Instructions for Chapter 16 Worksheets
- Make basic measurements and evaluate for ischemia and infarction.
- Diagnose right or left atrial abnormality based on the criteria in Chapter 16.
- Evaluate clinically.
Clinically-Based Critical Thinking: Interpretation
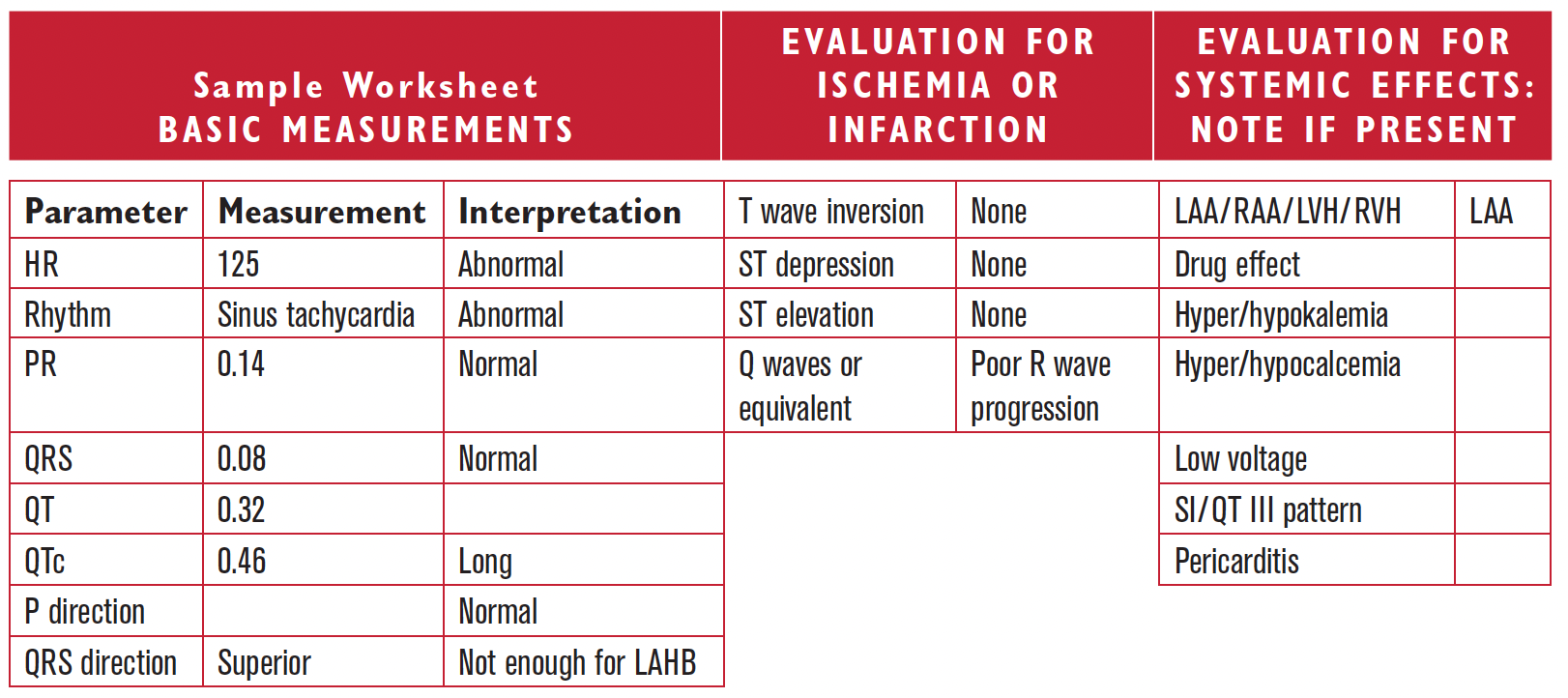
Sinus tachycardia is present and suggests sympathetic stimulation. Medications and electrolyte values should be checked to explain the long QTc. Poor R wave progression could be the result of underlying infarction or lung disease. It is not a specific finding and needs to be evaluated clinically. Left atrial abnormality is present, which may be due to left ventricular disease such as hypertensive heart disease, or systolic or diastolic heart failure. LAA can also be associated with mitral stenosis or regurgitation.