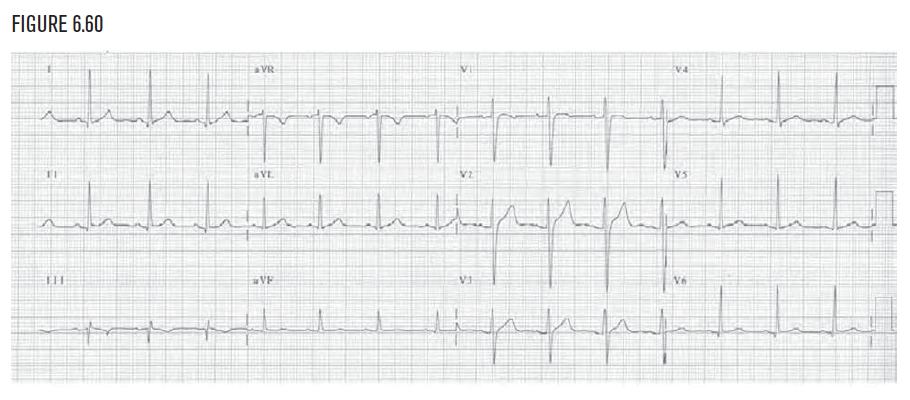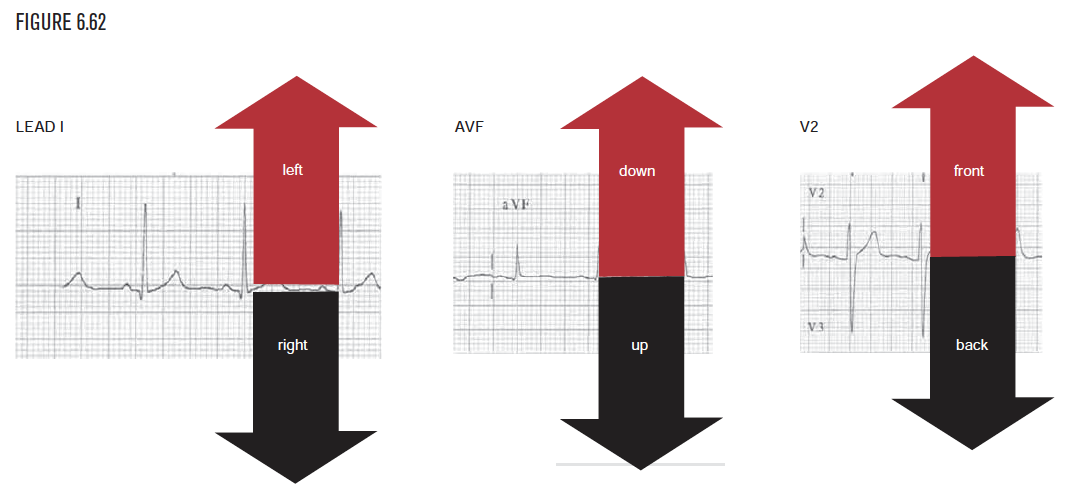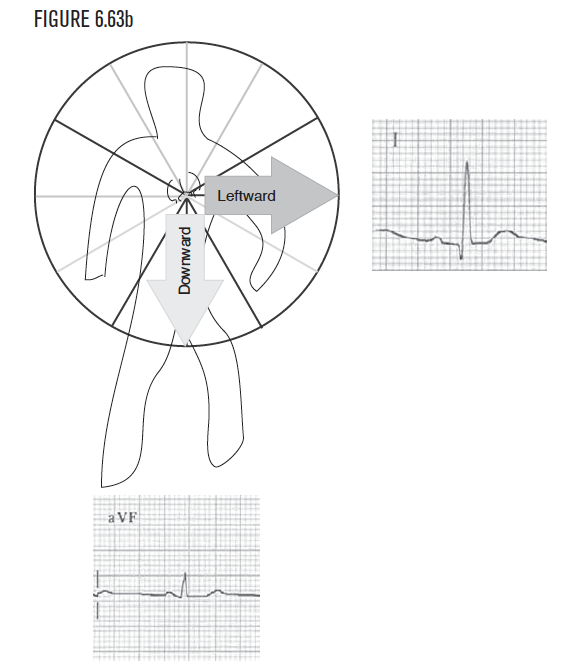
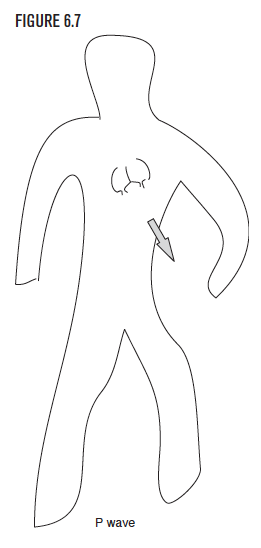

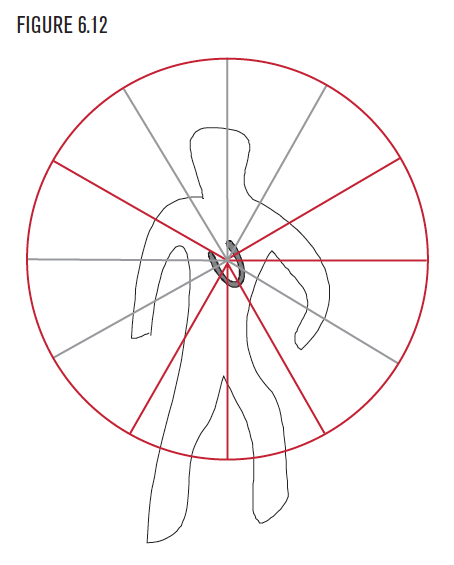
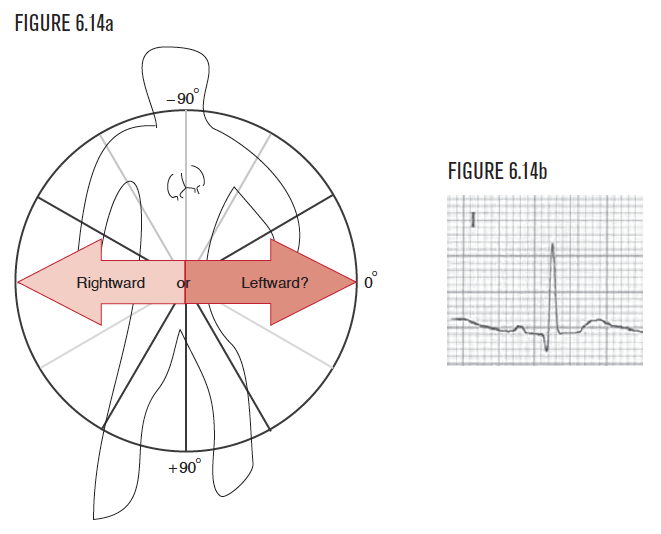
Remember that each lead is so primitive that it can “see” in only one dimension and can sense only if the electrical force is coming toward it or going away from it. Using this method, examine the P wave in lead I first. Your perspective is that of someone viewing the cardiac events from this location. The sensor at lead I is perfectly placed to provide one critical piece of information, namely whether the electrical force is pointing left or right. If the P wave (or any wave for that matter) is upright or positive, then the observer visualizes that force as pointing toward the patient’s left side. If the lead I sensor is negative or downward, the observer visualizes the force as pointing toward the patient’s right side. This concept of “positive = toward” and “negative = away” relative to any of the EKG leads is fundamental to visualizing direction.
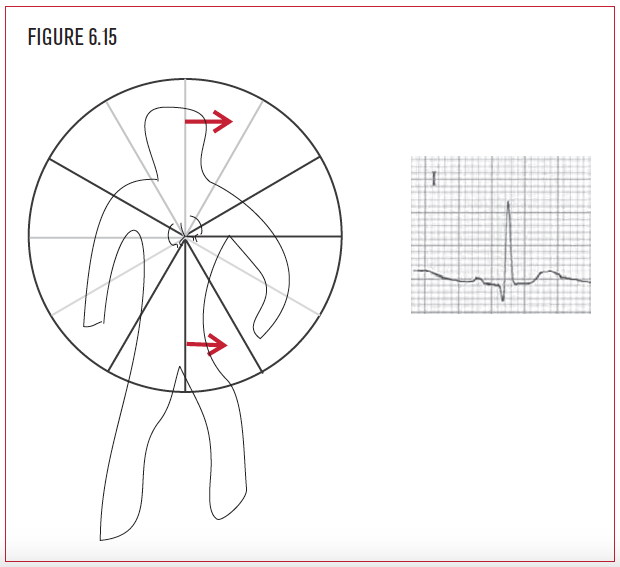
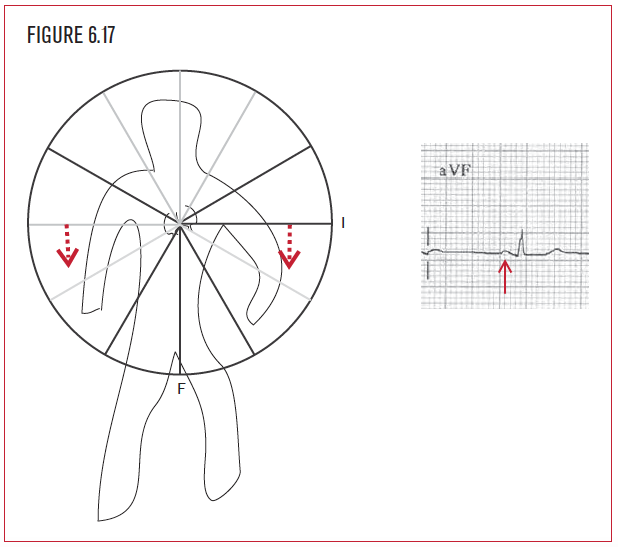
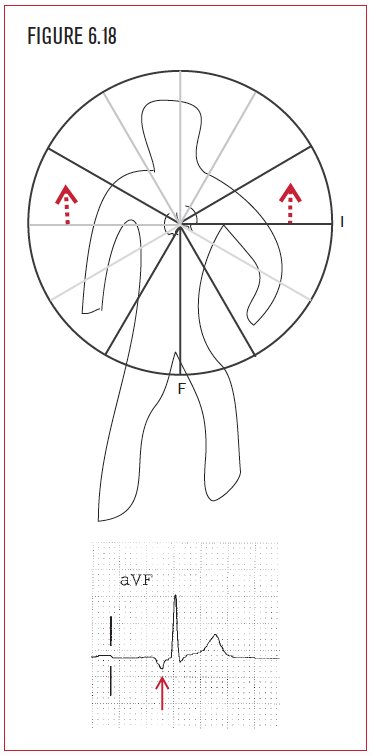
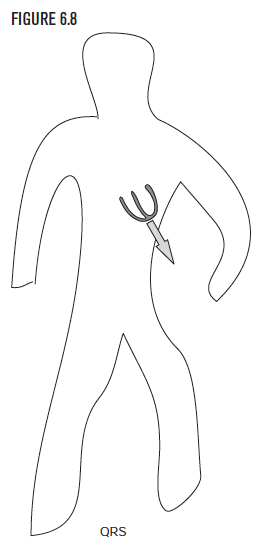
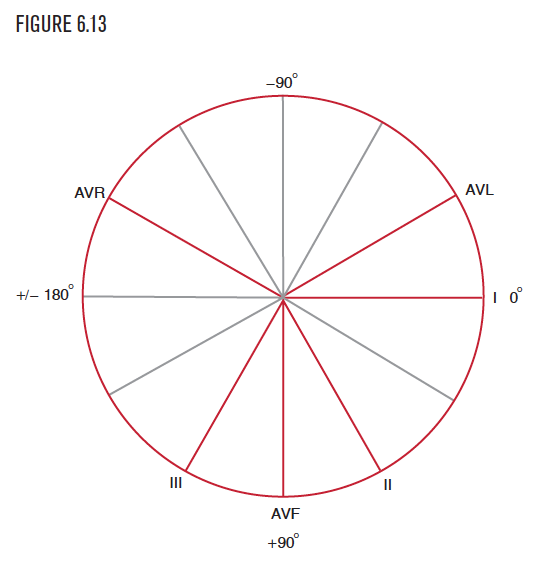
Once again, remember that each of the 12 EKG leads is so primitive it can “see” only in one dimension and can sense only if an electrical force is coming toward it or going away from it. Lead I has already let the observer visualize whether the force is pointing right or left. Lead AVF is the sensor below the patient’s feet and provides the perspective of someone viewing the cardiac events from below. The sensor at lead AVF is perfectly placed to provide another critical piece of information, namely whether the electrical force is pointing up or down. If the P wave (or any wave for that matter) is upright or positive, then the observer visualizes that force as pointing toward the patient’s feet, which is where AVF is placed. If the lead AVF sensor is negative or downward, then the observer visualizes the force as pointing toward the patient’s head. Be careful with AVF! If lead AVF is up, then visualize the force as downward!