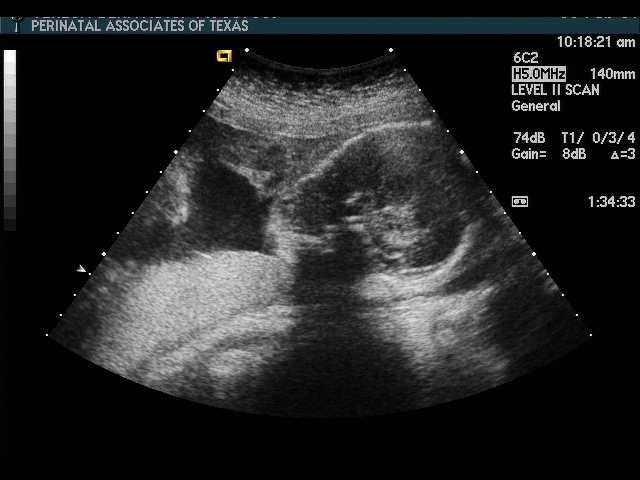
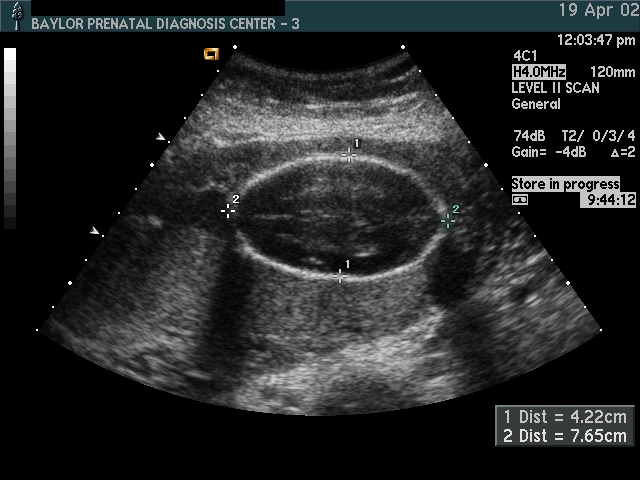
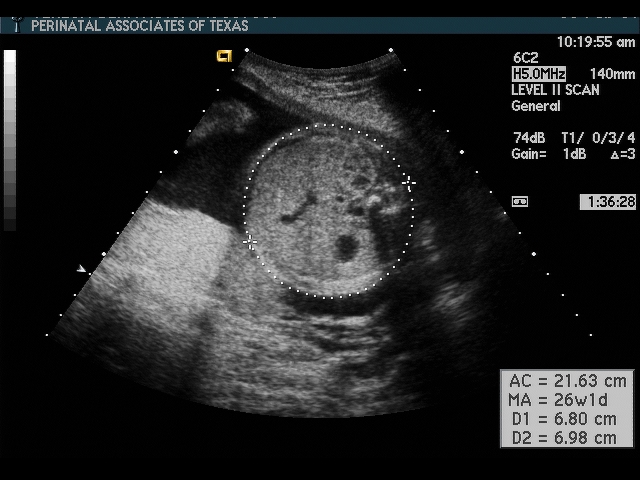
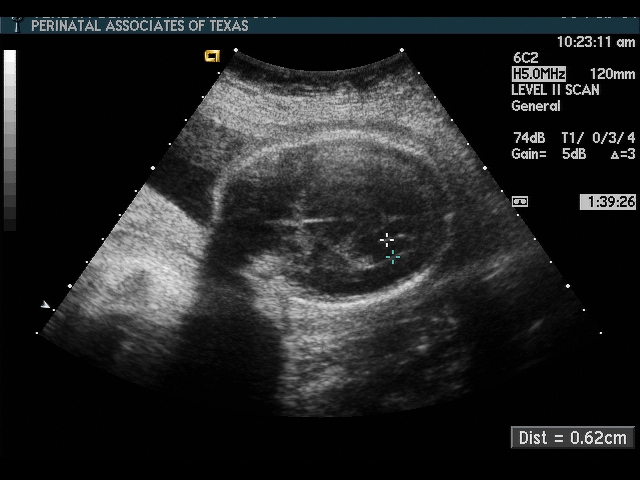
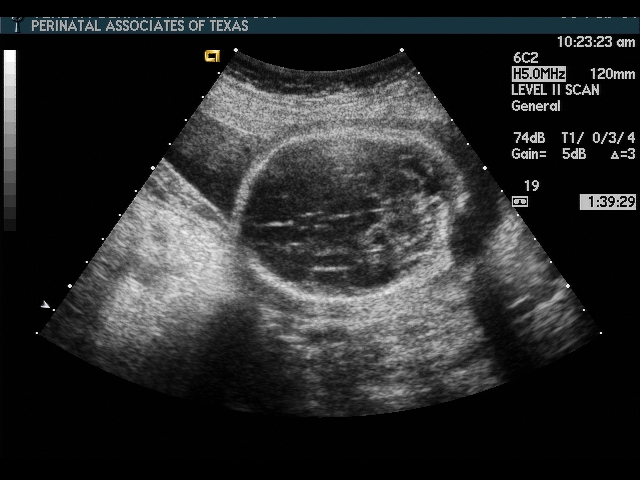
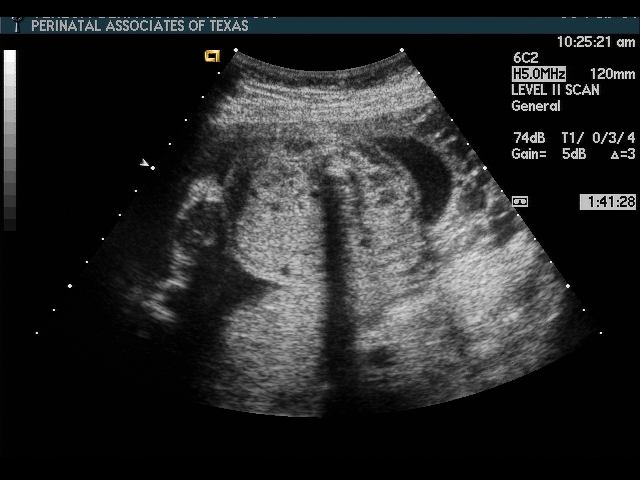
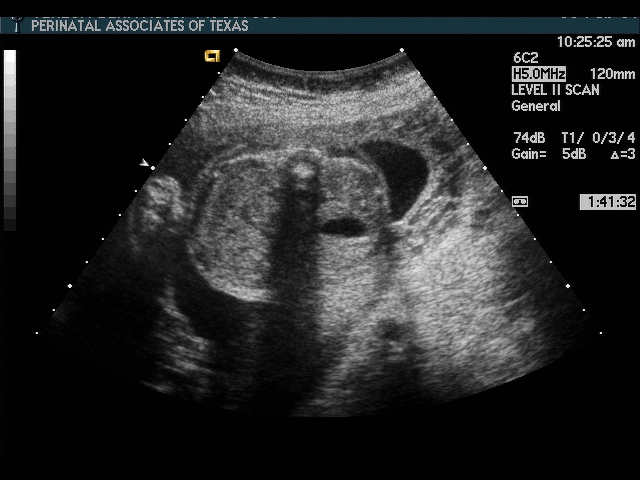
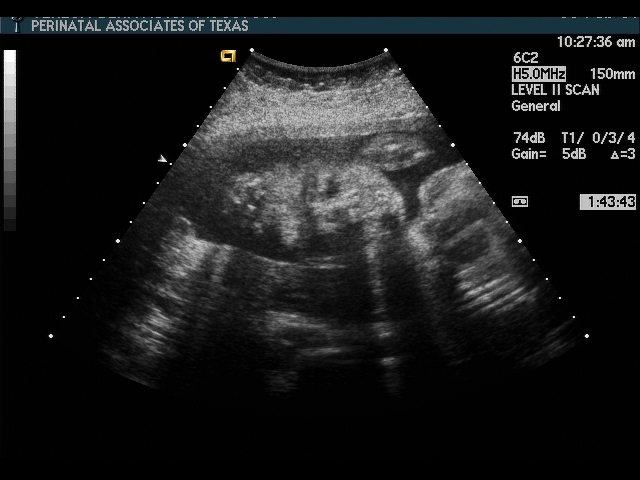
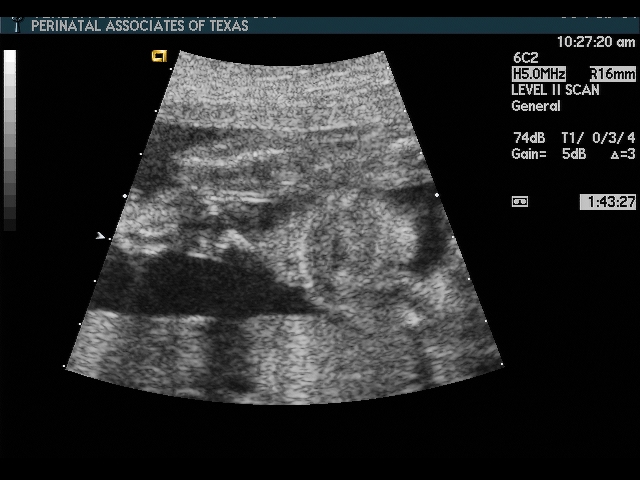
Important landmarks for a good AC:
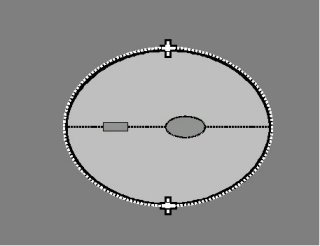
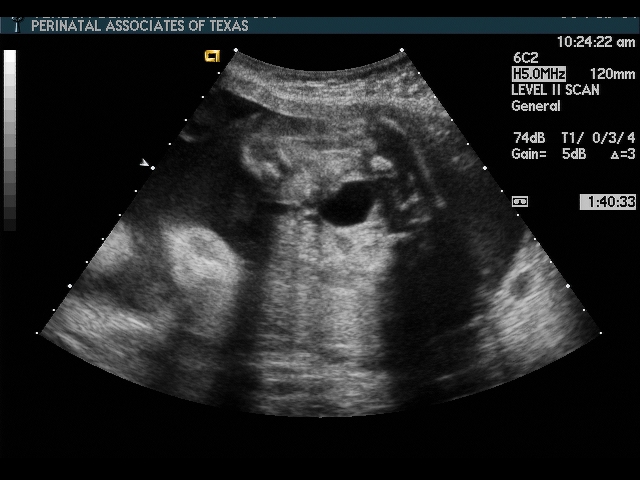
The abdomen should be as nearly circular as possible
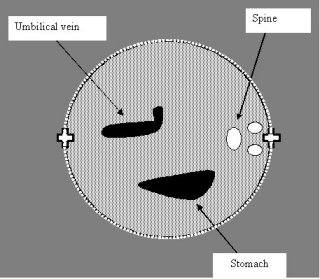
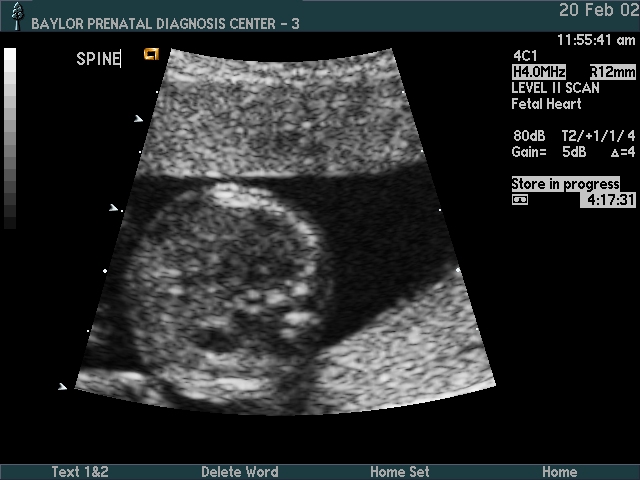
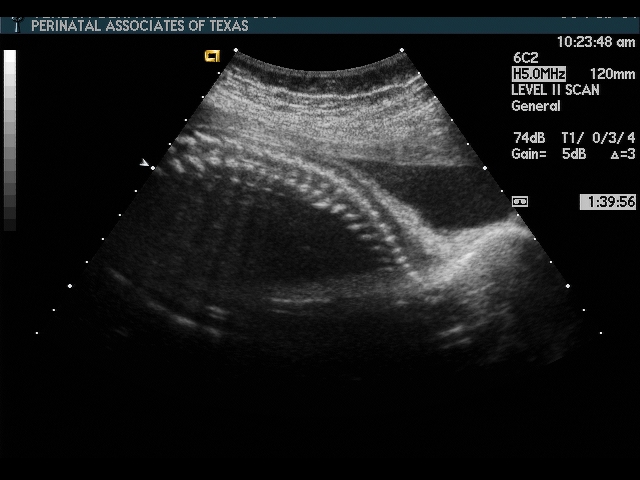
Spinal processes should be visible, in a compact triangle (elongation of the processes suggests a skewed view)
Stomach should be visible
The hepatic portion of the umbilical vein as it curves into the hepatic vein should be visible (if the umbilical vein extends to the abdominal wall, the view is too low)
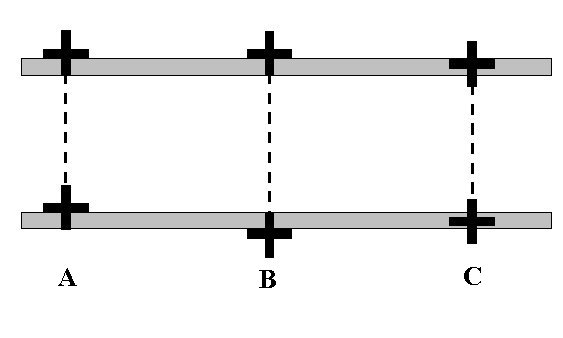
Measure circumferentially around the outer edge of the skin. Do not move the calipers in to the ribs, nor the spine. This is a measurement at the skin level.