1° AV block is an abnormally long delay in the transmission of the atrial impulse through the AV node. It causes a prolongation of the PR interval to greater than 0.20 seconds. In Figure 9.2, the PR interval is 0.26 seconds long. Associations include sick sinus syndrome, drugs such as digitalis, calcium channel blockers, and antiarrhythmics.

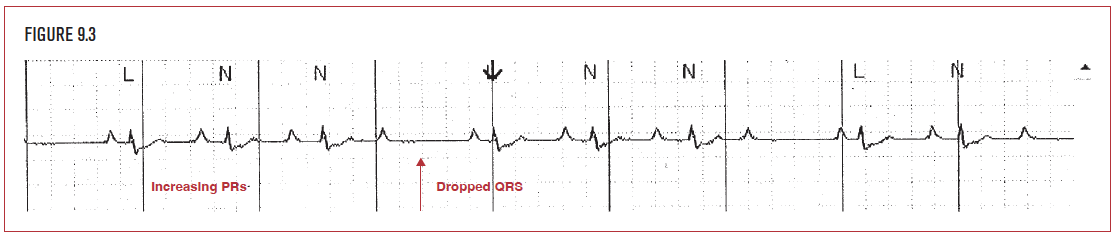
2° AV block is a more severe form of conduction abnormality in the AV node. It is characterized by a P wave that “gets lost” in the AV node and never generates a QRS complex on the EKG. There are two types of 2° AV block: Wenckebach (Type I) and Mobitz (Type II). Wenckebach is characterized by an increasing PR interval leading up to a dropped or nonconducted P wave, as shown in Figure 9.3. Because a grouping of 4 P waves leads to 3 QRS complexes, this is termed 4:3 Wenckebach. Type II (Mobitz) AV block is characterized by sequential P waves (usually more than two) that produce only a single QRS complex.
Pauses are most commonly caused by premature atrial contractions (PACs) that do not conduct down to the ventricle and generate a QRS complex. These are called nonconducted PACs (NCPACs). Frequently they occur during the T wave, and deform the T wave compared to normal. In Figure 9.4, the premature wave (P’) does not conduct to the ventricles and causes a pause of 2.6 seconds. Nonconducted PACs may be a sign of underlying conduction disease, such as sick sinus syndrome, particularly if they occur late in the cycle and are followed by a long pause.

Asystole is a prolonged period of no electrical activity. In Figure 9.5, for example, a sinus beat is followed by a period of 8 seconds of electrical asystole that continues until the end of the strip. Cessastion of function of the sinus node is called sinus arrest. Normally, when sinus arrest occurs, another pacemaker must take over, such as the junction (usually at an escape rate of 40–60 bpm) or the ventricles (usually at an escape rate of 30 bpm). In Figure 9.5, however, there is sinus arrest with no further pacemaker activity anywhere. This leads to asystole and cardiac arrest.

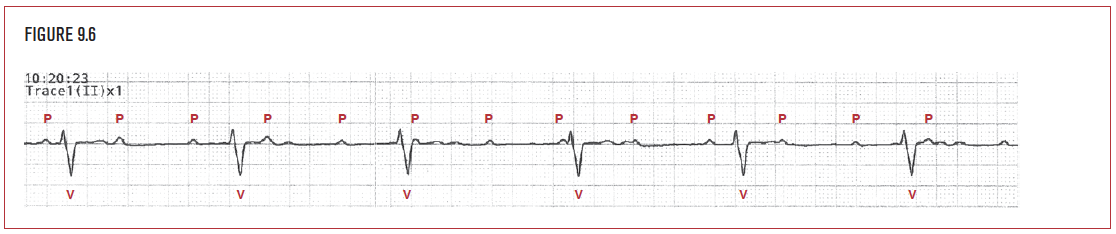
Complete heart block (CHB), also known as 3° AV block (3° AVB), describes the presence of atrial activity that does not conduct down to the ventricles on a continuing basis. Figure 9.6 demonstrates a patient with P waves (P) at a rate of 83 bpm. The P waves do not generate QRS complexes. A regular ventricular rhythm (V) at a rate of 36 bpm has come in as an escape to provide a heart beat.
Ventricular escape beats (VE) are wide QRS complexes that come late and function as a rescue rhythm of last resort for the heart. They function at a slow rate, usually in the range of 30 to 40 bpm. The ventricular escape mechanism is not as reliable a pacemaker as the sinus node or junction. It is typically associated with significantly compromised myocardium, as would be seen in cardiac arrest.
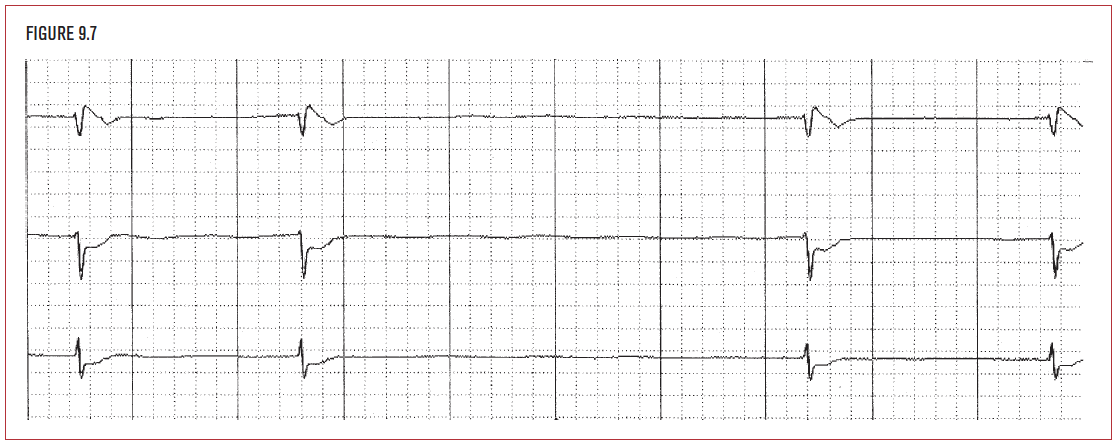
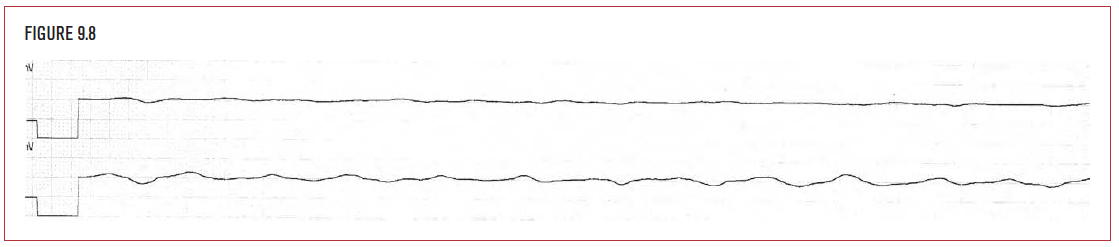
Asystole indicates the total absence of electrical activity. It has the worst prognosis of all cardiac rhythms. In Figure 9.8, the heart is unable to generate even an escape beat from the ventricles to generate a single QRS. The myocardium appears functionally dead.