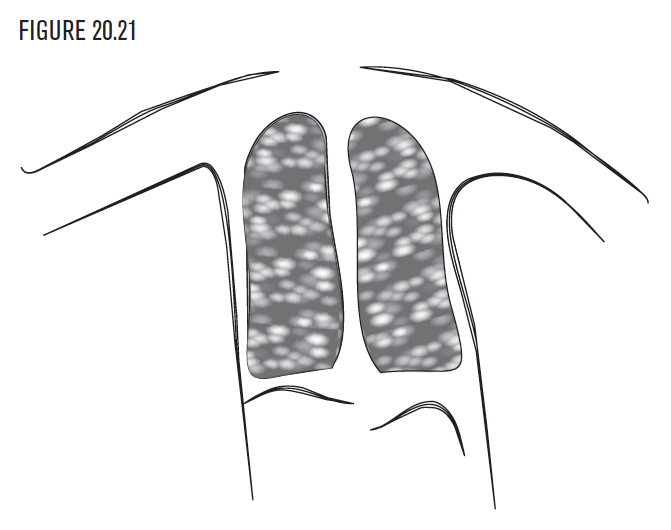
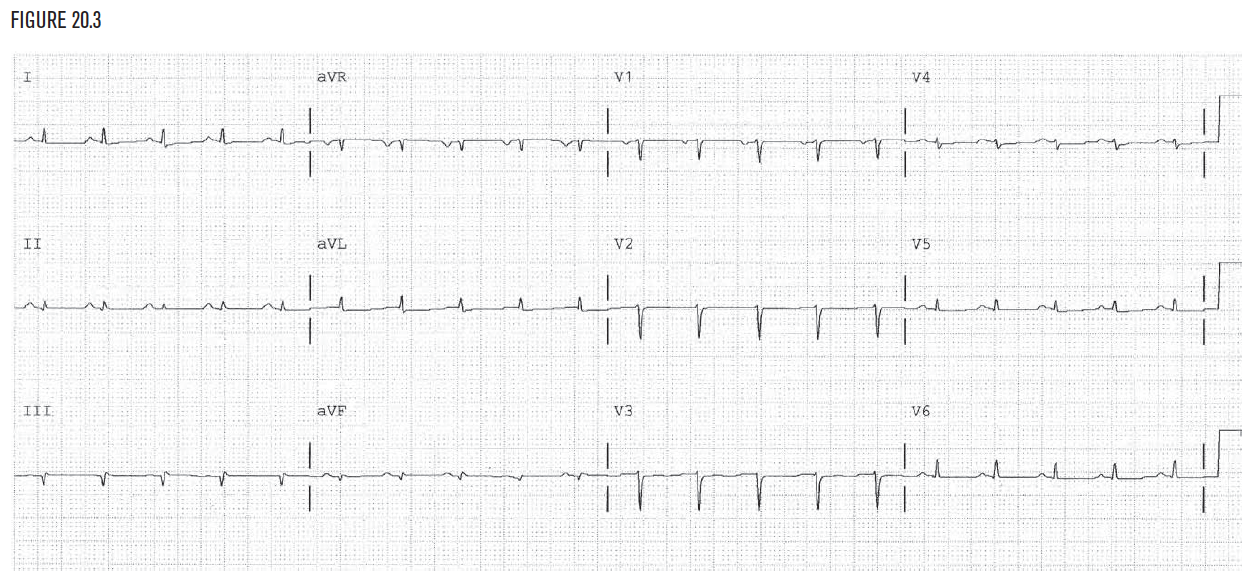
The heart lies in the chest in the mediastinum, slightly to the left of the midline. There are certain diseases and conditions that alter the normal anatomy of the chest cavity and can cause changes in the EKG. When the changes in anatomy interfere with the ability of the EKG leads to take normal measurements, a condition called low voltage can occur (Figure 20.3).
When the changes in anatomy interfere with the ability of the EKG leads to take normal measurements, a condition called low voltage can occur (Figure 20.3).
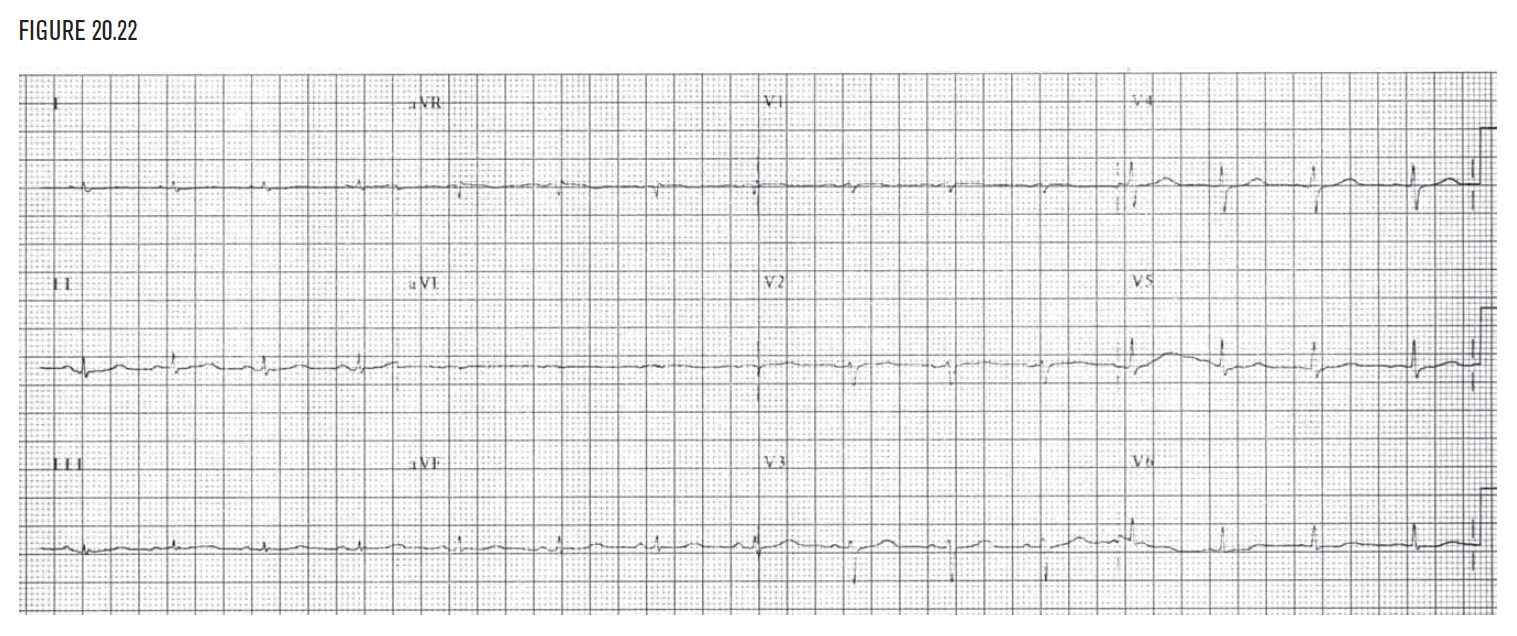
Low voltage is present in the frontal plane if the sum of the QRS amplitudes in leads I, II, and III (ie, I + II + III) is less than 15 little boxes. Similarly, low voltage is present in the horizontal plane if the QRS amplitude does not reach 15 little boxes in at least one of leads V1, V2, or V3. Some examples of this are pneumothorax, large pleural effusion, obstructive lung disease, infiltrative cardiomyopathies, and dextrocardia.
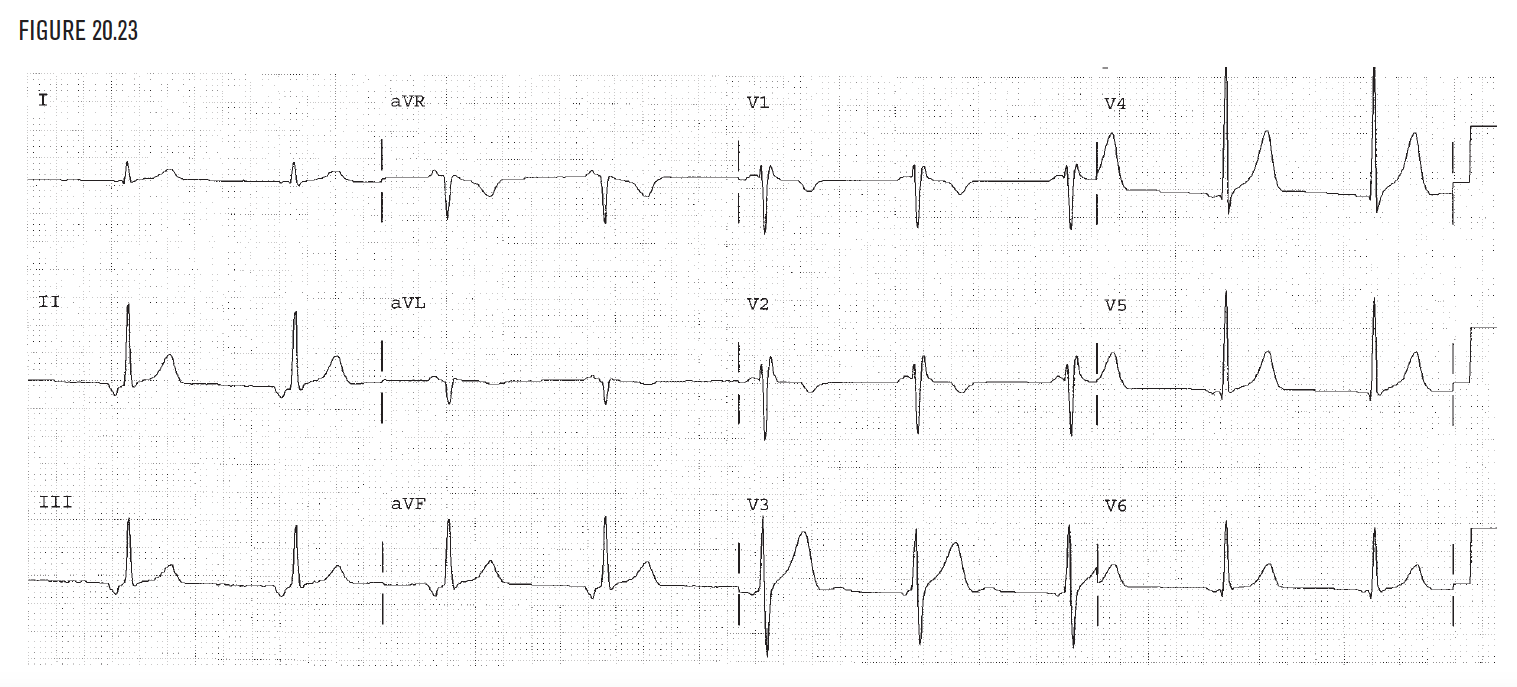
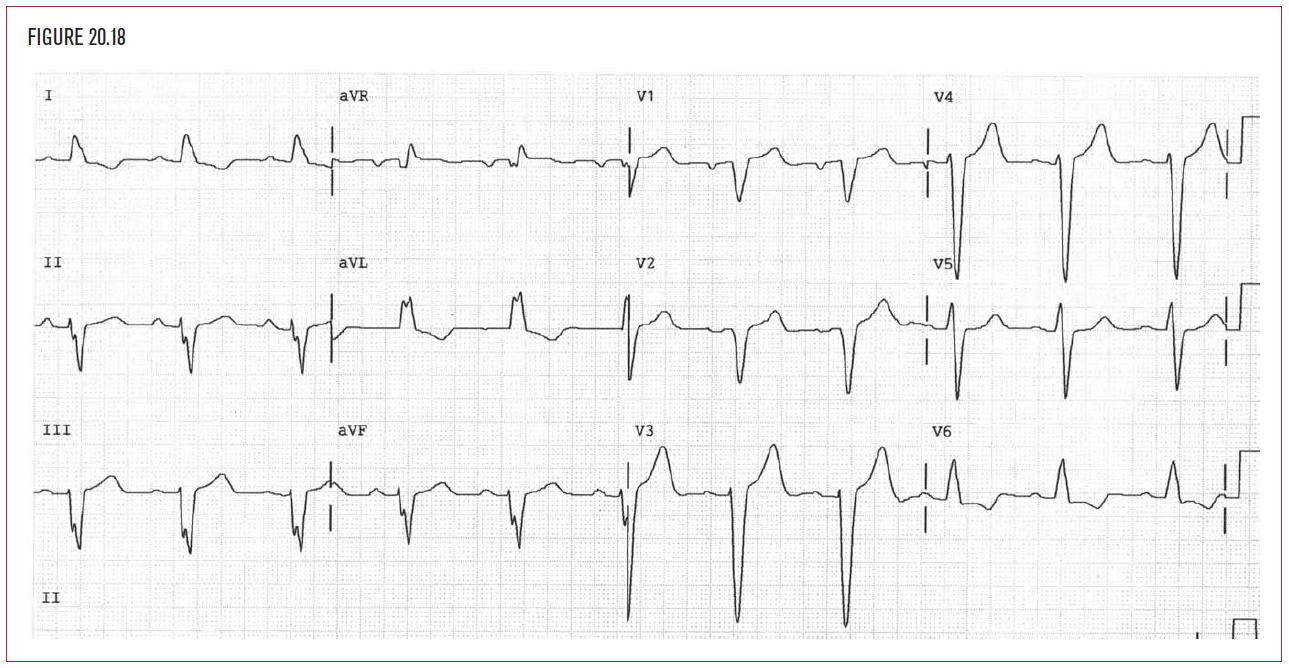
The EKG demonstrates abnormalities in many of the cardiomyopathies. Dilated cardiomyopathy is the diagnostic term used to describe a dilated and diffusely weakened heart muscle.  Although in most cases the cause of cardiomyopathy is unknown, there are certain diseases, such as hypertension, viral infections, and alcoholism that may contribute to it. The EKG may demonstrate left bundle branch block (Figure 20.18). Left atrial abnormality is another helpful clue.
Although in most cases the cause of cardiomyopathy is unknown, there are certain diseases, such as hypertension, viral infections, and alcoholism that may contribute to it. The EKG may demonstrate left bundle branch block (Figure 20.18). Left atrial abnormality is another helpful clue.
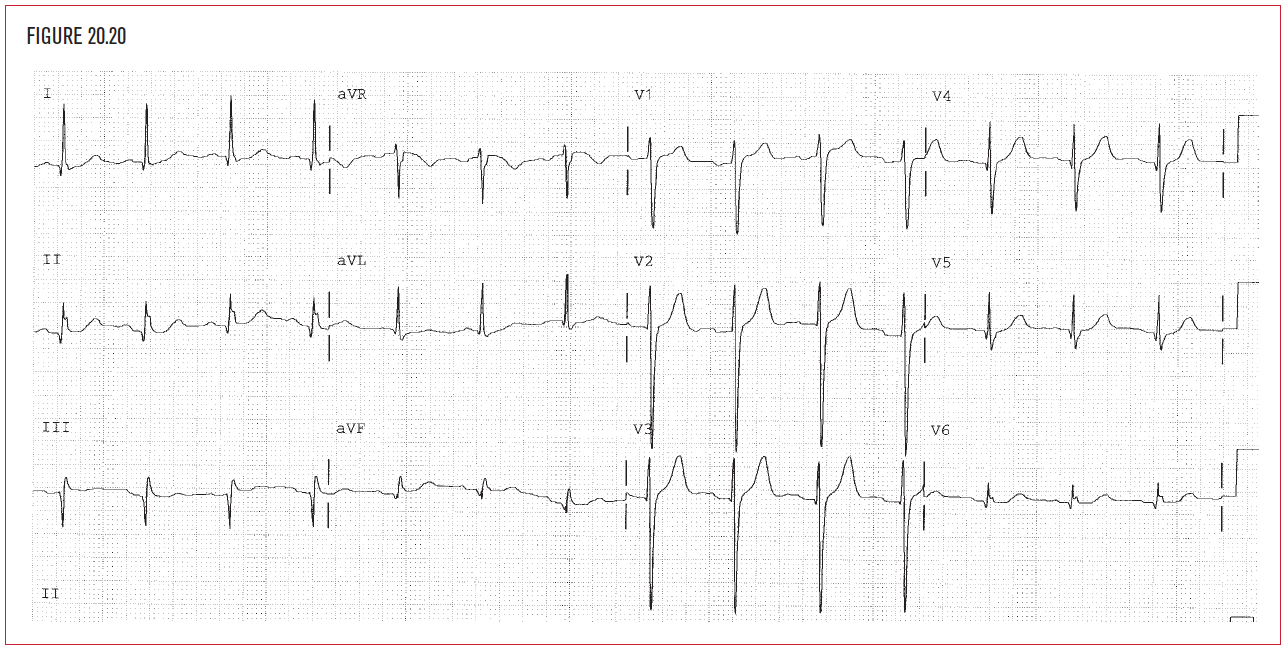
Hypertrophic cardiomyopathy is associated with sudden death. This may include asymmetric hypertrophy of the ventricular septum, which produces increased voltage and criteria for LVH on the EKG. There may be dynamic outflow obstruction below the aortic valve as well. This is due to coaptation of the anterior mitral valve leaflet against the ventricular septum. This coaptation restricts the exit of blood from the left ventricle.
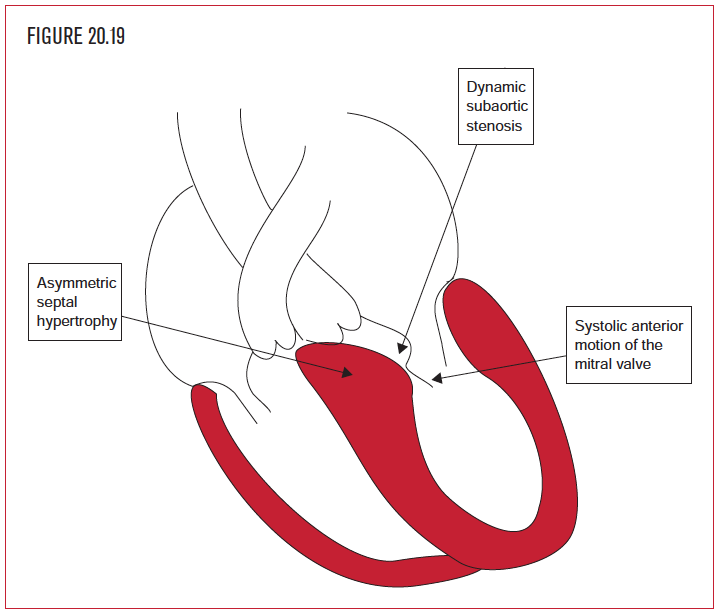 This drop in cardiac output can cause syncope, shock, or sudden death. The EKG typically shows increased voltage but no obvious universal pattern of changes has been described. The presence of EKG evidence of LVH without a history of hypertension should prompt a workup for other causes of LVH.
This drop in cardiac output can cause syncope, shock, or sudden death. The EKG typically shows increased voltage but no obvious universal pattern of changes has been described. The presence of EKG evidence of LVH without a history of hypertension should prompt a workup for other causes of LVH.