

Authors
Keely Coxon, MD
Dawn DeWitt, MD
In this module
Peripheral nerves

- Role: Carry sensory and motor information between the brain/spinal cord (central nervous system (CNS)) and the rest of the body.
- Each peripheral nerve is individually myelinated, produced by Schwann cells (vs. oligodendrocytes in CNS).
Types of peripheral nerves
- Motor nerves*
- Sensory nerves*
- Autonomic nerves
- Note
Signal movement of muscles under voluntary control. This includes skeletal muscle, which allows us to conduct everyday activities like walking, holding objects, and chewing.
Relay sensations of pain, temperature, and touch from the body back to the brain.
Control the involuntary actions of muscles and organs. The autonomic nervous system regulates breathing, digestion/GI motility, cardiac pacemaker cells, and certain glandular secretions.
What is peripheral neuropathy?
Dysfunction of peripheral nerves, generally resulting from damage to the axon and/or myelin sheath.
Peripheral neuropathies are usually divided into two categories:
- Guillain-Barré syndrome.
- Chronic inflammatory.
- Demyelinating polyneuropathy (CIDP).
- Diabetic neuropathy.
- Toxin exposure (including ETOH, drugs).
Common exam findings
- Weakness.
- Muscle atrophy.
- Changes in sensation:
- Pain.
- Paresthesias.
- Loss of sensation.
- Decreased or absent deep tendon reflexes (DTRs).
Principle causes of peripheral neuropathy
- Autoimmunity (inflammatory demyelinative polyradiculoneuropathies).
- Vasculitis (connective tissue diseases).
- Systemic illness (diabetes, uremia, sarcoidosis, myxedema, acromegaly).
- Cancer (paraneoplastic neuropathy).
- Infections (diphtheria, leprosy, lyme disease, AIDS, herpes zoster).
- Dysproteinemia (myeloma, cryoglobulinemia).
- Nutritional deficiencies and alcoholism.
- Compression and trauma.
- Toxic industrial agents and drugs.
- Inherited neuropathies.
Pathophysiology of peripheral neuropathy
It is useful to classify peripheral neuropathies as mononeuropathies (for example, carpal tunnel syndrom) or polyneuropathies (such as diabetic neuropathy).
- Segmental demyelination
- Wallerian degeneration
- Axonal degeneration
- Degeneration of myelin sheath; spares axon.
- May present unilaterally or bilaterally (symmetric).
- E.g., Guillain-Barre syndrome (axonal neuropathy in severe cases); Charcot-Marie-Tooth disease; MGUS-related neuropathy.
- Focal mononeuropathy caused by direct trauma to nerve (e.g., compression, lesion, infarction); axon begins to degenerate distal to insult.
- Most often these are length dependent (the signs and symptoms are most prominent in the lower extremities compared to the upper extremities).
- A.k.a. “dying back” phenomenon; begins distally and progresses in a proximal direction.
- Generally presents as symmetric polyneuropathy with noticeable weakness.
- E.g., diabetic polyneuropathy, HIV- and HCV-related neuropathy.
Note
Most common causes of adult-onset neuropathy in developed nations: Diabetes and alcoholism. Thirty to 40 percent of peripheral neuropathies are idiopathic, especially in older patients with mild symptoms.
Diagnostic studies in peripheral neuropathy
The AAN guideline says the highest-yield studies are fasting blood sugar, B12 level, and SPEP.
Helps distinguish a primary muscle disorder (myopathy) from neuropathy.
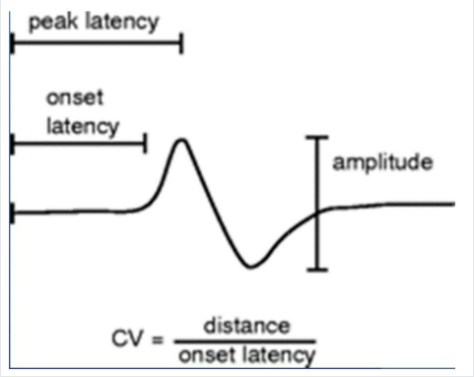
- Helps distinguish axonal processes from demyelinating.
- Axonal = decreased amplitude of action potential.
- Demyelinating = slowed conduction velocity.
Less-commonly done, but can help with definitive diagnosis.
CSF can be useful in diagnosing certain neuropathies, especially inflammatory.
- CBC: WBC [inflammation/infection], anemias.
- CMP: metabolic derangements.
- ANA.
- CRP.
- ESR.
- TSH.
- A1C.
- B12.
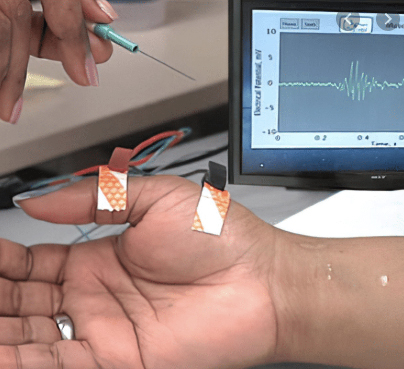
Electromyography

Axonal vs. demyelinating neuropathies
| Axonal Neuropathies | Demyelinating Neuropathies | |
|---|---|---|
|
Etiology |
|
Inflammatory examples
Hereditary example
|
|
Pathophysiology |
Direct insult to nerve axon results in degeneration distal to the site of injury (“Wallerian degeneration”). May also involve myelin sheath. |
Myelin facilitates more rapid conduction of nerve impulses demyelinating processes block or slow normal conduction velocity. |
|
Diagnosis |
|
History
Clinical course
EMG/NCS
|
|
Management |
Can often be treated by addressing the source of the axonal damage. |
|
Image credits
Unless otherwise noted, images are from Adobe Stock.