Instructions for Chapter 19 Worksheets
- Make basic measurements, evaluate for ischemia and infarction, evaluate for hypertrophy.
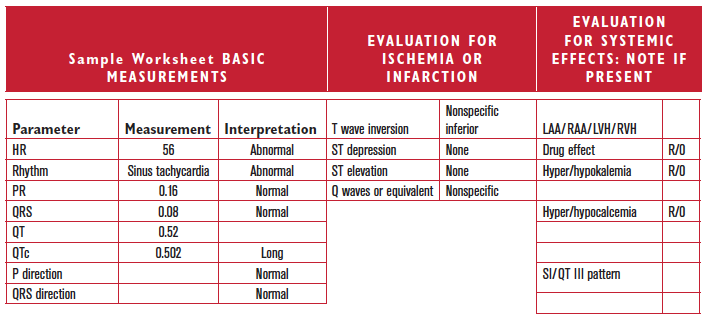
- Diagnose drug and electrolyte abnormalities as appropriate based on the heart rate, QRS, QTc, and ST segments.
- Evaluate clinically.
Clinically-Based Critical Thinking: Interpretation
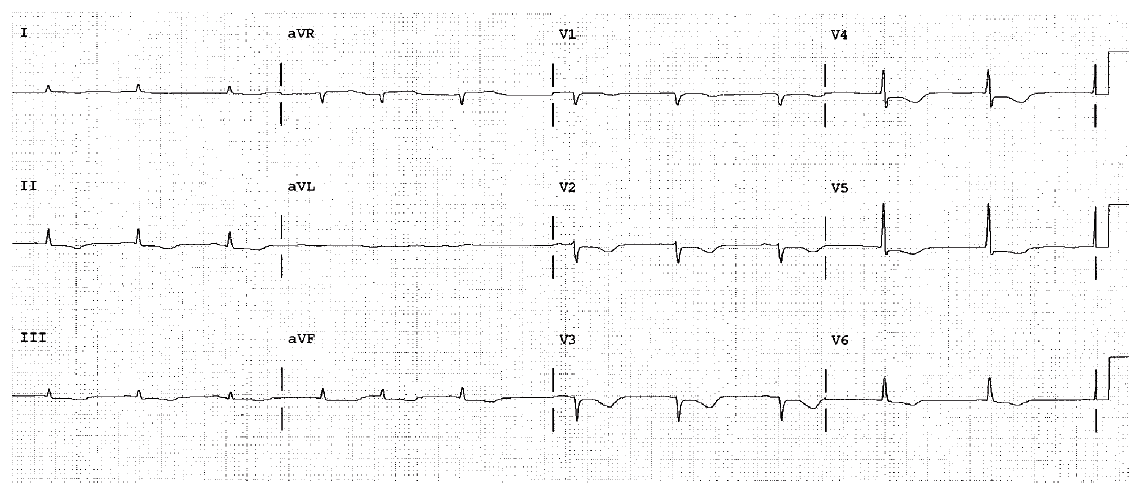
Sinus bradycardia is present. There is an abnormally long QTc. This suggests a drug toxicity or electrolyte abnormality. Antiarrhythmic therapy, hypokalemia, hypocalcemia, and so on, should be considered and ruled out as causes. The offending agent should be removed if at all possible.