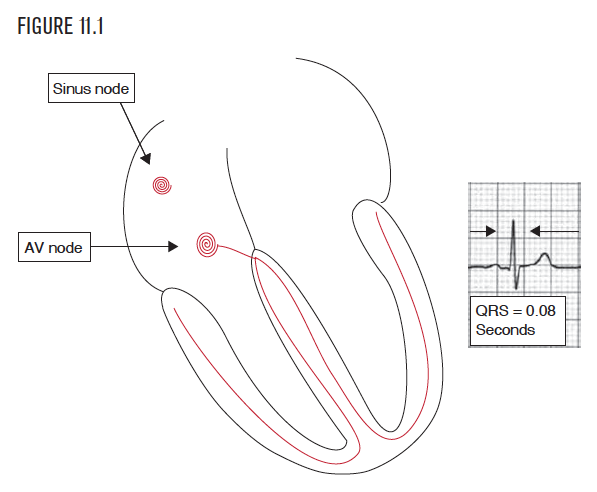
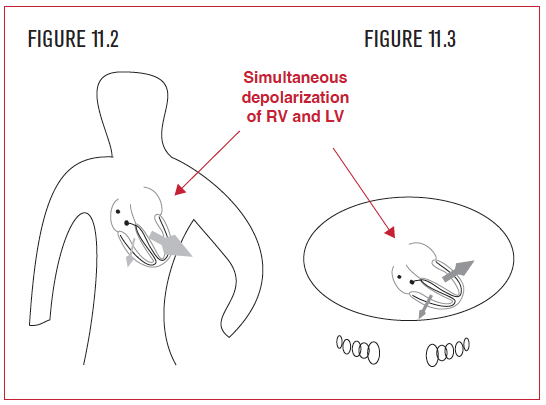
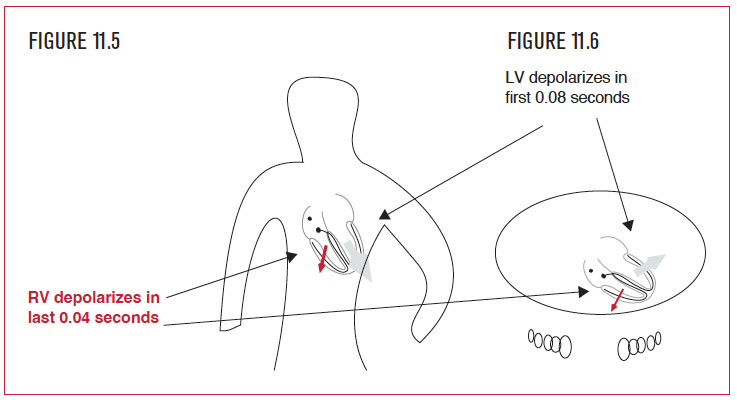
 The normal QRS complex represents combined depolarization of all the right and left ventricular cells. This normally happens, from first cell to last, in 0.08 seconds. The message to depolarize is conducted to both the right ventricle and left ventricle. The normal direction of the QRS, as was discussed in Chapter 6 and Chapter 11, is toward the left ventricle apex, inferiorly and to the left. This is because the left ventricle has more mass than the right ventricle. This bigger mass creates a bigger electrical force on the EKG than the smaller right ventricle. Both ventricles normally depolarize at the same time, and so the left ventricular component of the total electrical force overshadows the much smaller right ventricular force. In the frontal view, the QRS points to the patient’s left side, which is upward in lead I. In the horizontal view (from above), the direction of the QRS points posteriorly, which is negative in lead V2. (Review Figure 6.63.)
The normal QRS complex represents combined depolarization of all the right and left ventricular cells. This normally happens, from first cell to last, in 0.08 seconds. The message to depolarize is conducted to both the right ventricle and left ventricle. The normal direction of the QRS, as was discussed in Chapter 6 and Chapter 11, is toward the left ventricle apex, inferiorly and to the left. This is because the left ventricle has more mass than the right ventricle. This bigger mass creates a bigger electrical force on the EKG than the smaller right ventricle. Both ventricles normally depolarize at the same time, and so the left ventricular component of the total electrical force overshadows the much smaller right ventricular force. In the frontal view, the QRS points to the patient’s left side, which is upward in lead I. In the horizontal view (from above), the direction of the QRS points posteriorly, which is negative in lead V2. (Review Figure 6.63.)
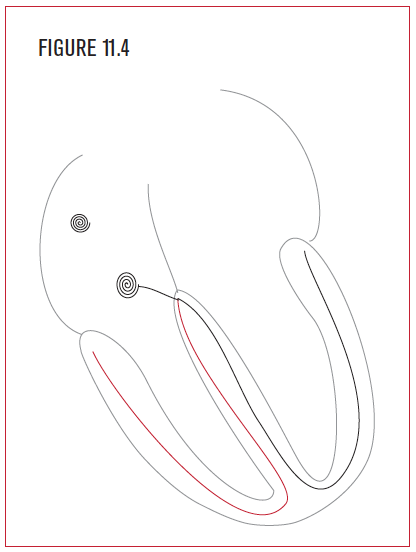 In right bundle branch block, this all changes. The ventricles are not depolarized at the same time, but in sequence—first the left ventricle, then the right ventricle. The sequence begins with the left bundle, since it is functioning normally. It depolarizes the whole left ventricle in the normal amount of time, which is less than 0.10 seconds.
In right bundle branch block, this all changes. The ventricles are not depolarized at the same time, but in sequence—first the left ventricle, then the right ventricle. The sequence begins with the left bundle, since it is functioning normally. It depolarizes the whole left ventricle in the normal amount of time, which is less than 0.10 seconds.
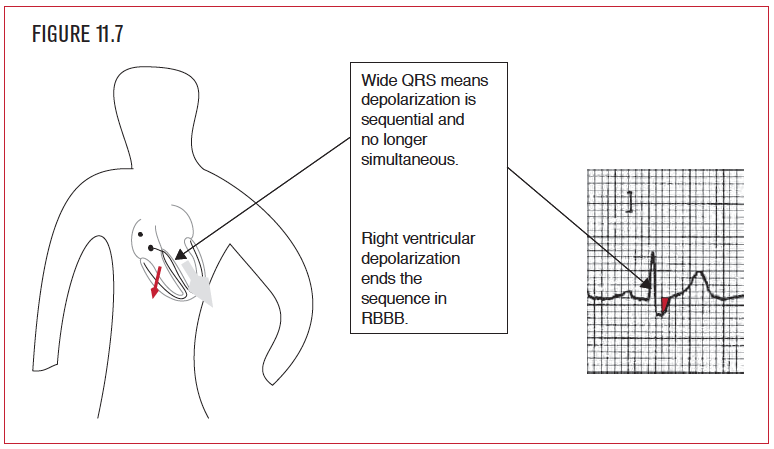
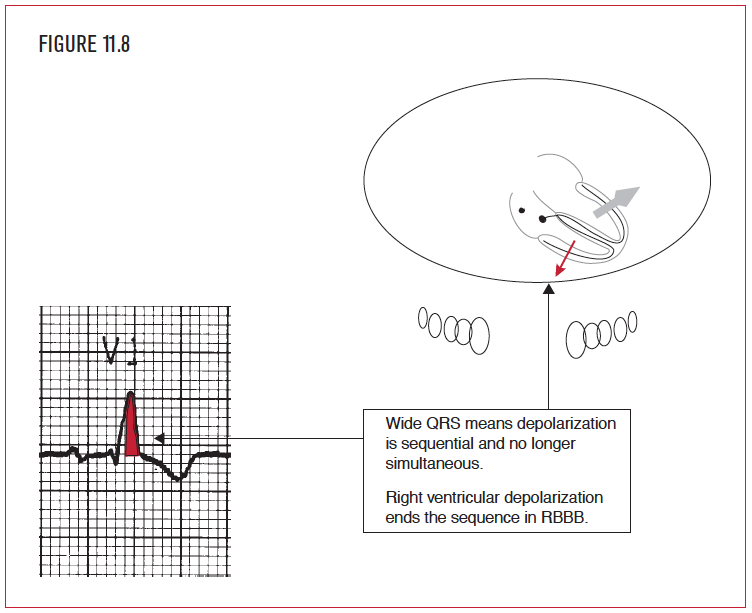
The rest of the QRS after that first 0.08 seconds represents only right ventricular activation. (The whole left ventricle was finished depolarizing in the first 0.08 seconds.) This is the second part of the sequence, depolarization of the right ventricle from the efforts of the left bundle. Since the depolarization of both ventricles is not simultaneous but sequential, it takes longer to finish, 50% longer to finish compared with the normal QRS of 0.08 seconds. Prolongation of the QRS interval to 0.12 seconds or more is the diagnostic signature of bundle branch block. This sequential depolarization allows for the second hallmark of RBBB, namely, that the last part of the depolarization sequence (the QRS) must be right ventricular in direction. In RBBB, the left bundle finishes off ventricular activation on the right side, so the QRS ends in the right ventricle, a direction that is rightward and anterior.
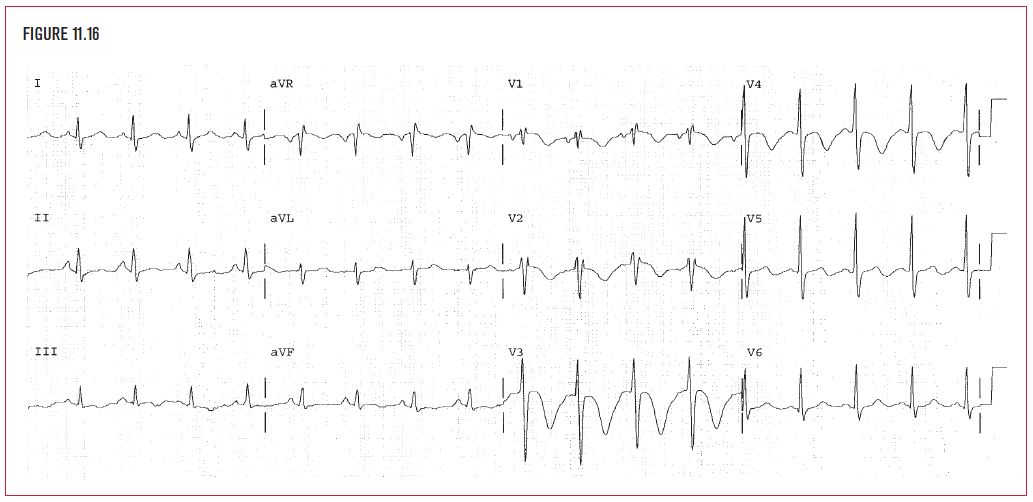
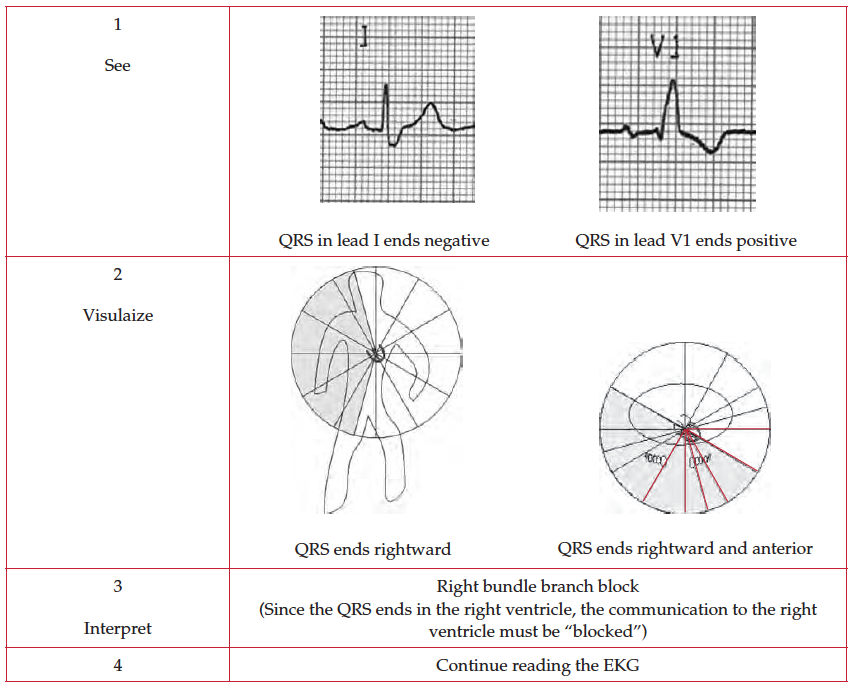
Prolongation of the QRS interval to 0.12 seconds or more is the diagnostic signature of bundle branch block. This sequential depolarization allows for the second hallmark of RBBB, namely, that the last part of the depolarization sequence (the QRS) must be right ventricular in direction. In RBBB, ventricular activation finishes on the right side, so the QRS ends in the right ventricle, a direction that is toward the patient’s right side and anterior. When the QRS interval is 0.12 seconds or more, bundle branch block is present. Visualize the direction of the end of the QRS in lead I. Since it is negative, it points to the right ventricle and RBBB is present.
Prolongation of the QRS interval to 0.12 seconds or more is the diagnostic signature of bundle branch block. This sequential depolarization allows for the second hallmark of RBBB, namely, that the last part of the depolarization sequence (the QRS) must be right ventricular in direction. In RBBB, ventricular activation finishes on the right side, so the QRS ends in the right ventricle, a direction that is toward the patient’s right side and anterior. When the QRS interval is 0.12 seconds or more, bundle branch block is present. Visualize the direction of the end of the QRS in lead V1. Since it is positive, it points to the right ventricle, and RBBB is present.
- The QRS interval is 0.12 seconds or longer.
- The last part of the QRS is moving toward the right ventricle, which is right and anterior.
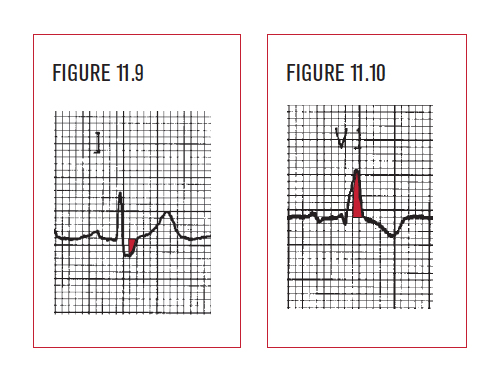
- Limb Leads: The QRS ends in an S wave in lead I, and in V6. This is a rightward direction (Figure 11.9).
- Horizontal Leads: The QRS ends in an R or R’ wave in lead V1. This is an anterior and rightward direction (Figure 11.10).
Critical Point: The first half of the QRS is irrelevant in making the diagnosis of RBBB!
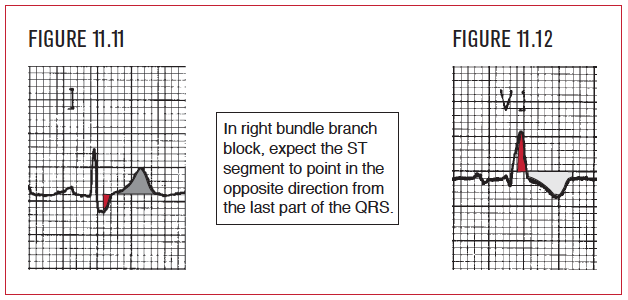
In RBBB, the ST segment is predictably abnormal and points away from the right ventricle. In Figure 11.11, the last part of the QRS is negative in lead I, so the ST segment should point away from this, or manifest ST segment elevation in that lead. In lead V1 (Figure 11.12), the last part of the QRS is positive, so the ST segment should point away from that, or manifest ST segment depression. In RBBB, the formation of the QRS is sequential. Because of this, do not diagnose right ventricular hypertrophy in the setting of RBBB. All other parts of the EKG, particularly hemiblock, ischemia, and infarction, can be diagnosed and should be evaluated.
Less than total loss of function in either the right or left bundle is called intraventricular conduction delay (IVCD) or incomplete RBBB. The primary diagnostic EKG abnormality in IVCD is prolongation of the QRS interval to 0.10 or 0.11 seconds. As in bundle branch block, IVCD may be left, right, or indeterminate. Once the QRS interval is measured at 0.10 or 0.11 seconds, it is the end of the QRS that is the key to diagnosis. If the end of the QRS is rightward (negative in lead I) and toward the right ventricle (positive in lead V1), then RIVCD is present.