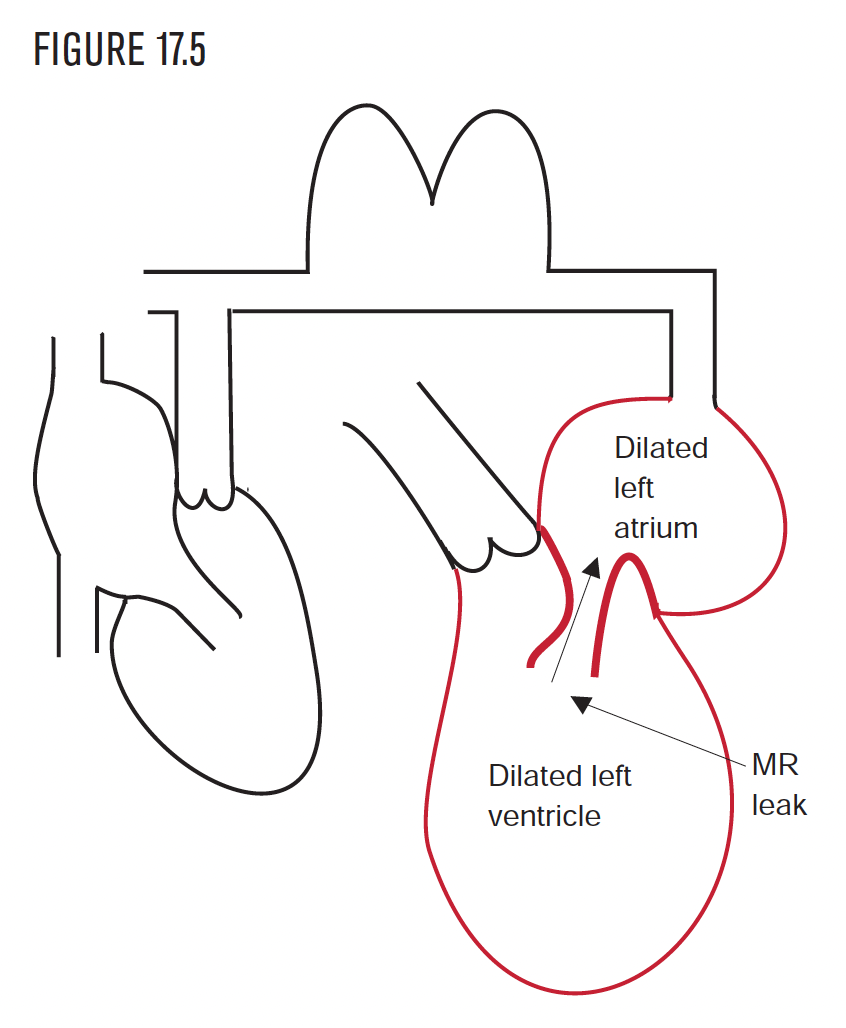
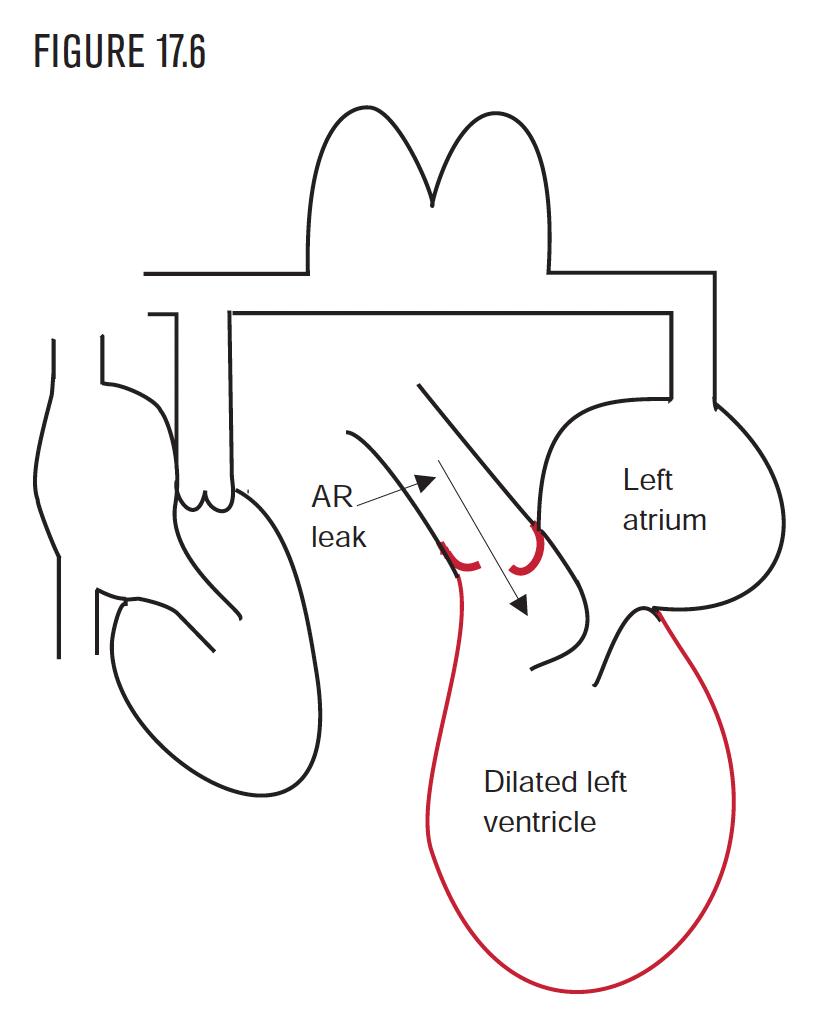
When the left ventricle is strained from volume overload, it compensates by making extra space or dilating (Figure 17.4). Volume overload is often seen in mitral or aortic regurgitation. LVH on the EKG indicates increased LV mass only. It does not distinguish between pressure overload and volume overload.
The most common cause of pressure overload is hypertension (HTN). The presence of LVH on the EKG in the setting of HTN establishes the presence of hypertensive heart disease and should prompt an investigation for other manifestations of end organ damage because of HTN.
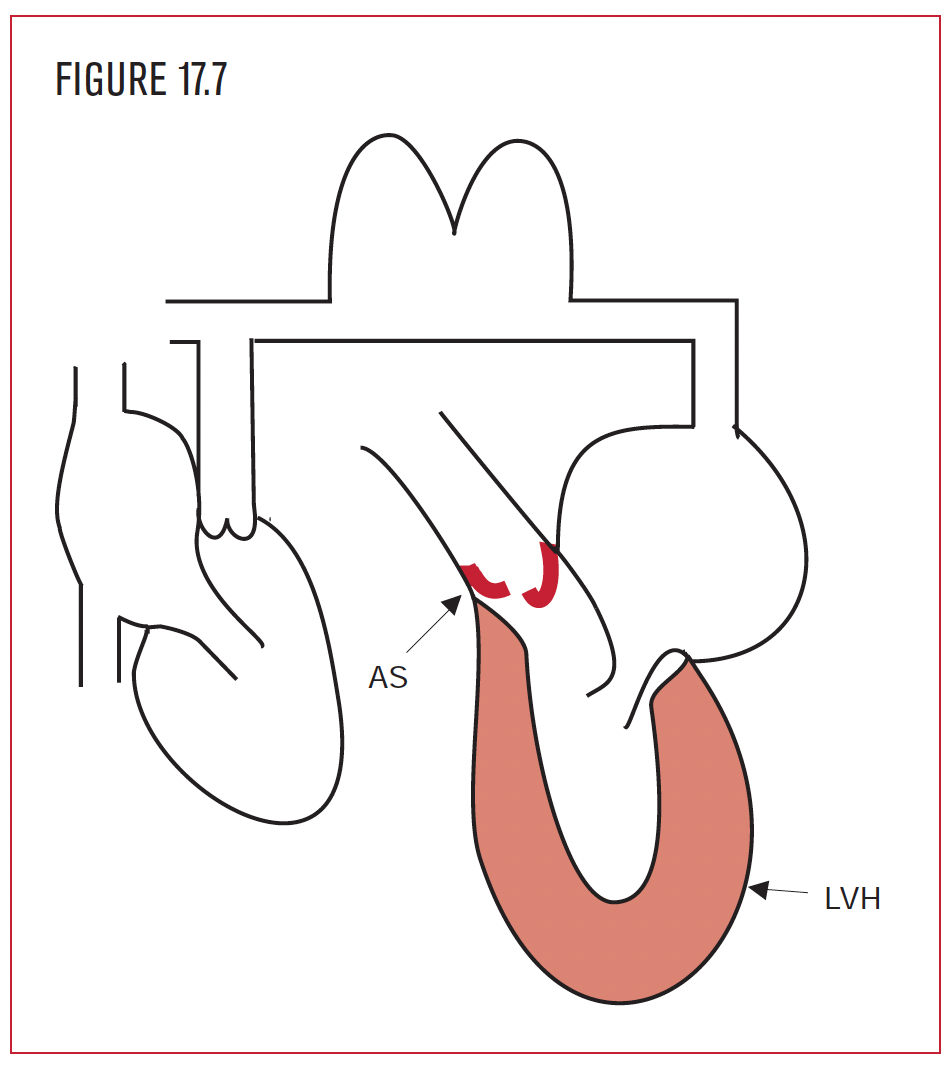 Aortic stenosis (AS) (Figure 17.7) is a less common cause of pressure overload, but should be suspected with LVH on the EKG in the absence of HTN. It develops when the opening of the aortic valve becomes narrowed, restricting the flow of blood out of the left ventricle. The left ventricle hypertrophies to provide the extra force to push the blood through the aortic valve. The most common causes of AS are rheumatic heart disease, congenital malformation, or calcification of the bicuspid or tricuspid valve.
Aortic stenosis (AS) (Figure 17.7) is a less common cause of pressure overload, but should be suspected with LVH on the EKG in the absence of HTN. It develops when the opening of the aortic valve becomes narrowed, restricting the flow of blood out of the left ventricle. The left ventricle hypertrophies to provide the extra force to push the blood through the aortic valve. The most common causes of AS are rheumatic heart disease, congenital malformation, or calcification of the bicuspid or tricuspid valve.
In pressure overload of the left ventricle from any cause, the left atrium hypertrophies as well. The left atrium “bulks up” to develop enough force to push blood into a thick, muscular, unrelaxed ventricle. HOCM or IHSS is a less common cause of LVH.
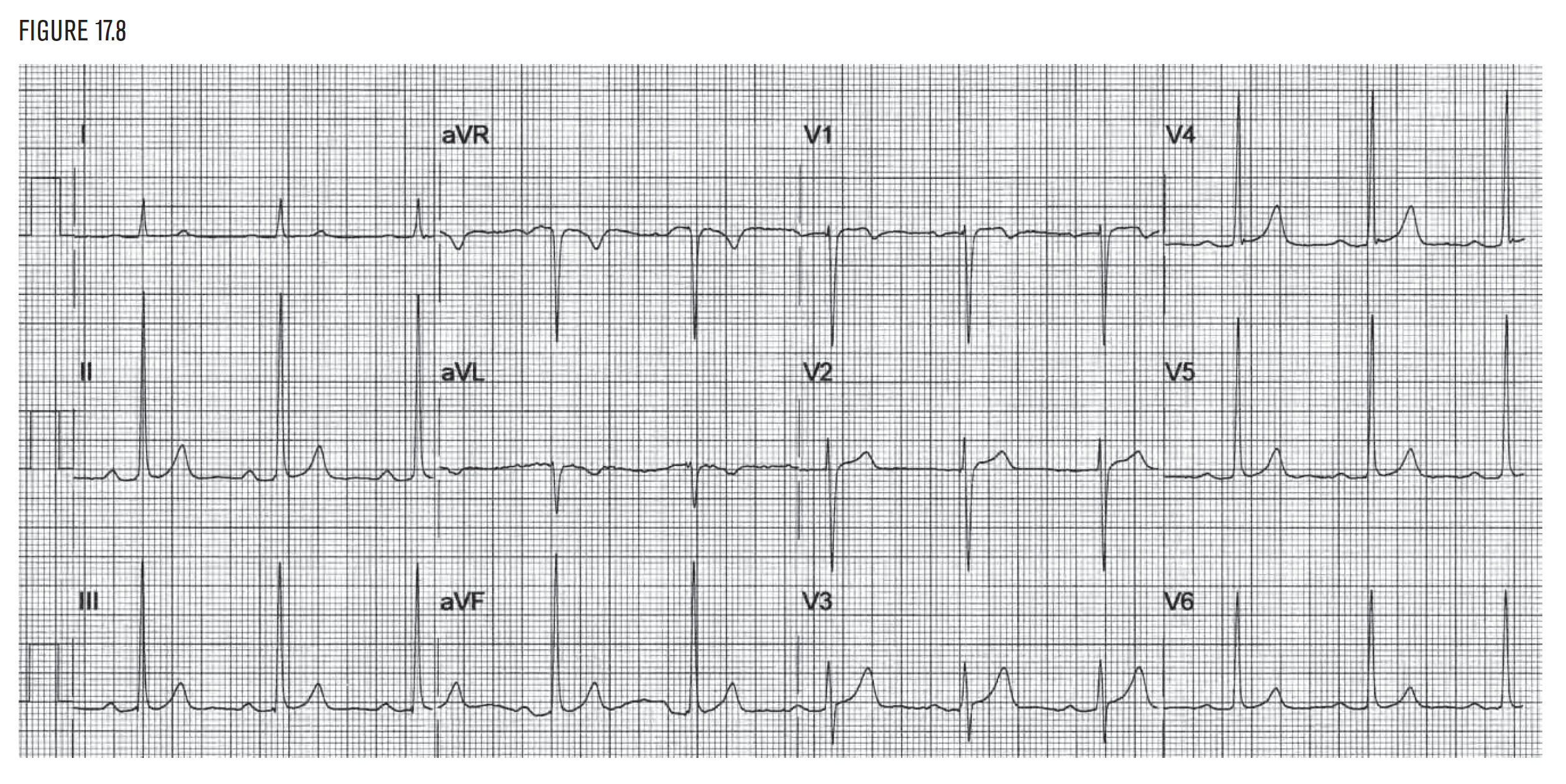
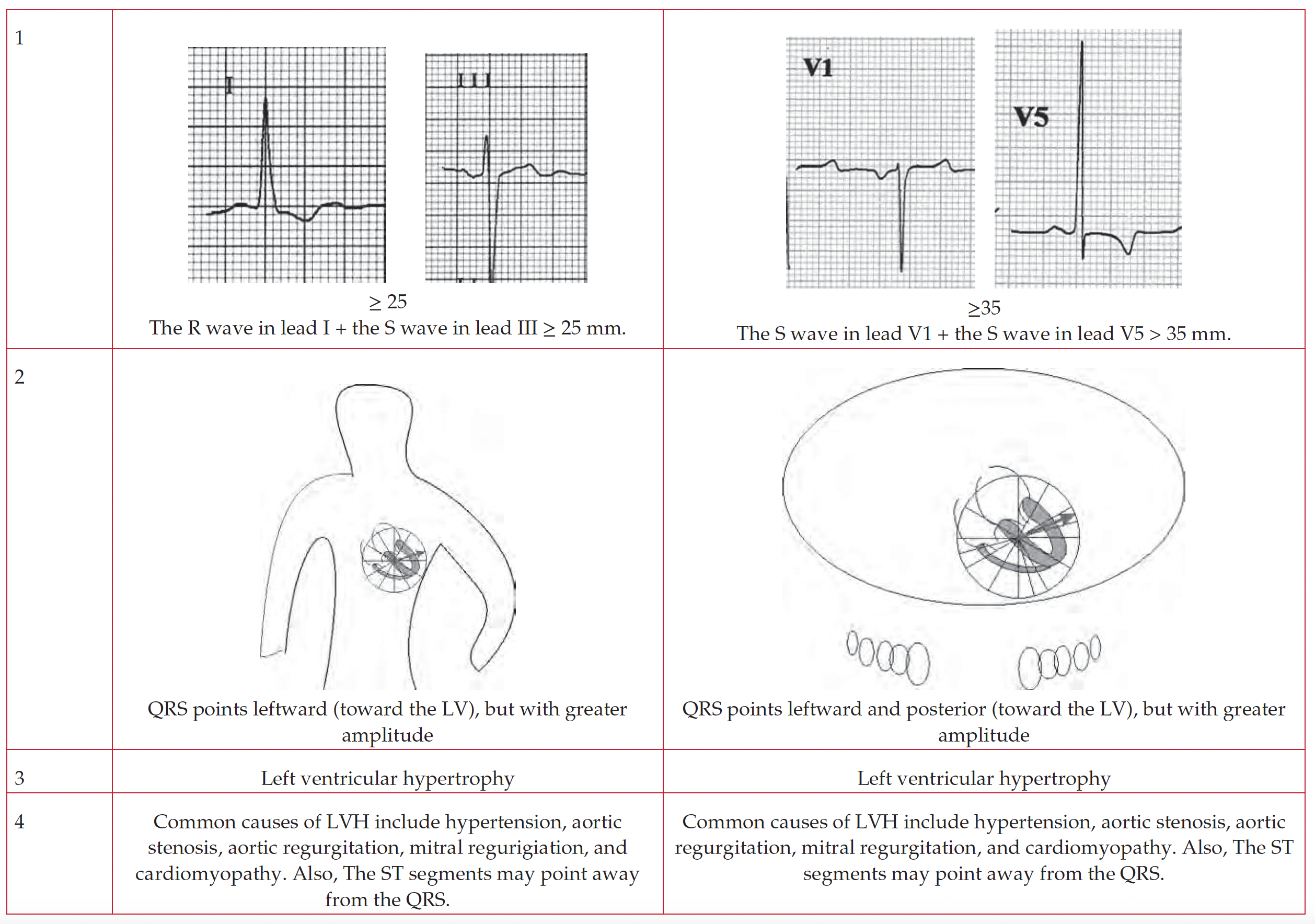
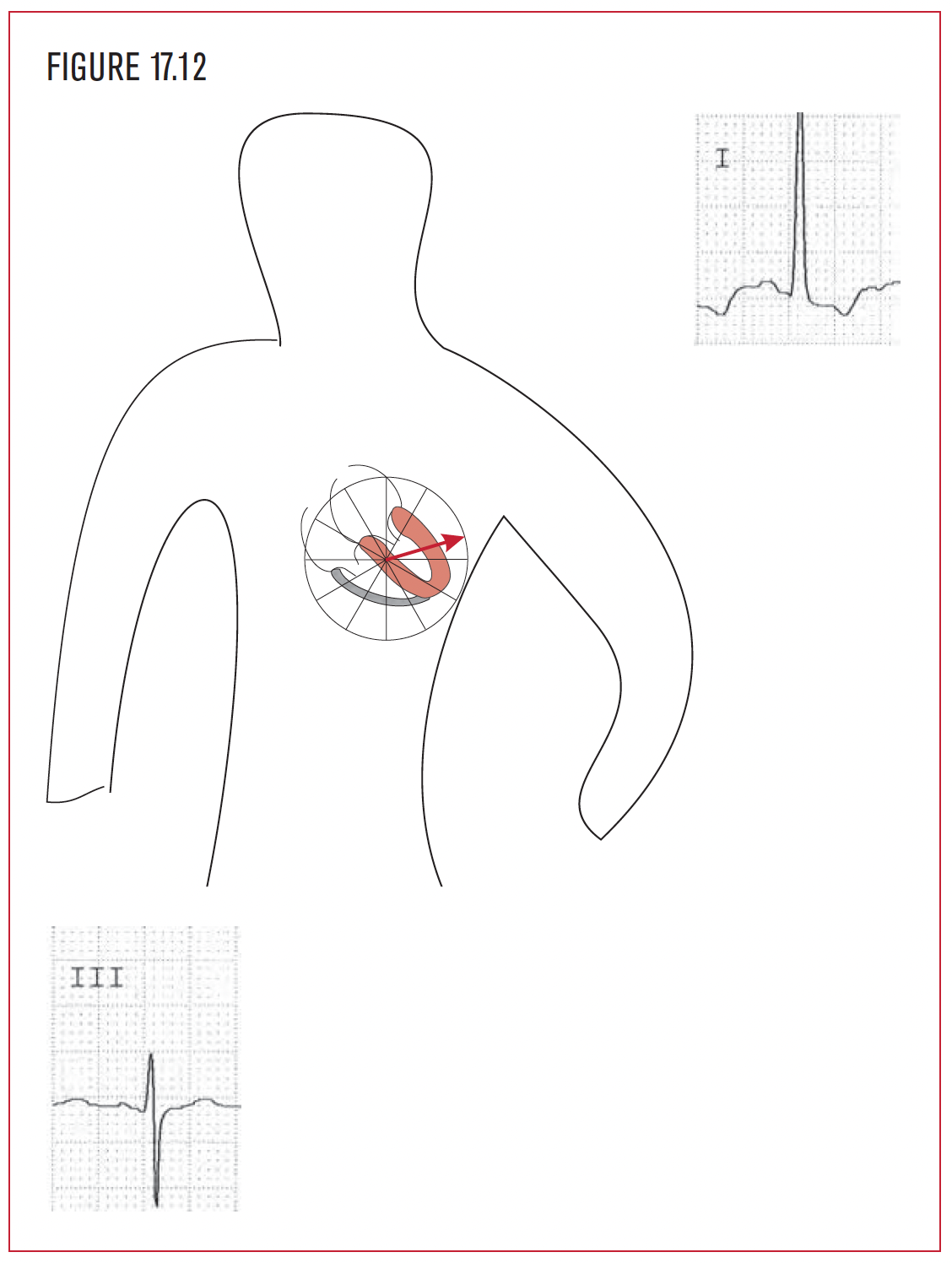
Criteria: The depth of the S wave in lead III added to the height of the R wave in lead I equals 25 little boxes or more. (Here the sum is 31 little boxes.)
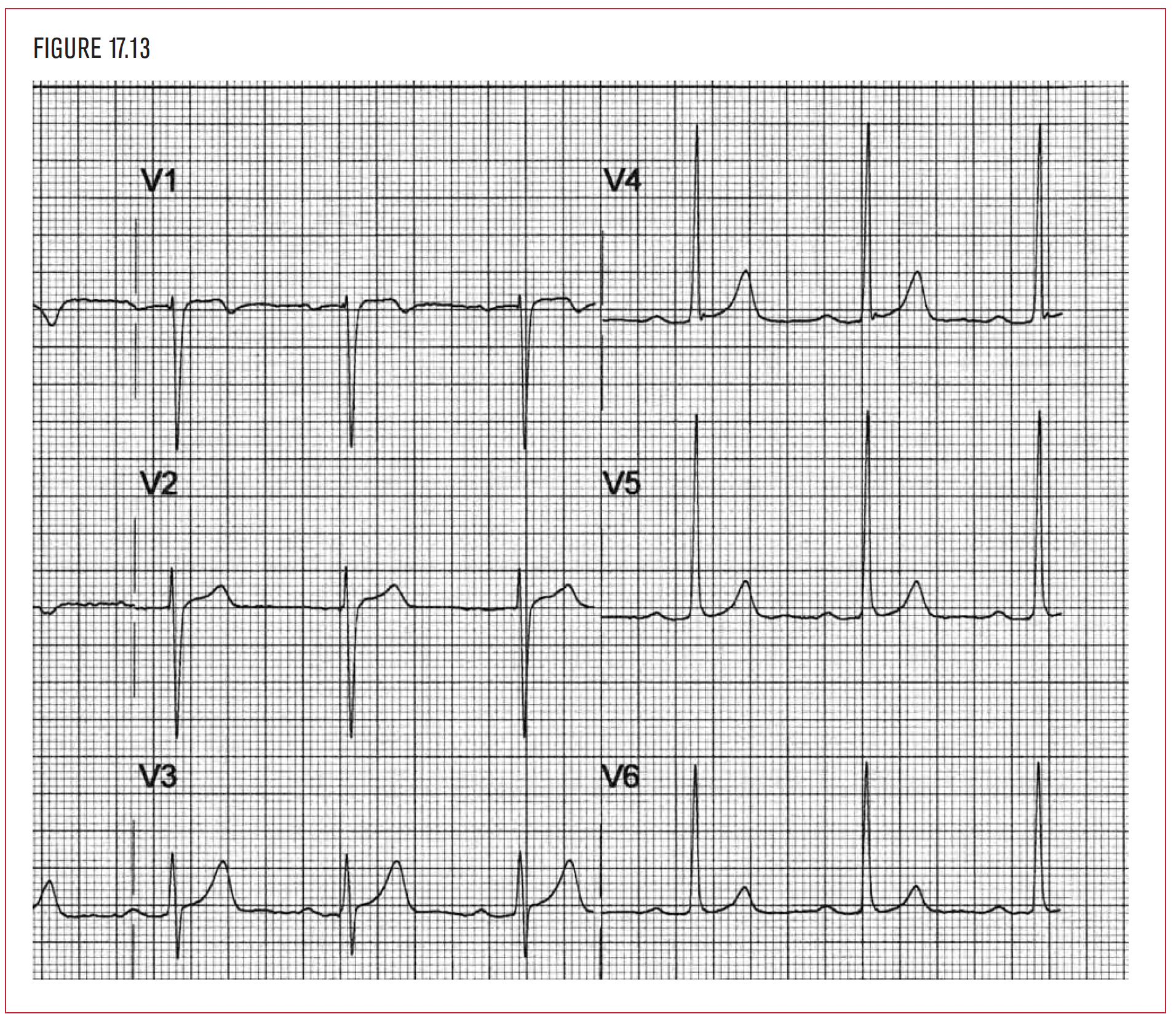
Criteria: The depth of the S wave in lead V1 added to the height of the R wave in lead V5 equals 35 little boxes or more. Here the sum is 44 little boxes.