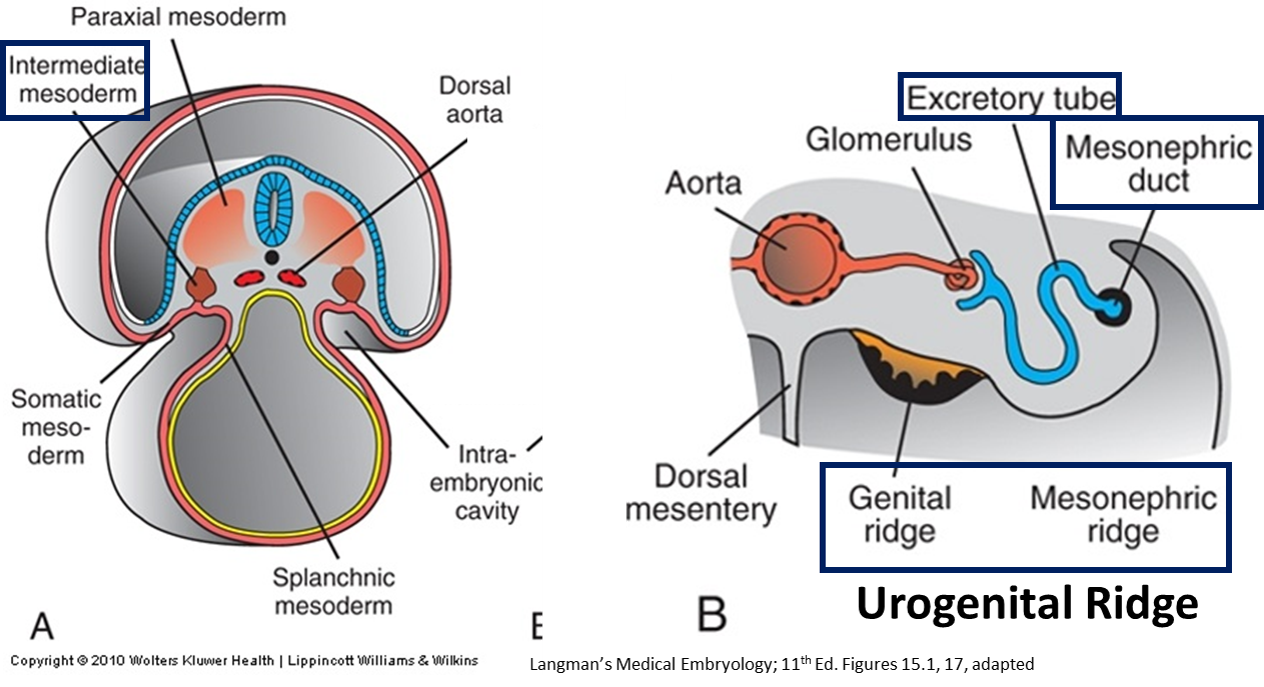

The nephrogenic cord (from intermediate mesoderm) forms 3 different sets of kidneys in a temporal (early to late) and spatial (cranial to caudal) sequence.
- Tubules (nephrons) form at 4 weeks in cervical region, 1 per body segment
- Degenerates! THE END.
- Forms interim kidney in thoracic region
- S-shaped mesonephric/excretory tubules, 3–4 per body segment connect temporary mesonephric kidney to a longitudinal collecting duct: the mesonephric duct.
- Most of the mesonephric kidney degenerates by the end of the second month of development
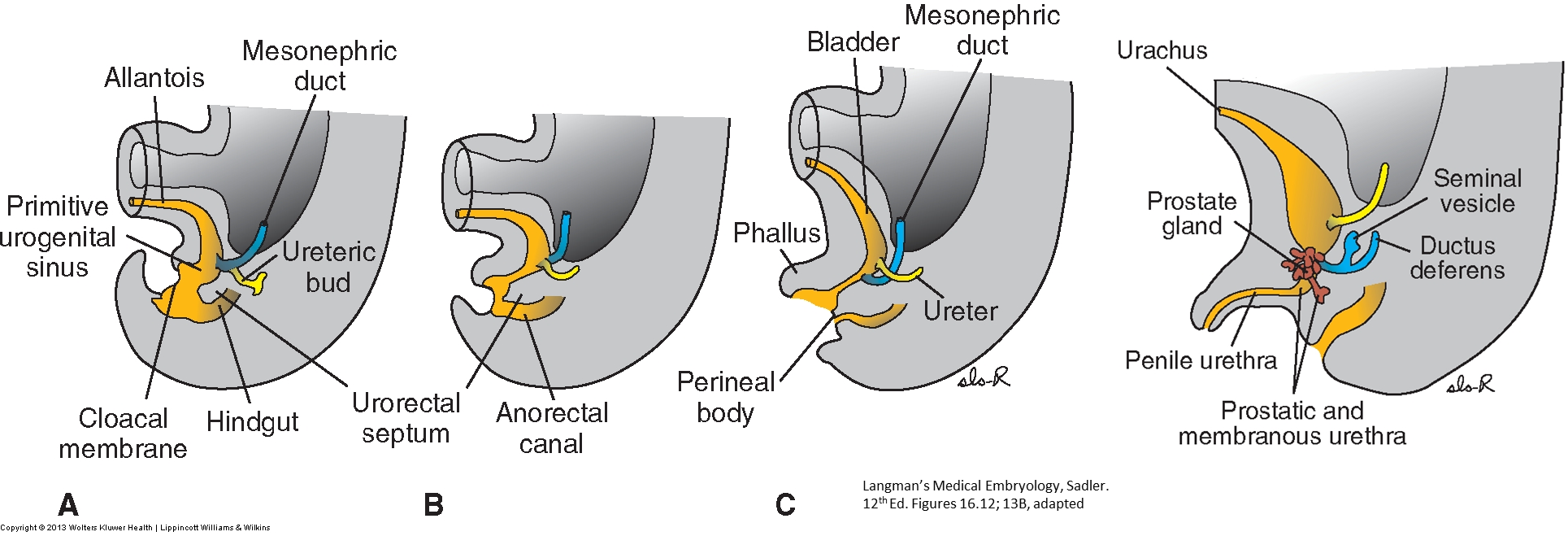
- Mesonephric (Wolffian) duct persists in the adult, becoming sperm-carrying tubes of male reproductive tract (ductus deferens, ejaculatory ducts, epididymis, and efferent ductules); is vestigial in females
The functional fetal and adult kidney
-
- Develops from intermediate mesoderm in pelvic region, begins development around Week 5
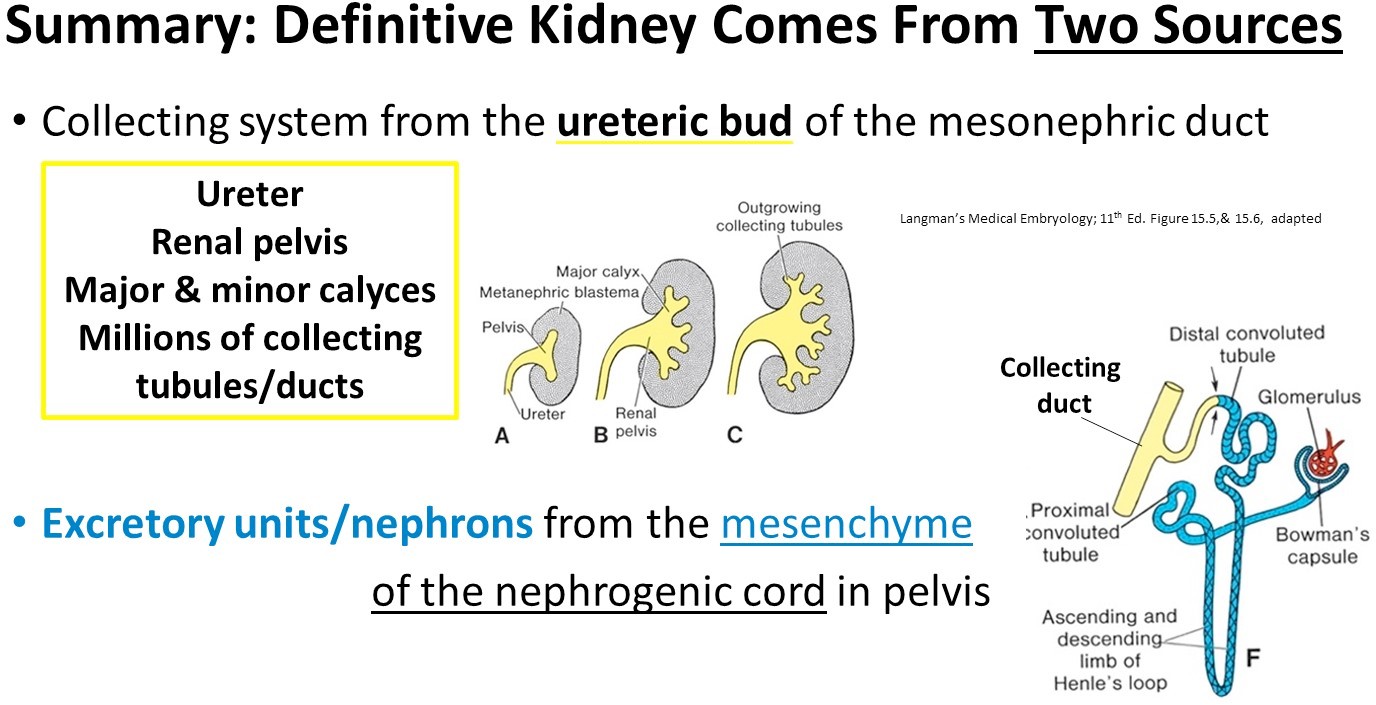
- Collecting ducts develop from ureteric bud
- Buds off of mesonephric duct into the metanephric mesenchyme/mesoderm
- Divides into smaller branches (12 orders): Major and minor calyces, and collecting ducts
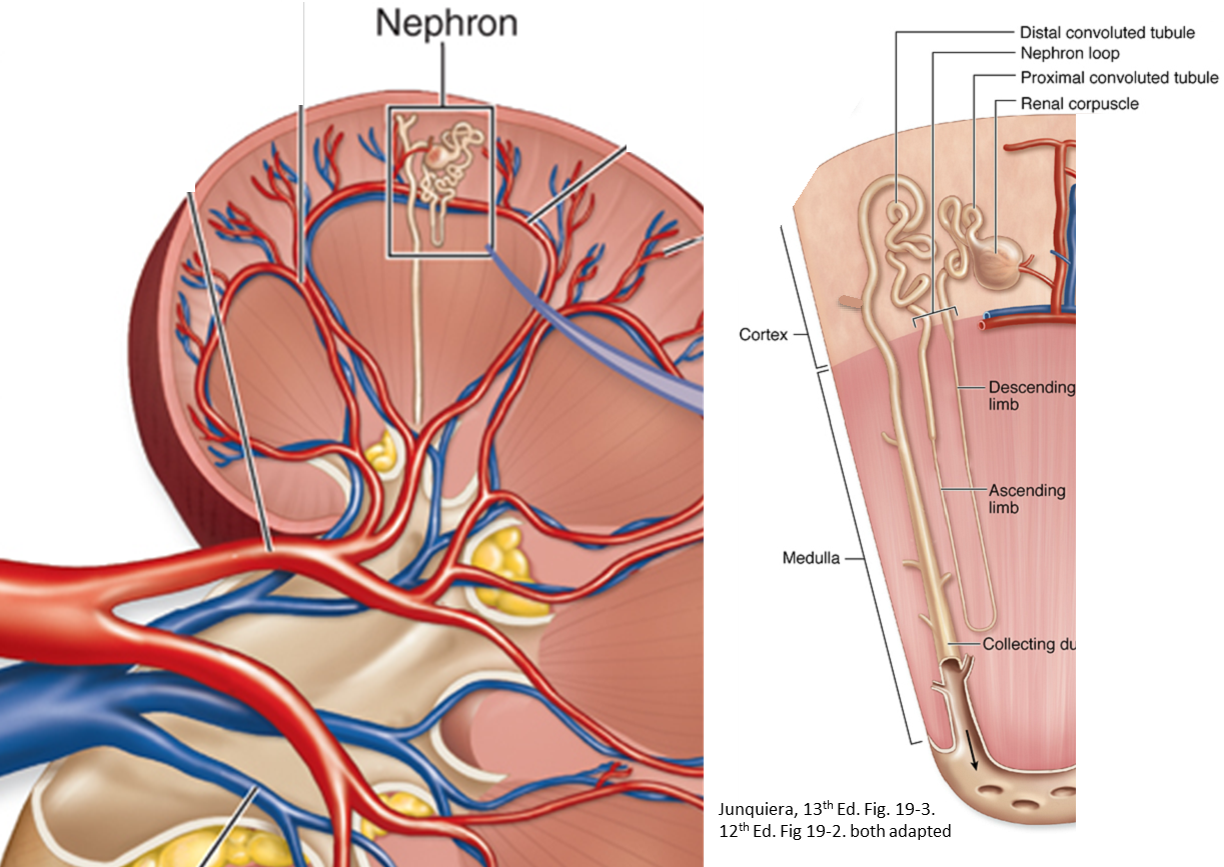
- Excretory units (nephrons) develop from metanephric mesoderm by forming caps over the collecting ducts
- Glomerular capillaries associate with these nephrons medially; distally, the tubules link the Bowman’s capsule to the collecting unit, establishing the proximal and distal convoluted tubules and the Loop of Henle
- About 1 in 750 people lack one kidney because the ureteric bud has degenerated early on one side, failing to induce the formation of nephrons in the nephrogenic cord.
- During the second half of development (10th week to 9th month), the metanephros is functional and the fetus produces urine. The fetus urinates this into the amniotic sac.
- Then, the fetus drinks the amniotic fluid, reabsorbing the contained urea through the intestine into the blood and excreting it across the placenta.
- By urinating into the amniotic sac and then drinking, the fetus can continually renew the amniotic fluid and regulate the volume of this fluid. The fetus controls the volume of the amniotic fluid.
- At birth, too little amniotic fluid in the amniotic sac (oligohydramnios) can indicate non-functioning kidneys, whereas too much amniotic fluid (polyhydramnios) can signify brain damage or a blocked esophagus.
- The kidneys are markedly lobed at birth, being covered externally with bulges. Each lobe represents the renal tissue around a single minor calyx and its branches. The lobes disappear during infancy as the nephrons grow bigger, but not in number.