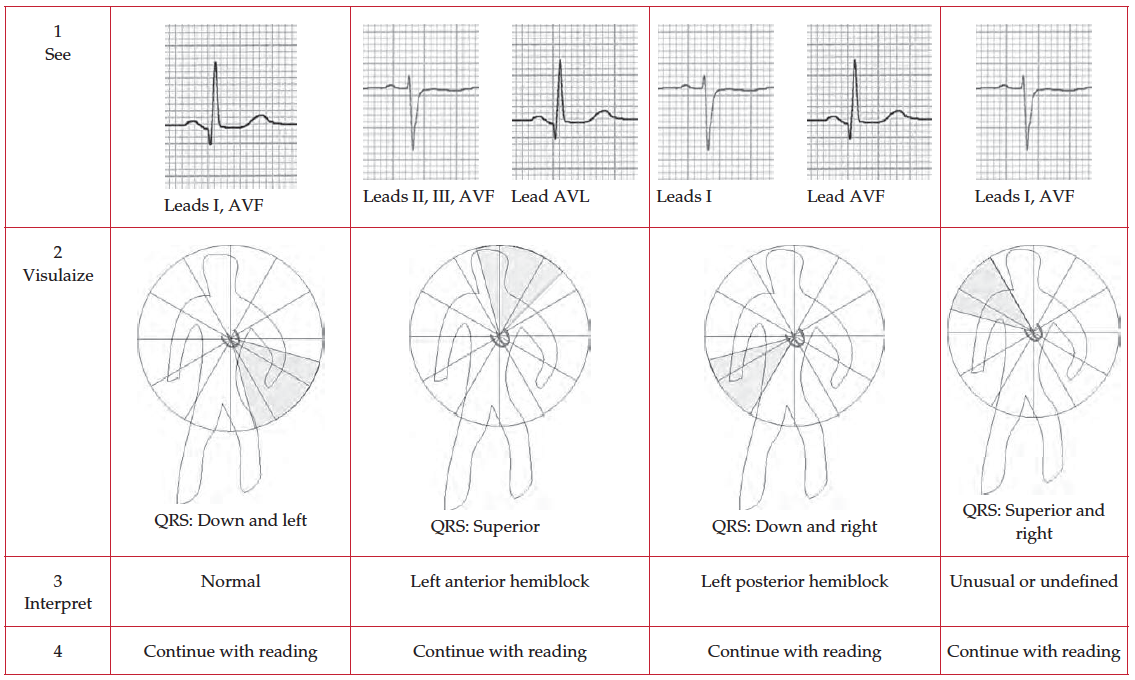
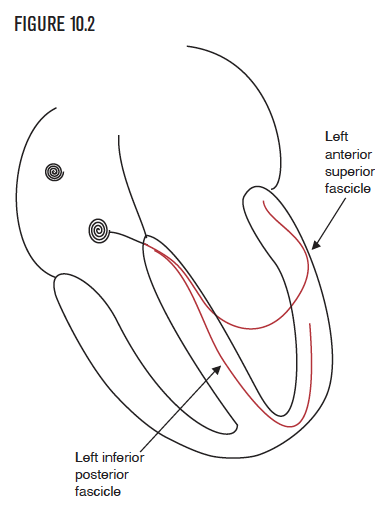
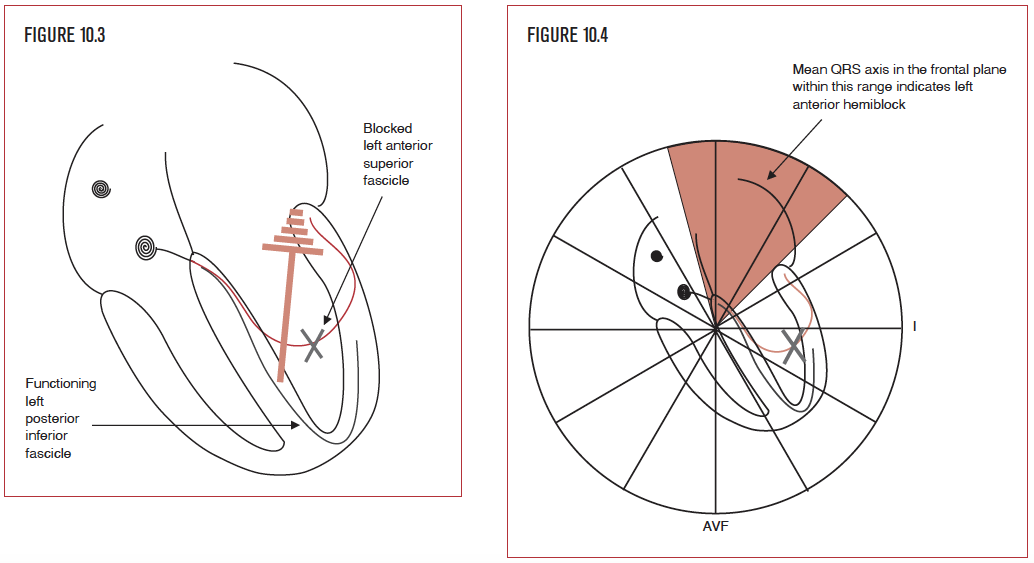
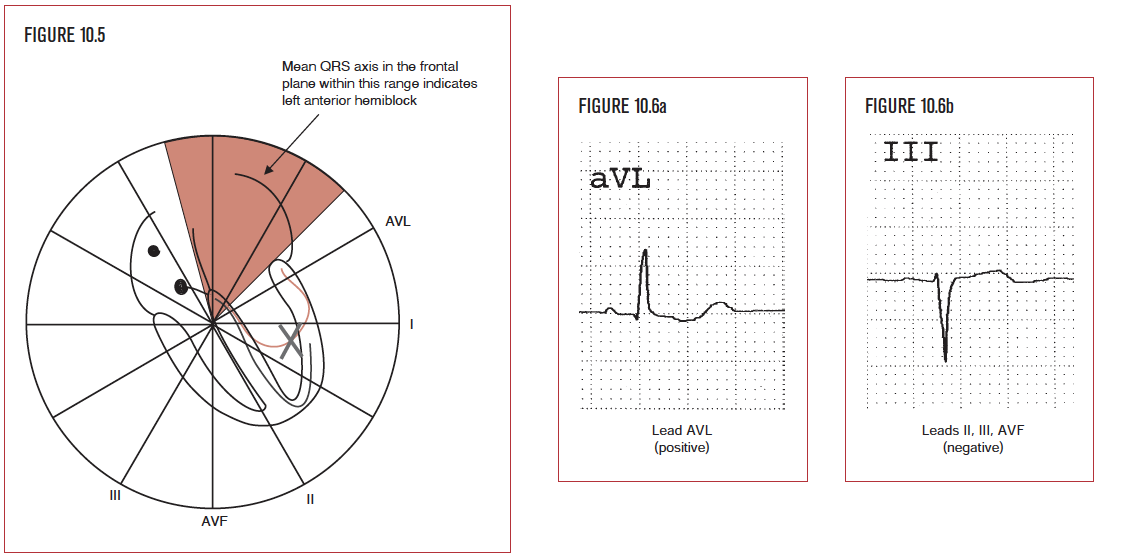
Left anterior hemiblock (LAHB) occurs when there is a loss of function in the anterior branch or fascicle of the left bundle branch (Figure 10.3). It is diagnosed by evaluating the mean QRS axis, or direction, in the frontal plane. The normal QRS direction is from the AV node toward the apex of the heart, that is inferiorly and to the patient’s left side. Left anterior hemiblock shifts the mean QRS axis upward and leftward (Figure 10.4). This occurs because the electrical impulse from the left inferior fascicle spreads superiorly and to the left to depolarize the entire left ventricle since the left anterior branch is unable to do so. Left anterior hemiblock is sometimes called left anterior superior hemiblock (LASH), which calls attention to the diagnostic trademark of LAHB, namely a superior QRS direction in the frontal plane. The two terms are synonymous. Of note, hemiblock does not significantly increase the duration of the QRS interval because each side of the heart has one functioning fascicle.
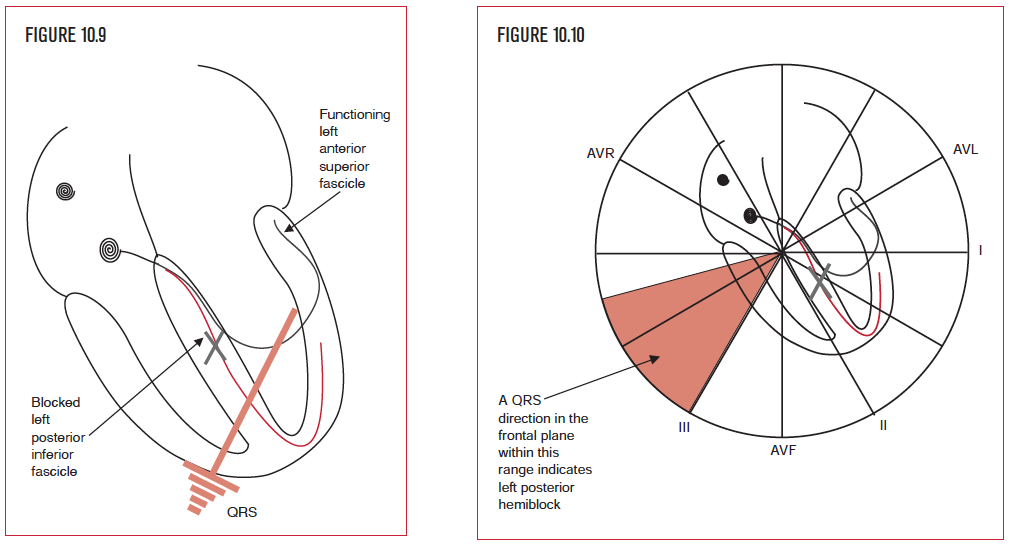
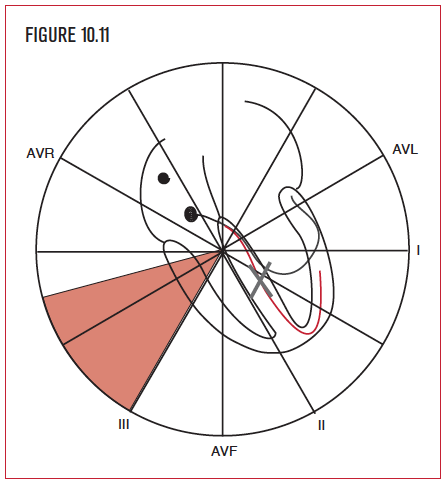
The second type of hemiblock is called left posterior hemiblock (LPHB). It occurs when there is a loss of function in the posterior part or fascicle of the left bundle branch. Like LAHB, it is diagnosed by evaluating the mean QRS axis or direction in the frontal plane. The normal QRS direction is from the AV node toward the apex of the heart, that is inferiorly and to the patient’s left side. Left posterior hemiblock shifts the mean QSR axis to the patient’s right side. This occurs because the electrical impulse from the left anterior fascicle spreads inferiorly and to the right to depolarize the entire left ventricle since the left posterior branch is unable to do so. Left posterior hemiblock is sometimes called left inferior posterior hemiblock (LIPH), which calls attention to the diagnostic trademark of LIPH, namely an inferior and rightward QRS direction in the frontal plane. The two terms are synonymous. Again, hemiblock does not significantly increase the duration of the QRS interval since each side of the heart has one functioning fascicle.